Article Text

Statistics from Altmetric.com
Summary
When laparoscopic surgery was introduced for the treatment of women with early cervical cancer by Dargent and Querleu, this technique always included a vaginal phase. Transvaginal transsection and closure of the vaginal cuff seal off tumor cells as initially described by Schauta. Alternatively, in radical abdominal surgery Wertheim and his followers use a rectangular clamp for intracorporeal colpotomy to avoid tumor cell contamination of the peritoneal cavity (1).
Due to lack of experience in vaginal surgery laparoscopic surgeons have omitted the vaginal phase and have developed techniques of total laparoscopic radical hysterectomy or robotic radical hysterectomy with inherent insertion of uterine manipulators and colpotomy at the manipulators’ rim. Thus, the pelvic peritoneum is exposed to cervical tumor and potentially can be contaminated by vital tumor cells (2).
Since the publication of the prospective randomized Laparoscopic Approach to Cervical Cancer (LACC) trial in 2018, minimally invasive radical hysterectomy has become a very controversial topic (3). The LACC study and other subsequent published analyses showed that minimally invasive radical hysterectomy was associated with lower rates of disease-free survival and overall survival compared with open abdominal radical hysterectomy. In particular, the rate of loco-regional recurrences was four times lower in patients following abdominal surgery.
In our surgical technique of vaginal assisted laparoscopic radical hysterectomy (VALRH), the laparoscopic and vaginal approach are combined, avoiding the use of any uterine manipulators and always creating a tumor-covering vaginal cuff transvaginally (4). VALRH comprises three steps: comprehensive laparoscopic staging and dissection of rectovaginal and vesicovaginal spaces (Figures 1 and 2), creation of a tumor-adapted vaginal cuff vaginally, and laparoscopic transsection of parametria. Over a period of 25 years we have avoided manipulator use and have sealed off cervical cancer cells by transvaginal closure of the vaginal cuff. Prospectively collected actual data on 389 consecutive patients with a risk profile comparable to the LACC cohort, with a median follow-up period of 10 years, prove recurrence-free and overall survival is identical to the open surgery patients in LACC (4).
Overwiev of laparoscopic dissection of the recto-vaginal space. This step is done after pelvic lymph node dissection and before proceeding with the vaginal part. The uterus and rectum are held under tension to make access to the recto-vaginal septum easier.Figure 2

{kind=link}
{kind=link}
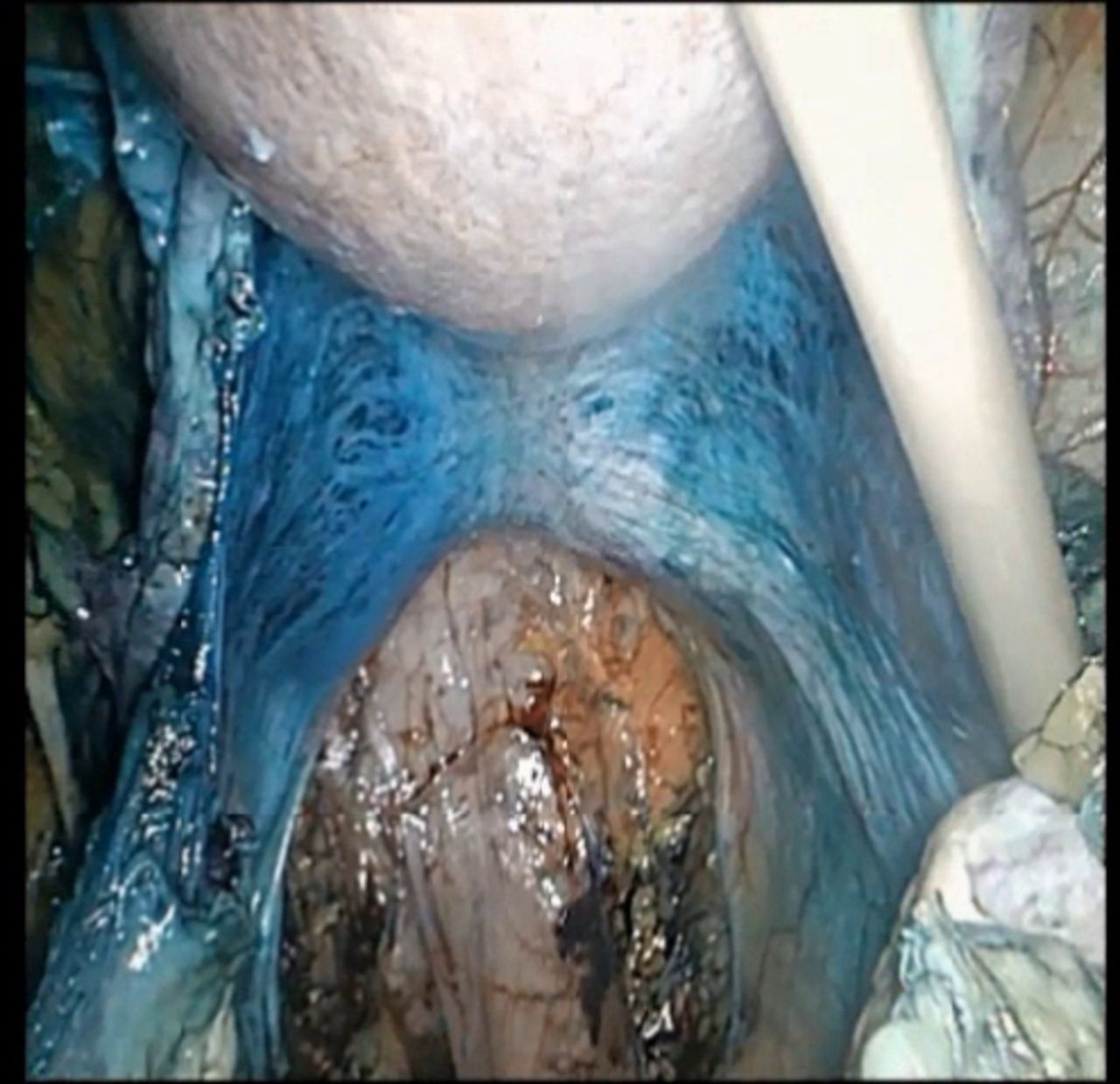
Overview of laparoscopic dissection of the vesicovaginal space. This step is done after pelvin lymph node dissection and before proceeding with the vaginal part. The uterus and the bladder are hold under tension to make the access to the vesicovaginal septum easier
In this video clip (Video 1) we demonstrate the transvaginal part of VALRH: we name the special instruments used and describe the technique step by step; and mention the complications which can be encountered and provide on how to avoid them.
Footnotes
Contributors CK and AP are responsible for planning of the video, the surgery and the writing of the abstract. VS and AS did the editing of the video file.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information