Article Text

Statistics from Altmetric.com
Case presentation
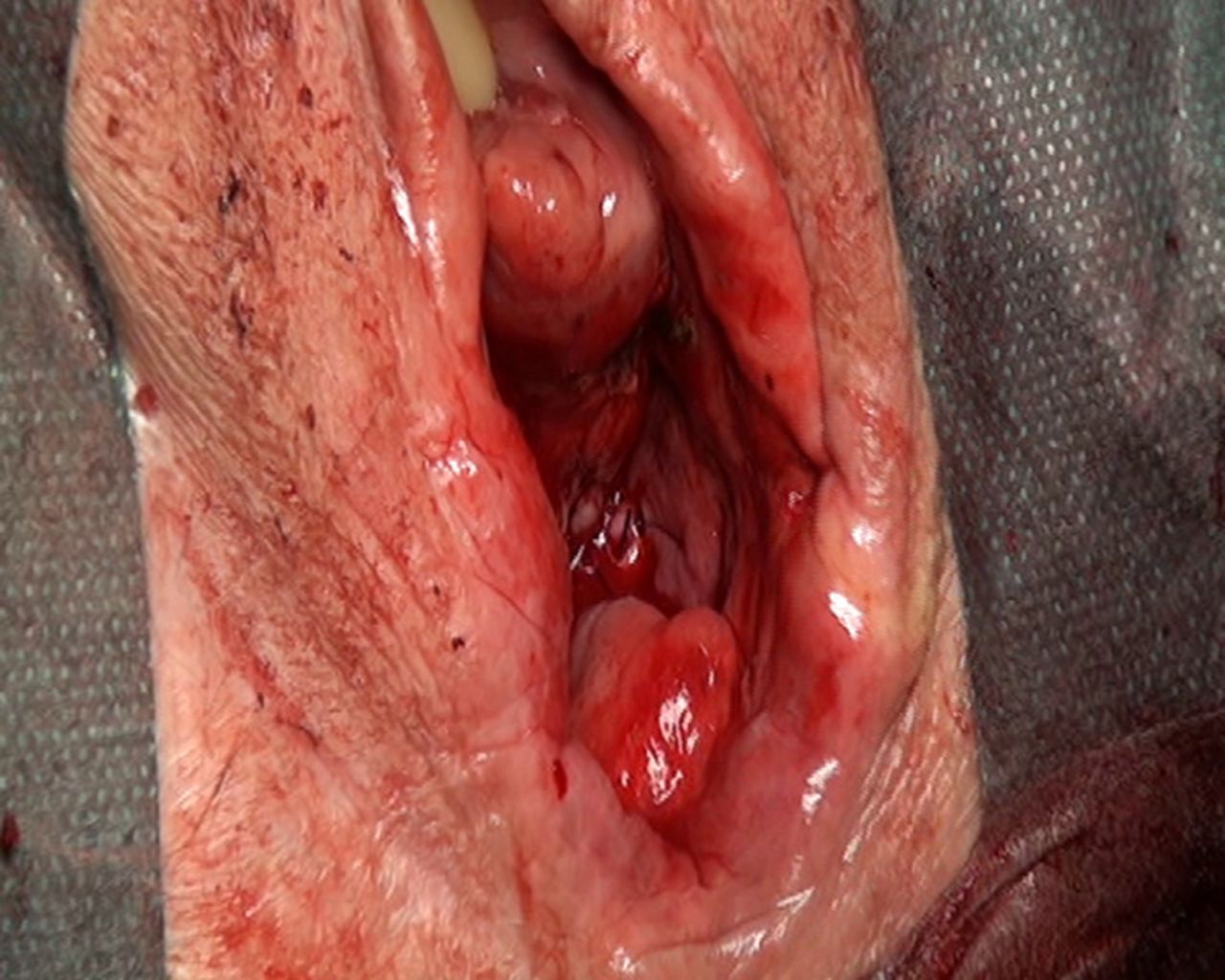
An 81-year-old woman (gravida 2, para 2) was referred on April 2019 to the Gynecologic Oncology Unit of San Gerardo Hospital from another institution for symptomatic utero-vaginal prolapse and foul-smelling discharge with concomitant bleeding. The clinical examination revealed a stage IV utero-vaginal prolapse (cervix and uterus have both descended outside introitus) and concomitant friable velvet tumor involving almost all the anterior and lateral sides of the vaginal walls with no macroscopic infiltration of the atrophic cervix (Figure 1). She reported frequency of urination, with associated incomplete emptying of the bladder without urinary incontinence. Preoperative urodynamic evaluation demonstrated post-void residuals>150 mL. At presentation, her weight was 40 kilograms and she had evidence of nutritional deficiency. She had a history of chronic hypertension, recurrent urinary tract infections, and chronic venous insufficiency. The biopsy of the vaginal wall tumor performed prior to her presentation showed a moderately differentiated invasive squamous cell carcinoma. Pelvic evaluation was negative and no palpable groin nodes were present. Work-up included chest X-ray, urodynamic evaluation, a pelvic MRI, and PET/CT scan.

Locally advanced vaginal tumor and associated vaginal prolapse at presentation.
Dr Perego
Can you describe the MRI and PET/CT imaging results?
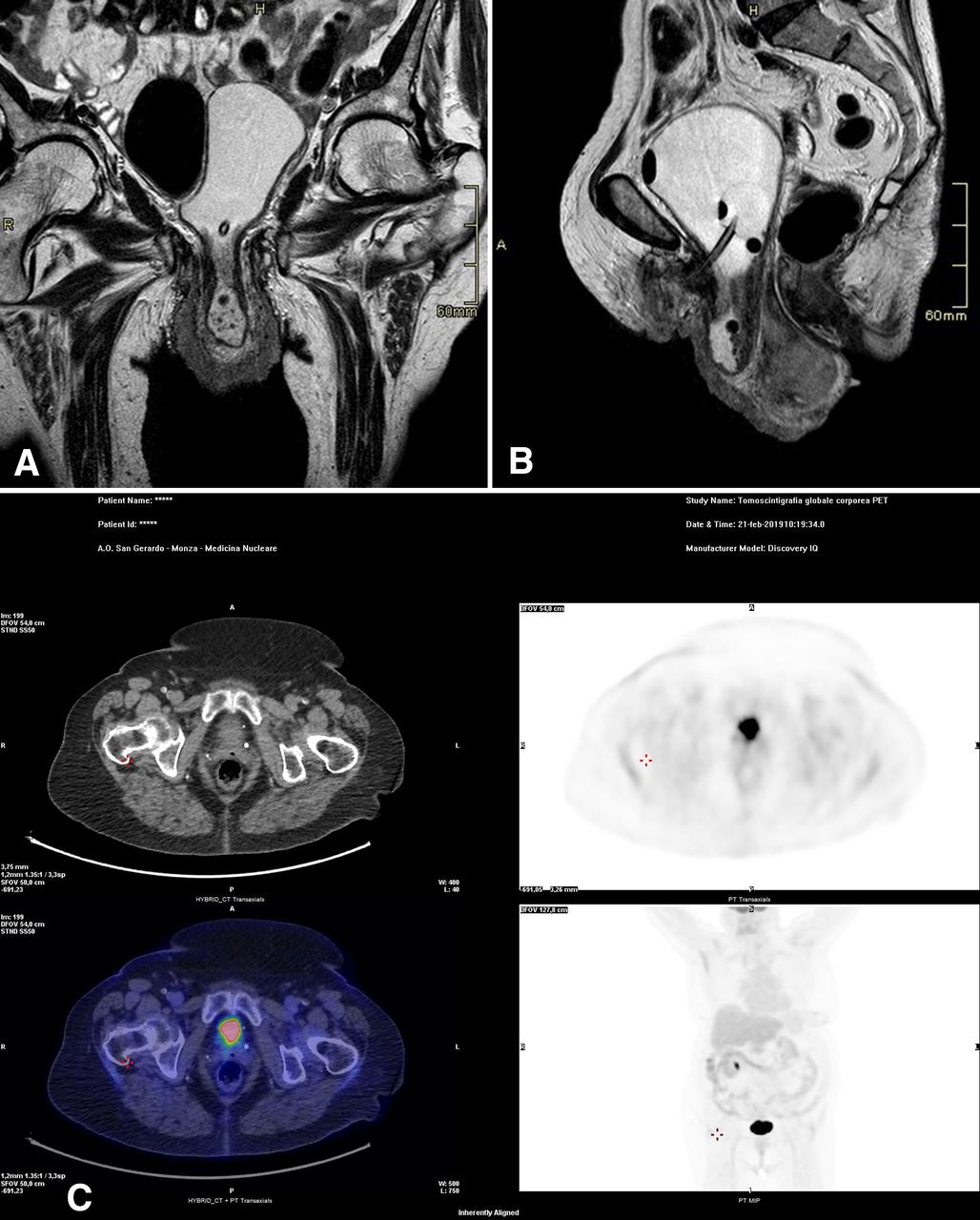
At MRI scan, the T1, T2-weighted, and DWI sequences and paramagnetic contrast (PROHANCE macrociclic, dose 2 mL/kg of the bodyweight) with a bladder catheter inside, showed a bladder floor prolapse (approximately 35 mm). Ureters were not visible in the pelvis most likely secondary to the advanced prolapse. Complete utero-vaginal stage IV prolapse with total vaginal eversion. The vaginal wall (total thickness 13 mm) was involved by the tumor presents as a rather homogeneous mass with high signal intensity infiltrating the vaginal mucosa from 6 o'clock to 3 o'clock. The hypointense ring of the submucosal and muscularis layer was intact.
The posterior vaginal pouch was occupied by the prolapsed uterus and both the ovaries. However, due to the advanced stage of prolapse, the topography and the anatomy of the uterus was completely subverted and was hard to clearly understand the presence of infiltration of the atrophic cervix from the vaginal tumor burden. Even with the artifacts of imaging in the presence of advance prolapse there was no apparent infiltration of the vescico-uterine space and/or urethral vaginal space. No suspicious groin and/or pelvic or aortic nodal metastasis were present. No free fluid. After reduction of the advanced prolapse, the contrast-enhanced PET/CT scan performed showed an avid 18F-fluorodeoxyglucose (FDG) uptake in the vulvar-vaginal region. No groin, pelvic, and/or aortic lymph nodesup-take was noted. There was no evidence of distant metastases (Figure 2).

(A, B) Para-coronal, and sagittal MRI T2-weighted images showing the advanced uterovaginal prolapse and the diffuse thickness of a large portion of the vaginal wall involved by tumor. (C) Fused positron emission tomography/computed tomography (PET/CT) images shows the hypermetabolic uptake in the vaginal wall, the maximum intensity projection (MIP) image, and the fused PET-images showing no distant metastasis.
Dr Buda
Given the MRI and PET/CT findings, what would be the decision and recommendations in the management of this patient?
The occurrence of primary carcinoma of the vagina is an uncommon condition, usually affecting elderly women, accounting for 1%–2%of all gynecologic malignancies, and therefore there is no consensus on optimal treatment.1The concurrence of vaginal cancer with irreducible uterine prolapse is even more rare. Usually, symptoms include vaginal bleeding, dysuria, and pelvic pain. Some important considerations should be discussed with thepatientwhen managing such a complex presentation.Patientsneed to understand that there is no consensus or standard of care regarding the management of vaginal cancer and concomitant severe prolapse. Treatment is always challenging, and options include radiotherapy, surgery, or palliative treatment.
External beam radiotherapy is associated with significant risk, and in the presence of associated advanced prolapse, organs such as the bladder or bowel that may be included in the cystocele or enterocele sac, may be more exposed to the field of radiation, thus increasing the associated complications, such as vesico-vaginal or entero-vaginal fistulas.22Vaginal radiotherapy is usually associated with fewer side effectscompared withexternal beam radiation. External beam radiotherapy combined with brachytherapy has an essential role in the curative treatment of primary vaginal cancer. Radiotherapy including brachytherapy is the treatment of choice for the majority ofpatientsas organ-sparing surgery with negative resection margins is difficult to achieve.3,43 4The American Brachytherapy Society recommends exclusive interstitial brachytherapy for cervical cancer cases, such as in the presence of bulky lesions, narrow vaginal apex, inability to enter the cervical ostium, extension to the lateral parametria, or to the pelvic sidewall, and lower vaginal extension.55However, there are no specific guidelines specifying how to deliver radiotherapy in complex cases such as the one we presented. Furthermore, if the prolapse is irreducible, as in this case, the vaginal radiotherapy may not be technically feasible without performing surgery.
Surgery represents the mainstay of therapy according to the prolapse stage and associated symptoms. However, the healing process after surgery, prior to radiation, may delay treatment of the cancer. In addition, not everypatientcan tolerate surgery due to an impaired medical condition.
The major challenges of surgery depend on the amount of vagina involved and the presence of paravaginal tissue and/or bladder floor involvement. The stage of prolapse represents another challenge since in the presence of the advanced stage, appropriate selection of the type of reconstructive technique is crucial to allow for adjuvant radiation therapy and to limit the surgical-associated morbidity. Transvaginal prosthetic-free procedures including non-obliterative techniques have shown some advantagescompared withmesh augmentation, including lower costs and morbidity.Finally, the surgical approach should be evaluated well through a multidisciplinary approach considering risk and benefit as it pertains to the clinical and anesthesia risks of thepatient. In this case, thepatientwas extensively counseled and the decision was made to proceed with a surgical approach followed by adjuvant brachytherapy in the event of positive vaginal margins.
Drs Frigerio & Milani
Please provide details regarding the surgical procedure
The day prior to surgery, bilateral ureteral stents were inserted by a cystoscopic approach. The goal of the surgery was to not only address the cancer, but to also treat concomitant pelvic organ prolapse and restore bladder function. Usually, the surgery requires the partial or complete radical colpectomy based on the extent of the tumor. In the case of cancer in the upper part of the vagina, hysterectomy and bilateral radical groin lymphadenectomy with or without pelvic lymph node dissection should be considered.44
Thispatientunderwent a transvaginal partial colpectomy with en bloc hysterectomy plus native-tissue repair with levator midline plication, to reduce associated morbidity. This was performed in order to preserve the vaginal viability and restore apical support. No lymph node dissection was performed in order to avoid post-operative morbidity in the absence of palpable enlarged groin nodes, or suspicious imaging. Blood loss was300 mLand the operative time was120 min. On final examination, there was evidence of adequate apical support with no narrowing of the residual vagina (Figure 3). The residual vaginal length was6 cmwith normal caliber from the hiatus to the apex (Pelvic Organ Prolapse Quantification system-POP-Q: Aa=-3, Ba=-3, C=-6,gh=3, pb=3, tvl=6, Ap=-3, Bp=-3, D=/). The post-operative course was uneventful and thepatientwas discharged on post-operative day 5.

Vaginal reconstruction at completion of surgery.
Reconstructive surgery is an option if a large portion of the vagina has been removed. Non-obliterative techniques for apical support include: sacrospinous ligament fixation, uterosacral ligament suspension, iliococcygeus fascia fixation, and levator myorrhaphy.5–7The latter involves levator ani muscles midline plication to which the vaginal cuff is fixed. Levator ani plication involves some theoretical advantagescompared withother native-tissue procedures. Para-rectal dissection is limitedcompared withboth sacrospinous and iliococcygeus fascia fixations. Moreover, it does not involve the risk of ureteral injury typical of uterosacral suspension. A limitation that should be noted is the risk of vaginal constriction. We chose the levator ani plication technique to avoid the narrowing of the vagina given the potential for adjuvant radiotherapy, reducing the risk of bleeding, and surgical complicationscompared withother apical procedures.8
Dr Jaconi
The surgical specimen consisted of a portion of vaginal wall measuring60×20×5 mmand the uterus measuring70×50×80 mm. On microscopic examination, the specimen showed a moderately differentiated, diffusely infiltrating, keratinizing squamous cell carcinoma, present at the surgical resection margins. Regarding extension to the uterus, the cervix appeared widely involved by the vaginal tumor burden, which had a maximum extension of70 mm, infiltrating the anterior side of the cervix with no extension on the underline cervical stroma. The rest of the uterus did not show particular alterations, with thin endometrial lining and uniform myometrium (Figure 4). No lymphovascular or perineural invasion was identified.
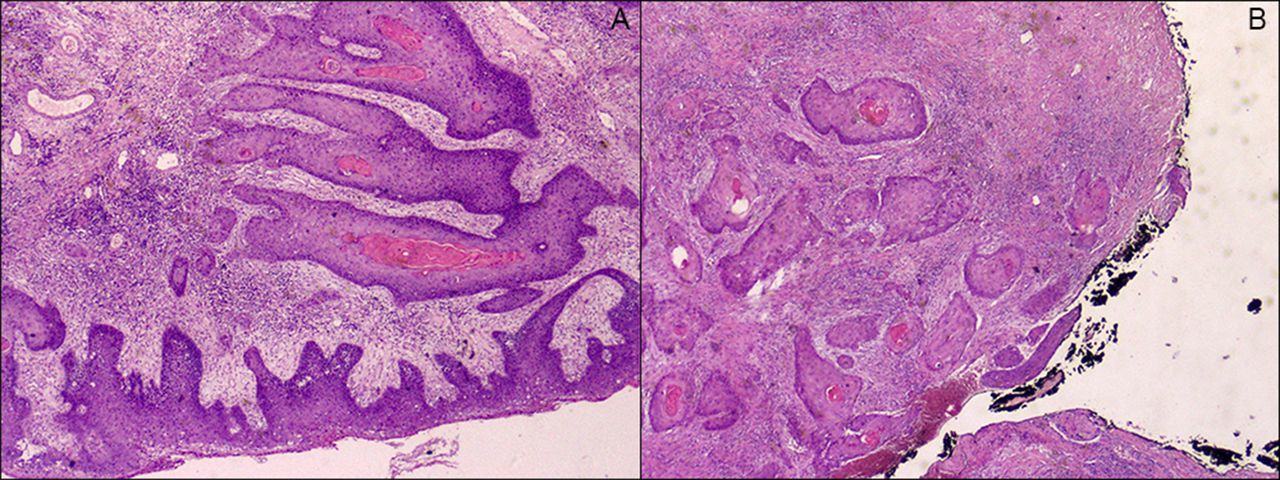
Histologic examination showing the extensive keratinizing squamous cell carcinoma (A), deeply infiltrating the vaginal wall and the anterior cervix extended to the surgical resection margin (B, marked with black ink). (hematoxylin and eosin (H&E) stain, 2x).
Dr Meregalli
Given the findings on the final surgical specimen what would be your suggested approach in this case?
In the presence of close or positive surgical margins, such as in this case, it is recommended to deliver vaginal brachytherapy. Surveillance is usually reserved in cases with negative margins. The main issue of concern to the radiation oncologists was the length of the residual vagina after the surgical intervention, presenting an overall length of6 cm. In this condition, the challenge lies in the insertion of the cylinder that contains the radiation source. Furthermore, thepatienthad a number of medical comorbidities and impaired nutritional status. Therefore, by using a shorter6 cm-long cylinder she underwent high-dose-rate (HDR) vaginal brachytherapy using a very small device with a low dose per fraction (4 Gy). A total dose of20 Gyinfivefractions was administered. No external beam radiotherapy was planned. The computed treatment planning has been optimized at each fraction by using a 3D technique with an optimal target coverage and sparing of organs at risk (bladder and rectum), carefully documented by the dose-volume histogram (DVH). (Figure 5)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A,B,C) High-dose rate (HDR) vaginal brachytherapy. The axial and coronal views of the 3D technique dose-volume histograms (DVH) showing the optimal target field and bladder rectum sparing. fused positron emission tomography/computed tomography (PET/CT) image shows a hypermetabolic mass in the vagina, the maximum intensity projection (MIP), and the fused PET/CT with no distant metastasis.
A clinical evaluation was performed at each brachytherapy fraction, without any acute toxicity noted. At the end of the treatment, thepatientwas slowly regaining weight with improvement of the general clinical conditions. After10months, she is alive without evidence of disease.
Dr Buda
Closing summary
Locally-advanced vaginal tumor with associated advanced prolapse is a rare condition. A surgical intervention when associated with irreducible utero-vaginal prolapse should be considered when thepatientis not suffering from major medical comorbidities and when the infiltrating tumor burden spares the urethra and/or bladder floor. Also considered when regional nodes are suspicious for disease. In such a rare condition, the multidisciplinary approach is critical. It is essential to not only appropriately address the cancer diagnosis but also, as in this case, the bladder and pelvic floor dysfunction. In addition, one must also prioritize quality of life for thepatient. Furthermore, when adjuvant brachytherapy is required, the vaginal reconstruction using the transvaginal levator ani plication provides a non-obliterative native-tissue reconstruction with adequate apical support. Based on limited literature on treatment options,1 6 8the vaginal surgical resection of the tumor and a well-defined modulated vaginal reconstruction followed by adjuvant brachytherapy seems a viable treatment option in thesepatients.
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Commissioned; externally peer reviewed.