Article Text

Abstract
The development of guidelines is one of the core activities of the European Society for Medical Oncology (ESMO) and European Society of Gynaecologial Oncology (ESGO), as part of the mission of both societies to improve the quality of care for patients with cancer across Europe. ESMO and ESGO jointly developed clinically relevant and evidence-based recommendations in several selected areas in order to improve the quality of care for women with ovarian cancer. The ESMO–ESGO consensus conference on ovarian cancer was held on April 12–14, 2018 in Milan, Italy, and comprised a multidisciplinary panel of 40 leading experts in the management of ovarian cancer. Before the conference, the expert panel worked on five clinically relevant questions regarding ovarian cancer relating to each of the following four areas: pathology and molecular biology, early-stage and borderline tumours, advanced stage disease and recurrent disease. Relevant scientific literature, as identified using a systematic search, was reviewed in advance. During the consensus conference, the panel developed recommendations for each specific question and a consensus was reached. The recommendations presented here are thus based on the best available evidence and expert agreement. This article presents the recommendations of this ESMO–ESGO consensus conference, together with a summary of evidence supporting each recommendation.
- ovarian cancer
- adjuvant treatment
- surgery
- pathology
- molecular biology
- recurrent disease
Statistics from Altmetric.com
Highlights
ESGO and ESMO organised a joint consensus conference on ovarian cancer to address clinically-relevant questions regarding pathology and molecular biology, early-stage and borderline tumours, advanced stage disease and recurrent disease.
Results of this consensus conference, including questions, recommendations and a summary of evidence supporting each recommendation, are detailed in this article.
Introduction
The development of guidelines recommendations is one of the core activities of both the European Society for Medical Oncology (ESMO) and the European Society of Gynaecologial Oncology (ESGO), as part of their mission to improve the quality of care for patients with cancer across Europe. The objectives of these recommendations are to improve and to harmonise the management of patients with ovarian cancer. ESMO and ESGO decided to jointly hold a consensus conference aiming at updating current knowledge relevant to the management of ovarian cancer.
Ovarian cancer is the leading cause of death among all gynaecological cancers in developed countries, with most patients presenting with advanced stage tumours, as defined by the spread of the disease outside the pelvis [International Federation of Obstetrics and Gynecology (FIGO) stage III and IV]. The estimated number of new ovarian cancer cases in Europe in 2012 was 65 538 with 42 704 deaths.1 More than two-thirds of patients are diagnosed at an advanced stage. More than 90% of malignant ovarian tumours are of epithelial origin, designated epithelial ovarian cancer (EOC). The most common and most lethal EOC is high-grade serous carcinoma (HGSC). Recent evidence suggests that most ‘extrauterine’ HGSCs arise from the fallopian tube and recommendations are presented for designating the site of origin of these neoplasms based on our current knowledge of the site of origin and precursor lesions.
Responsibilities
These recommendations are a statement of evidence and consensus of the authors regarding their views of currently accepted approaches to diagnosis and treatment. They do not include any economic analysis of the strategies. Any clinician applying or consulting these recommendations is expected to use independent medical judgement in the context of individual clinical circumstances to determine any patient’s care or treatment. These recommendations make no representations or warranties of any kind regarding their content, use or application, and the authors disclaim any responsibility for their application or use in any way.
Methods
Two consensus conference chairs (N. Colombo, D. Querleu) were appointed. The consensus panel comprised 40 experts in the management of ovarian cancer and included representation from ESMO and ESGO (see Appendix). Each panel member was assigned to one of four working groups (WGs), with a WG chair and co-chair appointed for each group. Each WG was assigned a subject area as follows:
Pathology and molecular biology (Chair: W.G. McCluggage; Co-Chair: I. McNeish)
Early-stage and borderline tumours (Chair: P. Morice; Co-Chair: I. Ray-Coquard)
Advanced stage disease (Chair: S. Pignata; Co-Chair: I. Vergote)
Recurrent disease (Chair: A. du Bois; Co-Chair: J. Ledermann)
The methodology and medical writing support was provided by F. Planchamp and each WG was assisted by a fellow (T. Baert, I. Belaroussi, A. Dashora, S. Olbrecht). These five individuals did not participate in the voting of consensus recommendations.
The consensus conference was held on April 12–14, 2018 in Milan, Italy. Before this consensus conference, the WG chairs were asked to identify five clinically relevant questions for each subject area/WG, giving a total of 20 clinically relevant questions.
To ensure that the recommendations were evidence-based, the literature was reviewed. A systematic literature review of the studies published between January 2007 and December 2017 was carried out using the Medline database (see Section 1 of supplementary data, IJGC, available online). The literature search was limited to publications in English. Priority was given to high-quality systematic reviews, meta-analyses and randomised controlled trials (RCTs), but lower levels of evidence were also evaluated. The reference list of each identified article was reviewed for other potentially relevant papers. Each WG was responsible for reviewing the relevant literature in order to draft preliminary recommendations relating to each of their assigned questions.
Supplemental material
During the conference, in parallel sessions, the four WGs discussed and reached agreement on recommendations relating to each of their assigned questions. Recommendations from each group were then presented to the entire panel of experts, where they were discussed and modified as required. An adapted version of the ‘Infectious Diseases Society of America-United States Public Health Service Grading System’2 was used (see Table 1) to define the level of evidence (LoE) and grade of recommendation (GoR) for each of the recommendations proposed by the group. Finally, members were asked to vote on each recommendation; members were allowed to abstain from voting in cases where they either had insufficient expertise to agree/disagree with the recommendation, or if they had a conflict of interest that could be considered as influencing their vote. The recommendations from this consensus conference, together with a summary of evidence supporting each recommendation, are detailed in this article. A summary of all recommendations is included in supplementary Table S1, IJGC, available online.
Supplemental material
Levels of evidence and grades of recommendation (adapted from the Infectious Diseases Society of America-United States Public Health Service Grading System*)
Results
Pathology and Molecular Biology
1. How to determine the site of origin of extrauterine high-grade serous carcinoma?
Despite growing evidence in support of the fallopian tube origin of a significant majority of extrauterine HGSCs,3–5 there continues to be disagreement on primary site assignment. This has implications for cancer registration and epidemiological analyses, and results in differences in the staging of low-stage disease.6 Continuing doubt on origin perpetuates the belief that there is a true biological entity of ‘primary peritoneal HGSC’, currently defined in the 2014 World Health Organization (WHO) classification7 as a disease of exclusion, to be designated only in cases with no gross or microscopic evidence of mucosal disease in either the tubes or the ovaries. Most significantly, continuing skepticism regarding the tubal origin is an obstacle to studying the impact of ovary-conserving preventative strategies that have potential to reduce HGSC incidence and mortality.
Studies on the origin of sporadic HGSC in the past have been hampered by its presentation with disseminated disease, technical challenges in performing molecular studies on formalin-fixed paraffin-embedded tissues and incomplete tubal examination; complete tubal sampling using detailed Sectioning and Extensively Examining the FIMbriated End (SEE-FIM) protocols is an essential prerequisite for identifying and sampling the microscopic precursor lesion of HGSC, serous tubal intraepithelial carcinoma (STIC). While STIC is reported to be present in 11–61% of HGSC cases, reports on low-stage and optimally examined cases clearly demonstrate that virtually all contain STIC or small microscopic tubal HGSC.8–11 These studies also show that examples of single-site disease are always tubal and never ovarian. Furthermore, while ovarian involvement in HGSC is typically bilateral, as is common in metastasis to a paired organ, tubal involvement is unilateral in the majority of cases.12 These observations are supported by detailed molecular analysis demonstrating shared TP53 mutation between STIC and HGSC, and that the majority of mutational and copy abnormalities seen in HGSC are also identified in accompanying STIC.13 Clonal evolution studies demonstrate the same result14 15 but also show that, in advanced cases, intraepithelial tubal metastasis can produce lesions indistinguishable from STIC, further demonstrating the futility of studying advanced HGSC to answer questions about its origin. What these and other studies have demonstrated irrefutably is that, despite being widely disseminated at presentation in the majority of cases, HGSC arises from a single precursor clone, and there is no molecular evidence of multifocal origin.16 17 A proposal for primary site assignment in extrauterine HGSC is recommended for reproducible categorisation (see Table 2), with its basis in scientific evidence in favour of traditional beliefs7 18; this has been recommended for use in international ovarian cancer pathology reporting guidelines.19 This evidence also forms the basis for recommendations on uniform staging of low-stage HGSC in cases that are left to the pathologist’s and clinician’s discretion in the current FIGO system,20 21 resulting in potential for identical cases to be staged differently.6 It should be emphasised that these criteria are only to be used for HGSC and not for other histological types of EOC.
Criteria for assignment of primary site in extrauterine HGSC
Recommendation 1.1
A large majority of extrauterine HGSCs arise in the fallopian tube from STIC. SEE-FIM sectioning of both fallopian tubes should be carried out in all cases of extrauterine HGSC where the tubes are grossly normal, and also in risk-reducing prophylactic surgery specimens.
Level of evidence: III
Strength of recommendation: A
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
Recommendation 1.2
Extrauterine HGSC can only be assigned as ovarian in origin if both fallopian tubes are grossly normal, and histologically contain no mucosal disease following examination using a SEE-FIM protocol.
Level of evidence: III
Strength of recommendation: A
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
Recommendation 1.3
Cases in which HGSC is present in the endometrium and the tube/ovary are very likely to represent a primary at one site with metastasis to the other; these are very unlikely to represent synchronous independent neoplasms.
Level of evidence: V
Strength of recommendation: A
Consensus: 97.5% (39) yes, 2.5% (1) no, 0% (0) abstain (40 voters)
Recommendation 1.4
The distinction between primary endometrial and primary tubal/ovarian HGSC requires assessment of a constellation of pathological features; negative wild-type 1 (WT1) staining favours an endometrial primary, but this is not always definitive.
Level of evidence: V
Strength of recommendation: A
Consensus: 92.5% (37) yes, 0% (0) no, 7.5% (3) abstain (40 voters)
Recommendation 1.5
The use of uniform criteria is important in site assignment in extrauterine HGSC for cancer registry and epidemiological reasons. The use of International Collaboration on Cancer Reporting (ICCR) and College of American Pathologists (CAP) guidelines is recommended.
Level of evidence: V
Strength of recommendation: A
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
Recommendation 1.6
Correct and uniform use of site assignment criteria is particularly important for accurate staging of early HGSC.
Level of evidence: III
Strength of recommendation: A
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
Recommendation 1.7
STIC should count as a disease site for staging purposes; for example, a case with a STIC and HGSC confined to the ovary should be staged as stage IIA fallopian tube HGSC.
Level of evidence: IV
Strength of recommendation: A
Consensus: 95% (38) yes, 0% (0) no, 5% (2) abstain (40 voters)
Recommendation 1.8
True primary peritoneal HGSC is extremely rare.
Level of evidence: IV
Strength of recommendation: A
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
Recommendation 1.9
Multifocal origin of extrauterine HGSC is exceptionally rare and thus HGSC currently staged as IB should be considered as stage IIA.
Level of evidence: IV
Strength of recommendation: A
Consensus: 95% (38) yes, 5% (2) no, 0% (0) abstain (40 voters)
2. How to identify tumours that will respond to targeted therapies, including poly(adenosine diphosphate-ribose) polymerase inhibitors and immune checkpoint inhibitors?
The targeted therapies that are under investigation include antiangiogenic agents, poly(adenosine diphosphate-ribose) polymerase (PARP) inhibitors, hormone receptor modulators and immune checkpoint inhibitors. Bevacizumab, an antivascular epithelial growth factor (anti-VEGF) monoclonal antibody has shown positive results in first-line therapy with standard chemotherapy and also in both platinum-sensitive and platinum-resistant relapsed disease, with improved progression-free survival (PFS) in various large RCTs.22–25 Improvements in overall survival (OS) have been harder to demonstrate and are currently limited to a retrospective analysis of high-risk patients within the ICON7 trial.22 Although therapy targeting VEGF has become the standard of care in tubo-ovarian carcinomas as well as other solid malignancies, attempts to identify predictive molecular biomarkers for efficacy have failed to identify any that could help oncologists decide who should and more importantly, who should not, receive VEGF-targeted therapies, including bevacizumab.26
Angiogenic markers, such as CD31 expression, microvessel density and tumour VEGF-A levels, may provide prognostic information in recurrent/persistent EOC, and were identified in a retrospective analysis of the Gynecologic Oncology Group (GOG) 218 study as potential predictive biomarkers,27 but further prospective evaluation will be required. Another study showed a discriminatory signature comprising mesothelin, FLT4, α-1 acid glycoprotein (AGP) and cancer antigen 125 (CA125) as potentially identifying those patients with EOC more likely to benefit from bevacizumab.28 A potential role of combined values of Ang1 and Tie2 as predictive biomarkers for improved PFS in bevacizumab-treated patients with EOC has also been suggested. However, these findings need to be validated in larger trials.29 Currently, only clinical biomarkers (including stage, debulking status and presence of ascites) appear to have predictive utility in selecting patients for first-line treatment with bevacizumab, and thus prospective studies evaluating predictive biomarkers of bevacizumab benefit are urgently required.
At the time of diagnosis, ∼50% of EOCs may exhibit defective DNA repair via homologous recombination (HR) due to genetic and epigenetic alterations of HR pathway genes.30 Defective HR is an important therapeutic target in EOC as exemplified by the efficacy of platinum analogs in this disease, as well as the advent of PARP inhibitors that exhibit synthetic lethality when applied to HR-deficient cells. PARP inhibitors, such as olaparib, niraparib and rucaparib, are being utilised in the clinic to manage recurrent EOCs that display defects in the HR repair pathway. However, PARP inhibitors also show significant clinical benefit in patients without demonstrable defects in known HR genes. Various studies validated this and extended the usefulness of PARP inhibitors in the treatment setting beyond BRCA-mutated tumours.31 32
The strongest clinical evidence for the use of PARP inhibitors comes from patients with germline or somatic mutations in BRCA1 or BRCA2, both as single-agent therapy and as maintenance following response to platinum chemotherapy in the first-line33 and relapsed34–36 settings. Rucaparib also has robust activity as single-agent therapy in relapsed BRCA-mutated HGSC,32 and the ARIEL2 study32 demonstrated that tumours harbouring mutations in RAD51C alterations are BRCA-like [high genomic loss of (LOH)] and responded to rucaparib at very similar rates to BRCA-mutated disease. However, attempts to identify robust predictive biomarkers of response to PARP inhibitors in HGSC beyond key HR gene mutations have proven difficult. The ARIEL2 study32 utilised genome-wide LOH as a potential predictive biomarker, and showed that BRCA WT/LOH high tumours did indeed have higher response rates and improve PFS compared with BRCA WT/LOH low, but lower than BRCA-mutated. However, attempts to use LOH as a predictive marker in the maintenance setting were less successful. The ARIEL3 study37 evaluated rucaparib versus placebo as maintenance treatment in patients with recurrent platinum-sensitive cancer and found rucaparib maintenance treatment significantly improved PFS versus placebo in the nested BRCA-mutated and HR deficiency (HRD) cohorts and in the overall intention-to-treat (ITT) population. PFS was improved with rucaparib maintenance treatment versus placebo in patients with BRCA WT EOC (LOH high and LOH low) as well. The NOVA study38 utilised a different algorithm to identify potential HRD tumours and again found that, in patients who had responded to platinum in the relapse setting, the median PFS was significantly longer among those receiving niraparib than among those receiving placebo, regardless of the presence or the absence of germline BRCA mutations or HRD status. Thus, in the maintenance setting, response to platinum chemotherapy remains the most robust predictive biomarker for PARP inhibitor benefit.
A major limitation of the current HR assays is that they are largely insensitive to reversion of HRD, which may occur on development of resistance to platinum and PARP inhibitors. True functional assays of HR function exist, but they require the cancer specimen to be exposed to some form of DNA damage, which precludes use of formalin-fixed, paraffin-embedded specimens, increases the technical complexity, and limits the reproducibility of these assays. Overall, there is currently no prospectively validated biomarker of HRD that has been incorporated into clinical practice, and this remains an active area of investigation.39
Bowman et al40 demonstrated that higher levels of oestrogen receptor (ER) expression in EOC resulted in disease stabilisation and CA125 response after treatment with the aromatase inhibitor letrozole, and suggested the presence of an endocrine-sensitive group that could be targeted in future studies. Similar results were later published by other groups, suggesting that ER/progesterone receptor (PR) expression status may be a predictive biomarker for hormonal therapy.41 42 There are no positive prospective randomised data for the use of hormone therapies as alternatives to chemotherapy or as maintenance therapy in first-line or recurrent disease, even in low-grade serous carcinoma (LGSC). RCTs incorporating hormone therapy are required, especially in LGSC. Prospective validation of ER score as a predictive biomarker is also required, as there is no validated or universally used ER score in EOCs.
Recommendation 2.1
There are no validated predictive molecular biomarkers of bevacizumab benefit.
Level of evidence: IV
Strength of recommendation: A
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
Recommendation 2.2
PARP inhibitors have greatest activity in patients with BRCA1/2 mutations.
Level of evidence: I
Strength of recommendation: A
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
Recommendation 2.3
Testing for BRCA1/2 mutations is recommended for all patients with non-mucinous ovarian cancer.
Level of evidence: I
Strength of recommendation: A
Consensus: 95% (38) yes, 0% (0) no, 5% (2) abstain (40 voters)
Recommendation 2.4
Testing for mutations in other HR genes, in particular RAD51C/D, BRIP1 and PALB2, should be considered.
Level of evidence: III
Strength of recommendation: A
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
Recommendation 2.5
Current assays of HR function cannot be used to exclude patients from PARP inhibitor therapy.
Level of evidence: I
Strength of recommendation: A
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
Recommendation 2.6
Moderate-strong ER staining may be a predictor of response to hormone therapy.
Level of evidence: III
Strength of recommendation: B
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
Recommendation 2.7
There are currently no prospectively validated predictive biomarkers of response to immune checkpoint inhibitors that are specific to ovarian cancer.
Level of evidence: V
Strength of recommendation: A
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
3. How to identify patients with acquired/intrinsic resistance to chemotherapy?
Although most patients with HGSC initially respond to platinum-based chemotherapy, the large majority of patients will relapse. Thus, resistance to platinum-based treatment is common, with roughly 20% of women experiencing disease progression ≤6 months after completing a platinum-based regimen (previously classified as ‘platinum-resistant’ relapse) or who fail to respond at all to first-line treatment or relapse within 4–6 weeks after last platinum dose (previously classified as ‘platinum-refractory’).43 There have been many efforts over the years to develop accurate predictors of outcomes in patients treated with chemotherapy to help inform treatment decisions.44
Elucidation of why platinum resistance occurs and how it can be reversed or prevented is essential for improving survival. However, the WG unanimously agreed that there are no validated predictive biomarkers that can be used in clinical practice for determining likelihood of primary platinum-refractory or platinum-resistant disease.
It is widely accepted that most HGSCs (60–80%) show a good response to conventional platinum-based chemotherapy. However, low-grade serous, mucinous, clear cell and endometrioid ovarian carcinomas are considered to be less chemoresponsive and to have a different prognosis, although in many cases they present at an early stage, in contrast to HGSCs, which usually present at an advanced stage. The large majority of patients enrolled in clinical trials have HGSC histology and thus the results from these studies cannot automatically be applied to all histological types, where numbers recruited to all-comer studies are low and where there are generally very few specific studies.45
With better understanding of the molecular biology of EOCs, DNA damage repair through HR is known to play a vital role in contributing to genomic stability and preventing malignant transformation. Numerous studies have reported that mutation in BRCA1 or BRCA2 is a prognostic marker in EOC and concluded that patients with BRCA mutation, especially BRCA2, have better survival outcomes, which is likely to reflect increased response rates to platinum-based chemotherapy.46–48
Germline or somatic mutations in HR genes are present in up to one-third of EOCs, including both serous and non-serous histologies. In addition, Pennington et al49 looked at somatic and germline mutations in 13 HR genes (BRCA1, BRCA2, ATM, BARD1, BRIP1, CHEK1, CHEK2, FAM175A, MRE11A, NBN, PALB2, RAD51C, RAD51D). They concluded that somatic mutations in other HR genes have a similar positive impact on OS and platinum responsiveness as germline BRCA1/2 mutations. HR mutations were more successful in predicting platinum sensitivity at primary treatment than at relapse.49 Other potentially important mutations include CDK12, loss of which may induce an HRD phenotype,50 although this needs further validation, as not all alterations will have the same effect on HR repair and sensitivity to platinum. Whole-genome studies in HGSC reveal that gene breakage commonly inactivates the tumour suppressors RB1, NF1, RAD51B and PTEN and contributes to acquired chemotherapy resistance. CCNE1 amplification is common in primary resistant and refractory disease, demonstrating the role of non-HRD molecular mechanisms in resistance development.51 52 An association between excision repair cross-complementation group 1 (ERCC1) polymorphism and platinum sensitivity has been reported in a few studies but with conflicting results; hence, this is not suitable for assessing platinum response.53–55
Finally, in patients with relapsed disease, the current classification strictly defines platinum resistance as those relapsing within 6 months of previous platinum chemotherapy. However, because time since last platinum chemotherapy represents a continuum of probability of response to further chemotherapy, a fixed 6-month cut-off decision on platinum sensitivity is neither sensible nor biologically relevant. In addition, the effect of maintenance therapies on the probability of response to further platinum is unknown. The time since last platinum chemotherapy correlates with response to other agents including PARP inhibitors, although this is not absolute.56 Large-scale trials collecting serial biological samples throughout treatment are required in order to improve the understanding of acquired resistance. In addition, investigation and validation of markers should be carried out using samples taken immediately before and during the therapy of interest rather than using archival samples.
Recommendation 3.1
There are no validated predictive markers of primary platinum refractory or resistant disease.
Level of evidence: IV
Strength of recommendation: A
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
Recommendation 3.2
Defects in HR repair are associated with improved outcome/PFS following platinum-based chemotherapy.
Level of evidence: IV
Strength of recommendation: A
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
Recommendation 3.3
The time elapsed since last platinum chemotherapy represents a continuum of probability of response to further chemotherapy.
Level of evidence: IV
Strength of recommendation: A
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
4. Can we develop accurate and sensitive circulating and tissue biomarkers both of response and relapse?
The Gynecologic Cancer InterGroup (GCIG) has published a consensus document regarding the criteria that should be used in clinical trial protocols to define PFS after first-line therapy, as well as the criteria to define response to treatment in recurrent disease using the serum marker CA125, and has specified the situations where these criteria should be used.57 This WG agrees to the utility of these criteria in routine practice but emphasises the importance of correlation with radiological and clinical assessment.
CA125 levels have been most widely studied in HGSC. The prognostic value of CA125 in other morphological types of EOC, such as low-grade serous, clear cell, endometrioid and mucinous, is less clear due to the relative rarity of these neoplasms in the advanced disease setting and the limited number of patients studied in trials. As a result, CA125 is not a reliable marker in non-HGSC EOC,58 59 in particular in mucinous carcinoma, where it is rarely secreted. Caution is also recommended when using CA125 as a response marker for molecularly targeted agents until prospective studies validate CA125 changes with objective imaging response results.60 61 Specifically, there is a lack of reliability of CA125 response criteria with anti-VEGF molecular therapies, where CA125 change may not correspond to imaging response criteria for EOC patients receiving bevacizumab.
Human epididymis protein 4 (HE4) has been proposed as the most promising biomarker that may complement CA125 and has been approved by the US Food and Drug Administration (FDA) in monitoring the follow-up and relapse of EOC patients. However, studies are contradictory62; as a result, HE4 testing currently cannot be recommended in routine practice.
Circulating tumour cells (CTCs) and circulating cell-free DNA (cfDNA) have been used as diagnostic and prognostic markers in many types of cancer, including ovarian cancer. These techniques do have specific challenges, including pre-analytical issues regarding sample volume, the proper tubes for sample collection, sample storage and the time of the analysis, quality control, and analytical validation of the assays. There are currently no standard methods for the isolation and detection of either CTCs or cfDNA in the bloodstream, with few studies recruiting large cohorts of EOC patients. Further studies regarding the validation, standardisation and quality control of the assays are needed before implementing this approach in the clinical routine.63
Another approach to address this question is the chemotherapy response score (CRS), which was developed to enable reproducible and prognostically relevant reporting of the histopathological changes in interval debulking surgical specimens after neoadjuvant chemotherapy (NACT) in extrauterine HGSC.64 65 Since its description, the CRS has been independently validated in several studies,66–69 including an individual patient data meta-analysis incorporating results from over 800 patients from different centres worldwide.70 This system has been recommended for use in the ICCR guidelines for tubal and ovarian carcinomas,19 since a numerical score allows objective reporting and comparison of results and is thus superior to descriptive reporting (see Table 3). The score identifies the roughly one-third of all patients (CRS3; total or near-total response) who show significantly improved PFS and OS, and has potential for incorporation into routine practice and clinical trial design as an early endpoint.
Chemotherapy response score: summary of criteria
Recommendation 4.1
The CA125 criteria for response and progression as agreed by GCIG have utility in routine practice but should be used in combination with radiological and clinical assessment.
Level of evidence: III
Strength of recommendation: A
Consensus: 97.5% (39) yes, 0% (0) no, 2.5% (1) abstain (40 voters)
Recommendation 4.2
The role of CA125 as a marker of response and progression in non-HGSC is less clear.
Level of evidence: V
Strength of recommendation: A
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
Recommendation 4.3
The use of CA125 in assessing response and progression to targeted therapies is not yet proven; thus, radiological and clinical assessment should be used.
Level of evidence: V
Strength of recommendation: A
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
Recommendation 4.4
HE4 should not be used routinely to assess response and progression due to conflicting results.
Level of evidence: IV
Strength of recommendation: A
Consensus: 97.5% (39) yes, 0% (0) no, 2.5% (1) abstain (40 voters)
Recommendation 4.5
Quantification of circulating cfDNA has not been established as a tool to assess response and relapse.
Level of evidence: IV
Strength of recommendation: A
Consensus: 97.5% (39) yes, 0% (0) no, 2.5% (1) abstain (40 voters)
Recommendation 4.6
Pathological CRS after NACT may provide an objective and reproducible prognostic measure of outcome in HGSC.
Level of evidence: IV
Strength of recommendation: A
Consensus: 82.5% (33) yes, 12.5% (5) no, 5% (2) abstain (40 voters)
5. What are the morphological criteria useful in separating borderline from invasive ovarian neoplasia?
Previously, it was a widely held view that the distinction between a borderline ovarian tumour (BOT) and a carcinoma was based on the presence of destructive stromal invasion in the latter. However, ovarian carcinomas, particularly of mucinous and endometrioid type, can exhibit expansile (non-destructive) or infiltrative (destructive) stromal invasion. Mucinous carcinomas exhibiting expansile invasion have been reported to have a lower risk of metastasis than those exhibiting infiltrative invasion.71–76 Expansile invasion is morphologically characterised by complex glandular, papillary and/or cribriform architecture with a labyrinthine or anastomosing pattern and little or no intervening stroma.73–75 77
Extraovarian disease in association with a serous BOT (sBOT) was previously divided into non-invasive and invasive implants, and the former were further divided into ‘epithelial’ and ‘desmoplastic’ implants.78 In the 2014 WHO classification,7 it is stated that the term extraovarian ‘LGSC’ should be used for invasive implants in association with an sBOT. The WG regards such terminology as potentially confusing and wishes to separate bona fide metastases from an ovarian LGSC from invasive implants in the omentum or peritoneum associated with an sBOT.
The micropapillary variant of sBOT is characterised by the presence of slender papillae with a length-to-width ratio of at least 5:1, growing in a non-hierarchical pattern; a cribriform growth pattern is less frequent but may co-exist with the micropapillary pattern. The micropapillary or cribriform component must be confluent over an area of at least 5 mm in maximum extent for the tumour to be designated as a micropapillary variant of sBOT.78 79 The micropapillary variant of sBOT is more likely to be associated with extraovarian invasive implants than the typical sBOT, and some advocate using the term ‘non-invasive LGSC’ for the former. This has resulted in this term being used interchangeably with the micropapillary variant of sBOT in the 2014 WHO classification.7 A recent population-based study of a Danish cohort with long-term follow-up reported that patients with the micropapillary variant of sBOT are more likely to present at advanced stage and more frequently have bilateral disease, gross residual disease after surgery, areas of microinvasion, and invasive implants at presentation compared with patients with usual-type sBOT.80 The WG does not favour the use of the term ‘non-invasive LGSC’, since such tumours which are confined to the ovary at presentation have a comparable outcome to the usual-type sBOT and the term may be misleading for clinical management.
There have been various definitions of microinvasion in BOTs and the 2014 WHO classification7 uses a cut-off of 5 mm. Microinvasion can be seen in all morphological subtypes of BOT but is most common in serous and mucinous neoplasms. Two types of microinvasion have been described, namely ‘microinvasion’ and ‘microinvasive carcinoma’, although the distinction between these is not always straightforward.81 Although the presence of microinvasion has been associated with a higher risk of tumour recurrence in some series,82 the majority of studies have not identified such an association.83 84 The WG recommends that BOTs with microinvasion should be classified and managed as borderline tumours.
The term implant should be restricted to extraovarian disease in association with an sBOT and not be used in the context of a mucinous BOT (mBOT). Extraovarian disease in a patient with a presumed mBOT either represents metastasis from an undiagnosed or undetected focus of carcinoma within the ovary, or the ovarian and extraovarian disease represents metastasis from a mucinous carcinoma elsewhere.
Borderline endometrioid tumours are rare.81 The criteria used to distinguish a borderline endometrioid tumour from endometrioid adenocarcinoma are broadly similar to the criteria used to distinguish atypical hyperplasia from grade I endometrioid adenocarcinoma in the uterine corpus, and are largely architectural. Adenocarcinomas are characterised by complex growth with gland fusion and stromal exclusion; cribriform and microglandular patterns may also be seen.85
Recommendation 5.1
Destructive stromal invasion is no longer necessary for carcinoma diagnosis (carcinomas may exhibit expansile invasion).
Level of evidence: V
Strength of recommendation: A
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
Recommendation 5.2
According to the 2014 WHO classification, extraovarian invasive implants in association with an sBOT are synonymous with extraovarian LGSC. The WG does not support this terminology because it may be misleading for clinical management.
Level of evidence: V
Strength of recommendation: A
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
Recommendation 5.3
In the 2014 WHO classification, the micropapillary variant of sBOT is also termed non-invasive LGSC but the WG does not support this terminology because it may be misleading for clinical management.
Level of evidence: V
Strength of recommendation: A
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
Recommendation 5.4
Microinvasion (<5 mm) can be seen in borderline tumours but these cases should still be regarded as borderline for classification and management purposes.
Level of evidence: V
Strength of recommendation: A
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
Recommendation 5.5
The term implant should not be used in the context of mBOTs; extraovarian disease in association with an mBOT should be considered as metastasis (from ovary or another organ).
Level of evidence: V
Strength of recommendation: A
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
Recommendation 5.6
Borderline endometrioid tumours can be differentiated from grade I endometrioid carcinoma using similar criteria as used to differentiate atypical hyperplasia from grade I endometrioid carcinoma in the uterine corpus.
Level of evidence: V
Strength of recommendation: A
Consensus: 97.5% (39) yes, 0% (0) no, 2.5% (1) abstain (40 voters)
Early-Stage and Borderline Tumours
6. Are there exceptions to the standard surgical management for early-stage ovarian carcinoma?
The standard surgical approach in early-stage ovarian cancer is based on removal of both ovaries with a staging procedure. A complete exploration of the abdomino-pelvic peritoneal cavity via a thorough visual examination is required to detect potentially suspicious implants. Peritoneal staging surgery is based on peritoneal washing, peritoneal biopsies (pelvic peritoneum, paracolic gutters, diaphragm) (4–6) and omentectomy (at least infracolic). The standard approach is by open surgery. The rationale for this choice is based on the accuracy of the macroscopic exploration and the reduction of the risk of a rupture of the primary tumour during its dissection/removal. This risk is potentially increased using a minimally invasive surgical approach.86 Regardless of the approach used, rupture of an intact tumour could alter the FIGO staging and affect prognosis, and must be avoided.87 Nevertheless, the minimally invasive approach can be considered for restaging surgery in cases where the initial ovarian tumour has been removed and there is no risk of ‘rupture’ of the ovarian lesion. This surgery should then be carried out by trained surgeons in expert centres to assure optimal assessment vision of all abdominal quadrants and to lower the risk of peri- and postoperative complications. Nodal staging surgery is part of the ‘conventionally’ required procedure in early-stage ovarian carcinoma. This nodal staging surgery of apparent stage I ovarian carcinoma includes a bilateral pelvic and para-aortic lymphadenectomy up to the left renal vein (regardless of the surgical approach used).88 89 Ten to 15% of cases have nodal involvement.88 However, due to a low prevalence of nodal metastases in some histological subtypes (eg, mucinous carcinoma of expansile subtype or LGSC), the indication for staging surgery in these cases90–92 may be questioned.
The issue of restaging surgery must be addressed separately. Contrary to the indication of staging surgery discussed above, where the decision is based on macroscopic evaluation of the abdominal cavity and the result of a frozen section analysis (FSA), some patients may have initially undergone surgery without proper staging. In this context, the restaging procedure is indicated if it may bring new elements that have a direct impact on the definitive treatment planning. If the primary tumour exhibits high-risk features (eg, high-grade, capsule rupture, tubal or peritoneal extension) that justify adjuvant chemotherapy, indication of nodal restaging surgery with the aim of obtaining additional prognostic variables must be balanced with the potential surgical morbidity of the procedure.
FSA should be available during a surgical procedure carried out for a suspicious ovarian mass and should be supported by the diagnosis of an experienced gynaecological pathologist. Nevertheless, it must only be done when the surgical strategy would be altered by the outcome (eg, choice of a nodal or radical surgery). FSA is less accurate in cases of pathological diagnosis of borderline tumours, mucinous tumours, tumour sampling done by an inexperienced oncologist, or large ovarian lesions (>8–10 cm).93 94
Recommendation 6.1
Laparotomy is the standard surgical approach to treat and stage patients with apparent early-stage ovarian carcinoma.
Level of evidence: V
Strength of recommendation: A
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
Recommendation 6.2
Minimally invasive surgery can be carried out for restaging.
Level of evidence: IV
Strength of recommendation: B
Consensus: 75% (30) yes, 12.5% (5) no, 12.5% (5) abstain (40 voters)
Recommendation 6.3
Whatever the approach used, rupture of an intact tumour with spillage of cancer cells at the time of surgery must be avoided.
Level of evidence: IV
Strength of recommendation: A
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
Recommendation 6.4
Peritoneal restaging surgery is mandatory even if it does not alter the indication for adjuvant chemotherapy.
Level of evidence: V
Strength of recommendation: B
Consensus: 92.5% (37) yes, 2.5% (1) no, 5% (2) abstain (40 voters)
Recommendation 6.5
Peritoneal restaging should be considered in cases of incidentally detected, apparently isolated STIC lesions.
Level of evidence: IV
Strength of recommendation: B
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
Recommendation 6.6
The standard surgical staging of apparent early EOC includes systematic lymph node (LN) dissection of the pelvic and the para aortic regions up to the left renal vessel origin.
Level of evidence: IV
Strength of recommendation: A
Consensus: 77.5% (31) yes, 22.5% (9) no, 0% (0) abstain (40 voters)
Recommendation 6.7
LN dissection for restaging purposes may be avoided if the nodal status does not alter the patient management.
Level of evidence: V
Strength of recommendation: B
Consensus: 95% (38) yes, 0% (0) no, 5% (2) abstain (40 voters)
7. What are the limits of fertility-sparing surgery (cancer and borderline ovarian tumour)?
Fertility-sparing surgery (FSS) is based on unilateral salpingo-oophorectomy and complete surgical staging. This management seems to be safe in patients with conventional low-grade stage IA (serous, endometrioid or mucinous expansile subtype).95–97 The use of FSS in patients with stage IC disease should be defined using the current 2014 FIGO staging system.98 FSS is acceptable for stage IC1 tumours, with half of these recurrences being isolated on the remaining ovary and therefore able to be rescued by subsequent surgery. However, the recurrence rates are higher in stage IC2, IC3 and grade 3 disease, although mainly in extraovarian sites and are, therefore, not clearly correlated with the fertility-sparing approach. Adequate counseling is, therefore, needed in this situation.98
In cases of stage II or III disease, the use of FSS is unconventional, with high risk of recurrences reported.95 FSS remains contraindicated in these patients, although it is unclear whether such recurrences are related to the natural history of the disease rather than the type of surgery in these ‘high-risk’ patients.
Recommendation 7.1
FSS can be safely offered to all stage IA and IC1 low-grade ovarian carcinomas.
Level of evidence: IV
Strength of recommendation: B
Consensus: 94.7% (36) yes, 2.6% (1) no, 2.6% (1) abstain (38 voters)
Recommendation 7.2
There is no place for ovarian preservation for invasive EOC greater than fully staged FIGO stage I.
Level of evidence: V
Strength of recommendation: A
Consensus: 94.9% (37) yes, 0% (0) no, 5.1% (2) abstain (39 voters)
8. Should all stage I carcinomas receive adjuvant chemotherapy and, if not, which ones?
A Cochrane systematic review99 clearly demonstrated that the addition of adjuvant platinum-based chemotherapy to surgery is effective in significantly prolonging long-term OS and PFS in women with early-stage EOC. Considering the risk of recurrence, the ICON1 trial100–103 determined that women with a high-risk of recurrence (stage IA grade 3, IB or IC grade 2 or 3, any clear cell tumours) may benefit the most from adjuvant chemotherapy. Retrospective studies104–107 suggested that adjuvant chemotherapy may not be necessary for some histological subgroups, due to the absence of recurrences observed in patients who did not receive adjuvant chemotherapy. It should be noted that the ICON1 trial100–103 could neither confirm nor exclude survival benefits in low/intermediate risk disease (stage IA grade 1 or 2, IB or IC grade 1) in a subgroup analysis. Recently, the retrospective SEER database also reported no benefit for adjuvant chemotherapy in the low and intermediate endometrioid groups.108 On the contrary, in a large cohort study,109 chemotherapy was associated with reduced mortality not only for high-risk patients but also for patients with stage IA/IB, grade 2 ovarian cancer. This study was in line with prior study results demonstrating no benefit for chemotherapy in women with stage IA and IB, grade 1 neoplasms. Finally, the available data could neither confirm nor exclude survival benefits for the addition of adjuvant chemotherapy in optimally staged patients (all risk groups considered). More specifically, for histological subgroups such as clear cell carcinoma, the targeted retrospective studies reported in the literature primarily from Asian populations105 107 108 110 did not identify any benefit compared with observation for early-stage disease (stage IA to IC1). For the mucinous subgroup, the expansile or grade I type is associated with better prognosis and should not receive adjuvant chemotherapy, while the infiltrative form is associated with a high risk of relapse.72 90 91 111
The chemotherapy administered in the ICON1100–103 and ACTION112–116 trials consisted of a variety of platinum-based regimens, given ideally for 6 cycles. However, only 4 cycles were required for the ACTION trial and only half of the patients in the ICON1 trial received all 6 cycles without dose modification, due to toxicity. Bell et al117 reported an RCT of 3 versus 6 cycles of adjuvant carboplatin and paclitaxel administered every 3 weeks in women with high-risk, early-stage ovarian cancer. This GOG trial found that longer treatment was not associated with a significant reduction in recurrence risk and resulted in additional toxicity. A subsequent exploratory analysis118 of this GOG study revealed that longer adjuvant therapy was associated with a significant reduction in recurrence risk for serous tumours but not for non-serous tumours. There was no benefit for longer adjuvant therapy in any other subgroup of interest, including age, performance status (PS), stage, grade and presence of ascites, tumour rupture and positive cytology. Bakkum-Gamez et al119 evaluated a cohort of surgically staged, stage I ovarian cancer patients who completed either 3 or 6 cycles of carboplatin and paclitaxel. Patients with stage IC cancer and with fixed tumours (described adhesions or fixation to other pelvic structures) and positive cytology and/or tumour surface involvement appeared to have a lower risk of recurrence after 6 cycles of carboplatin/paclitaxel compared with 3 cycles, although the cohort is recognisably small.
Four trials100–103 112–116 120–122 included in the Cochrane systematic review99 mentioned above used cisplatin-based chemotherapy, while one123 used melphalan. Six percent of women in the combined ACTION/ICON1 trials100–103 112–116 and none of the women in the other trials making up this meta-analysis received taxanes. The majority of women received carboplatin monotherapy (about 6 out of 10 patients in ACTION/ICON1 trials100–103 112–116 and all of the women included in the trial published by Tropé et al.121 122). The others received either cisplatin or cisplatin combinations. As part of the ICON3 trial124 comparing carboplatin with carboplatin plus paclitaxel, 20% of the population actually had stage I or II disease. There was no benefit in survival for the use of carboplatin plus paclitaxel either in the trial as a whole or in the women with early-stage disease, with >80% of patients receiving 6 cycles of chemotherapy. The GOG 175 trial125 demonstrated that adding 24 weeks of weekly maintenance low-dose paclitaxel to the standard 3 cycles of carboplatin plus paclitaxel did not significantly impact the recurrence-free interval in patients with completely resected, high-risk, early-stage ovarian cancer, and is associated with increased toxicity.
The potential importance of the timing of initiation of adjuvant therapy after surgery has been studied in patients with ovarian cancer.126–136 However, all of these published studies except one137 pertain to advanced disease or had a higher proportion of stage III–IV patients. Although this one report137 of early-stage ovarian cancer patients from two RCTs (GOG 95138 and GOG 157117) did not identify a benefit associated with earlier initiation of adjuvant therapy, it remains unclear if a significant delay in starting adjuvant therapy may worsen outcome. In conclusion, adjuvant chemotherapy should be based on decision-making treatment algorithms (see Figures 1–4). Platinum-based monotherapy or combination chemotherapy can be given. Optimal duration remains controversial; however, serous tumours should receive 6 cycles.

Adjuvant chemotherapy for patients with early-stage serous ovarian cancer (stage I–IIA).aConsidered no adjuvant chemotherapy only for patients with complete surgical staging.

Adjuvant chemotherapy for patients with early-stage mucinous ovarian cancer (stage I–IIA).aConsidered no adjuvant chemotherapy only for patients with complete surgical staging.

Adjuvant chemotherapy for patients with early-stage clear cell ovarian cancer (stage I–IIA).aConsidered no adjuvant chemotherapy only for patients with complete surgical staging.
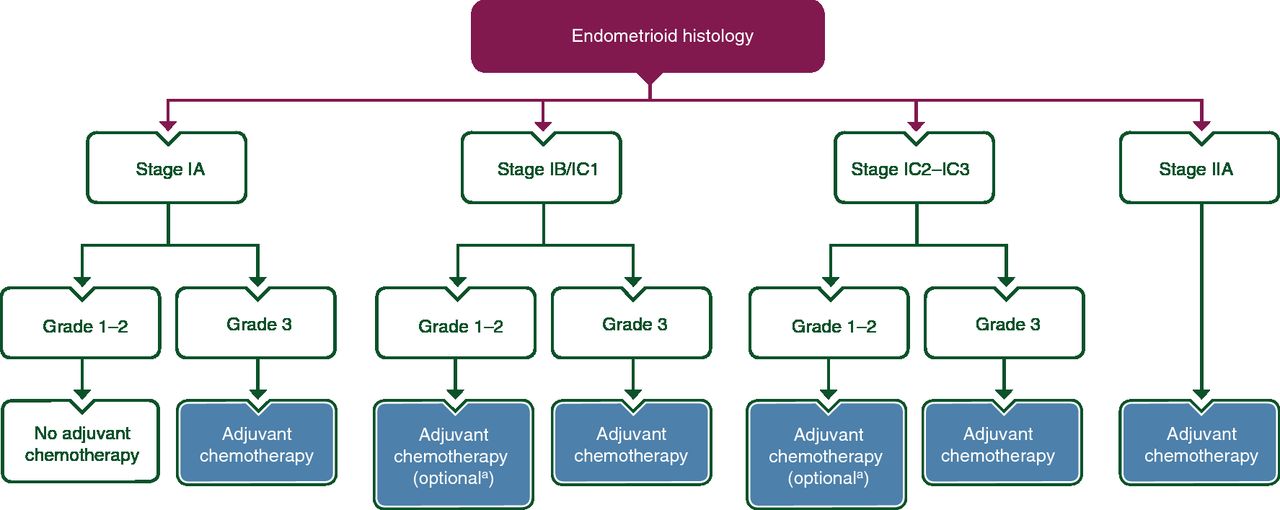
Adjuvant chemotherapy for patients with early-stage endometrioid ovarian cancer (stage I–IIA).aConsidered no adjuvant chemotherapy only for patients with complete surgical staging.
Recommendation 8.1
Adjuvant chemotherapy should be offered to patients with early-stage ovarian cancer (stage I–IIA) with the exception of fully staged patients with the following:
Low-grade serous IA
Grade 1 and 2 endometrioid IA
Grade 1 and 2 mucinous IA (expansile invasion)
Level of evidence: II
Strength of recommendation: A
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
Recommendation 8.2
Adjuvant chemotherapy is not recommended in the management of incidentally detected isolated STIC lesions.
Level of evidence: V
Strength of recommendation: A
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
Recommendation 8.3
The benefit of adjuvant chemotherapy is uncertain for patients with the following cancers and should be discussed on an individual patient basis:
Clear cell carcinoma stage IA and IB/IC1
Grade 1 and 2 endometrioid IB/IC
Low-grade serous IB/IC
Grade 1 and 2 mucinous IC (expansile invasion)
Mucinous IA (infiltrative invasion)
Level of evidence: III
Strength of recommendation: C
Consensus: 92.5% (37) yes, 7.5% (3) no, 0% (0) abstain (40 voters)
Recommendation 8.4
For patients with early-stage disease requiring adjuvant chemotherapy, acceptable treatment regimens are:
Carboplatin alone
Carboplatin/paclitaxel
Level of evidence: I (carboplatin alone), II (carboplatin/paclitaxel)
Strength of recommendation: A
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
Recommendation 8.5
For patients receiving single-agent adjuvant carboplatin, 6 cycles are recommended.
Level of evidence: I
Strength of recommendation: A
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
Recommendation 8.6
For patients receiving carboplatin and paclitaxel, a minimum of 3 cycles is recommended except for the high-grade serous subgroup or stage IC (any histological type), for whom 6 cycles are recommended.
Level of evidence: II
Strength of recommendation: B
Consensus: 77.5% (31) yes, 0% (0) no, 22.5% (9) abstain (40 voters)
9. Are non-serous borderline ovarian tumours managed according to the same standard as serous borderline ovarian tumours?
FSS (defined as the preservation of the uterus and at least a part of one ovary) is the standard management of young patients with BOTs,139 140 while bilateral salpingo-oophorectomy with or without hysterectomy is the standard management of BOTs in menopausal patients. Focussing on the risk factors for overall recurrences (borderline and invasive) for all patients, conservative treatment (and particularly cystectomy) and incompletely staged disease increased the rate of relapse.83 Nevertheless, those factors did not exert a statistical impact on the invasive recurrence rate because most of the recurrences were borderline tumours, which are unlikely to have a further impact on patient outcomes.140 141 The risk of an invasive recurrence is very low but exists, and is estimated at 0.5% after FSS.142 Even when preservation of healthy ovarian tissue is not technically ‘feasible’ (bulky bilateral involvement of ovaries), preservation of the uterus should be considered.
The impact of the histological subtype on surgical management (mBOT or sBOT) is still debated.83 142 143 Patients with mBOTs relapse less frequently than those with serous disease, but when a relapse occurs, the risk of an invasive recurrence seems to be higher for mBOTs.144 Nevertheless, clear evidence is lacking as to whether this is due to the particular natural history of this tumour, to a wider use of cystectomy or to the fact that, as mBOTs may be bulky, a small part of a ‘true’ invasive carcinoma may have been misdiagnosed after the initial sampling of a large tumour.144 Pragmatically, as most mBOTs are unilateral, unilateral salpingo-oophorectomy is recommended to decrease the potential risk of invasive recurrence.142 144
The case of serous disease is somewhat different because bilateral tumours are observed in 15–25% of cases and peritoneal spread in 15–40%.145 A meta-analysis and a large multicentre German series demonstrated that (ultraconservative) surgery (cystectomy) increases the risk of recurrence.139 141 Nonetheless, this does not imply that an adnexectomy should be preferred over a cystectomy because the use of this latter procedure also increases the subsequent fertility rate.146 A recent phase III trial (the only one concerning BOTs in the ‘modern era’) demonstrated that the use of bilateral cystectomies compared with a unilateral adnexectomy and a contralateral cystectomy (in patients with bilateral BOTs, mainly in serous subtype) increased the fertility rate without increasing the recurrence rate.146 Moreover, the risk of ovarian invasive recurrence is very low in stage I serous disease.144 Preservation of the maximum volume of the healthy ovary (and follicles) should, therefore, be proposed to improve fertility results. Cystectomy is an acceptable management in sBOTs to optimise fertility preservation.
Recommendation 9.1
Preservation of at least part of one ovary and the uterus is the standard approach in young patients with BOTs.
Level of evidence: III
Strength of recommendation: A
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
Recommendation 9.2
Unilateral salpingo-oophorectomy is recommended with mBOTs to decrease the risk of invasive recurrence after cystectomy.
Level of evidence: IV
Strength of recommendation: A
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
Recommendation 9.3
Cystectomy is an acceptable management in sBOTs to preserve fertility.
Level of evidence: III
Strength of recommendation: B
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
10. How should serous borderline ovarian tumours with extraovarian implant be managed?
Adequate staging in BOTs includes careful inspection of the peritoneum and peritoneal staging biopsies as previously described. Appendectomy as a staging procedure is not recommended even in the mucinous subtype.147 There is no evidence supporting LN dissection. Large studies have demonstrated that the omission of staging has an impact on recurrence rate.83 On the other hand, the benefit on OS of complete surgical staging in macroscopically stage I BOTs remains unproven.148 149 The benefit of restaging surgery is questionable if comprehensive staging has not been completed during the first surgery. Considering the potential morbidity associated with this procedure, surgical restaging should only be considered in the following situations: (1) patients with a higher risk of extraovarian microscopic implants (serous tumour with micropapillary patterns); or (2) patients with incomplete visual exploration of the abdomino-pelvic peritoneum during the first surgery.
In the case of sBOTs with peritoneal implants, residual disease has been reported to be a prognostic factor.142 150 151 Complete removal of peritoneal implants is necessary for both staging and therapeutic purposes. There is no proven benefit of lymphadenectomy in stage II/III sBOTs.142 Data in the literature concerning FSS in sBOTs with peritoneal implants are rare.140 145 Compared with stage I disease treated conservatively, the risk of recurrence is increased after conservative treatment of more advanced stages.145 These could be ovarian and/or peritoneal and so not related to the ovarian preservation itself but to the natural history of the initial peritoneal spread.145 Furthermore, the risk of lethal outcomes is rare in this context if a complete resection of implants is achieved.145 FSS could be then considered in selected stage II or III sBOTs. Some authors have suggested to extend this strategy even in the cases of invasive implants140; however, fewer than 15 cases have been reported.140 145
The role of adjuvant chemotherapy in advanced-stage sBOTs is highly debated.152 153 Recent retrospective data, collecting the largest number to date of patients with invasive implants treated with surgery and adjuvant chemotherapy, suggested a potential advantage in selected groups of patients.152 According to the available evidence, there is no benefit in adding adjuvant treatment to upfront surgery in patients with sBOTs with invasive implants.111 151–171 A meta-analysis on BOTs concluded that there is no evidence supporting the use of any specific type of adjuvant treatment.153 However, considering the low risk of invasive high-grade relapse, it is unlikely that it will be possible to demonstrate the efficacy of adjuvant treatment in these patients.
It is important to note that sBOTs with invasive implants would now be defined as ‘extraovarian LGSC’ according to the 2014 WHO classification.7 Since the management of young patients with sBOTs is clearly different than stage II/III LGSC (in terms of FSS in young patients, place of LN dissection or adjuvant treatment strategies), patients with sBOTs and invasive implants must be considered as a separate entity from advanced LGSC.
Recommendation 10.1
Peritoneal staging surgery is recommended for sBOTs.
Level of evidence: III
Strength of recommendation: B
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
Recommendation 10.2
The benefit of restaging is not clear but should be considered in patients with:
sBOTs with micropapillary pattern
sBOTs with incomplete visual exploration of the peritoneal cavity
Level of evidence: IV (sBOTs with micropapillary pattern), III (sBOTs with incomplete visual exploration of the peritoneal cavity)
Strength of recommendation: B
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
Recommendation 10.3
There is no role for appendectomy in BOTs.
Level of evidence: V
Strength of recommendation: A
Consensus: 85% (34) yes, 0% (0) no, 15% (6) abstain (40 voters)
Recommendation 10.4
All peritoneal implants must be removed.
Level of evidence: IV
Strength of recommendation: A
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
Recommendation 10.5
There is no proven benefit of systematic LN dissection in stage II/III sBOTs.
Level of evidence: IV
Strength of recommendation: B
Consensus: 97.5% (39) yes, 0% (0) no, 2.5% (1) abstain (40 voters)
Recommendation 10.6
FSS could be considered in selected patients with stage II or III sBOTs.
Level of evidence: V
Strength of recommendation: B
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
Recommendation 10.7
Adjuvant systemic treatment is not recommended for primary treatment of sBOTs with extraovarian invasive/non-invasive implants.
Level of evidence: III
Strength of recommendation: B
Consensus: 92.5% (37) yes, 0% (0) no, 7.5% (3) abstain (40 voters)
Advanced-stage Disease
11. How to select patients for primary debulking surgery or neoadjuvant chemotherapy?
Complete resection of all macroscopic disease has been shown to be the single most important independent prognostic factor in advanced EOC172 173 and careful evaluation of patients before surgery is essential for defining the management plan.174 If resection of all macroscopic disease can be obtained based on pre-operative staging with an acceptable operative morbidity, upfront debulking surgery (UDS) followed by carboplatin/paclitaxel is standard of care.175 176 The EORTC55971 trial177 and the CHORUS trial178 have showed a similar PFS and OS for patients with stage IIIC or IV disease receiving NACT and interval debulking surgery (IDS) compared with UDS. As both studies contained low percentages of patients with complete upfront debulking surgery (<20%), the Trial on Radical Upfront Surgical Therapy (TRUST), including a qualification process for participating centres, is currently ongoing.
Nevertheless, evidence-based standardisation of the assessment of disease extent and patient condition are essential to predict the possibility of residual macroscopic disease after upfront debulking surgery.179 Pre-operative diagnostic work-up with computed tomography (CT), positron emission tomography (PET)-CT, or diffusion-weighted whole-body magnetic resonance imaging (MRI), should be used to assess the extent of disease.180–183 Ultrasound imaging quality has improved in recent decades; if carried out by an experienced sonographer, ultrasound has an invaluable role in estimating the malignant potential and histopathological features of ovarian cysts but also in assessing tumour extent in the pelvis and abdominal cavity.184–186 Diagnostic laparoscopy can provide a definitive histopathological diagnosis and detailed information about the intra-abdominal disease burden (eg, Fagotti scoring system).187 188 After laparoscopy, a high rate of port-site metastases are observed, but do not worsen the prognosis.189
Based on previously described examinations, in 2017 ESGO formulated recommendations on contraindications to UDS related to tumour spread.190 Patient-specific factors (eg, co-existing illnesses, age, WHO PS) should also be considered in the pre-operative assessment of operability.174 179 To assure adequate management of patients with HGSC, diagnostic work-up as well as the treatment should be carried out in a multidisciplinary setting and in a specialist ovarian cancer centre, according to ESGO Quality recommendations 2016.191
Recommendation 11.1
The selection of patients for primary debulking surgery or neoadjuvant treatment must be carried out in a specialist ovarian cancer centre, according to the ESGO Quality recommendations 2016191 in a multidisciplinary setting.
Level of evidence: IV
Strength of recommendation: A
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
Recommendation 11.2
Complete tumour resection at upfront debulking is the most important prognostic factor for patients with advanced ovarian cancer and is the main goal of surgery.
Level of evidence: IV
Strength of recommendation: A
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
Recommendation 11.3
When complete surgery with no macroscopic visible disease appears feasible (both spread of disease and general condition of the patient), primary upfront debulking should be offered.
Level of evidence: IV
Strength of recommendation: B
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
Recommendation 11.4
Diagnostic work-up with CT, PET-CT or diffusion-weighted whole-body MRI and expert ultrasound or diagnostic laparoscopy should be used to assess the extent of disease.
Level of evidence: III
Strength of recommendation: C
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
Recommendation 11.5
Patients are not candidates for primary surgery (according to ESGO 2017 recommendations190) if the following spread of disease, among other factors, is present:
Diffuse deep infiltration of the root of small bowel mesentery
Diffuse carcinomatosis of the small bowel involving such large parts that resection would lead to a short bowel syndrome (remaining bowel <1.5 m)
Diffuse involvement/deep infiltration of:
stomach/duodenum
head or middle part of pancreas
Involvement of coeliac trunk, hepatic arteries, left gastric artery
Central or multisegmental parenchymal liver metastases
Multiple parenchymal lung metastases (preferably histologically proven)
Non-resectable LNs
Brain metastases
Level of evidence: III
Strength of recommendation: A
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
12. What is the current role of bevacizumab in first-line treatment?
Bevacizumab was the first targeted therapy to receive the approval of the European Medicines Agency (EMA) for the treatment of EOC in the first-line and relapsed settings. GOG 218,192 a placebo-controlled phase III trial, randomised patients with incompletely resected stage III or any stage IV newly diagnosed EOC to either carboplatin/paclitaxel with or without bevacizumab (15 mg/kg) followed by placebo or bevacizumab maintenance treatment up to 21 cycles; a significant increase in PFS was shown in patients receiving bevacizumab for 21 cycles. The ICON7 trial193 included patients with high-risk, early-stage disease (stage I or IIA and clear cell or grade 3 tumours) or advanced-stage IIB to IV tumours. Despite lower dosage and fewer cycles of bevacizumab (7.5 mg/kg for 18 cycles) used in the ICON7 trial, PFS results were similar.193 Neither the GOG 218 trial nor the ICON7 trial showed an OS benefit in the overall study populations,192 193 but post hoc subgroup analysis indicated statistically significant OS benefit in patients with stage IV disease in GOG 218194 and patients at high risk of progression (ie, FIGO stage III with >1 cm residual disease or stage IV) in the ICON7 trial.22
Bevacizumab-related toxicities are usually mild. The most common toxicities are ≥grade 2 hypertension and ≥grade 3 proteinuria. The incidence is positively correlated with higher dose and longer duration.192 193 Furthermore, the ICON7 and GOG 218 trials showed a trend towards more mucocutaneous bleeding, ≥grade 3 thromboembolic events, and gastrointestinal adverse events (AEs).192 193 195 Regarding gastrointestinal toxicity, the most common AE was perforation (1.1%), followed by hemorrhage (0.8%) and fistula formation (0.7%).22 195 Multivariable analysis estimated that previous treatment of inflammatory bowel disease and large bowel resections at UDS are significantly associated with increased odds of gastrointestinal AEs.195 Adequate patient selection is important to minimise the occurrence of these serious AEs.
Recently, the results of the SOLO1 trial were presented and showed the importance of the use of PARP inhibition after first-line chemotherapy in BRCA-mutated patients (without the use of bevacizumab).33 This phase III trial demonstrated a 70% risk reduction of disease progression or death with olaparib maintenance therapy after complete or partial response on first-line standard, platinum-based chemotherapy in patients with newly diagnosed, advanced BRCA-mutated ovarian cancer.
Regarding the administration of bevacizumab with NACT, two smaller RCTs, the ANTHALYA and GEICO 1205/NOVA open-label phase II trials,196 197 were carried out. Patients received 4 cycles of neoadjuvant carboplatin/paclitaxel with or without at least 3 cycles of bevacizumab (15 mg/kg) followed by IDS.196 197 Bevacizumab was stopped 4–5 weeks before surgery and restarted at least 7 weeks after IDS in the ANTHALYA trial,196 compared with 6 weeks before and 6 weeks after surgery in the GEICO 1205/NOVA trial.197 In the ANTHALYA trial,196 the complete resection rate was significantly higher with additional bevacizumab compared with the CRR previously reported in the EORTC study.177 In contrast, the GEICO 1205/NOVA trial197 showed no benefit in the complete macroscopic response rate (PCI=0) but found an enhanced rate of surgical operability. Both studies showed similar safety profiles, with no increase in toxicity (≥grade 3 hematological, gastrointestinal and vascular AEs) compared with carboplatin/paclitaxel therapy when adequate patient selection was carried out. Therefore, bevacizumab in the neoadjuvant setting is considered safe and may improve surgical outcome.
Recommendation 12.1
Bevacizumab (15 mg/kg or 7.5 mg/kg every 3 weeks for maximum of 15 months) improves PFS in patients with stage III–IV ovarian cancer and should be considered in addition to carboplatin and paclitaxel.
Level of evidence: I
Strength of recommendation: A
Consensus: 97.5% (39) yes, 0% (0) no, 2.5% (1) abstain (40 voters)
Recommendation 12.2
Bevacizumab in the neoadjuvant setting can be considered, although additional improvement in efficacy is not proven with level I evidence.
Level of evidence: II
Strength of recommendation: B
Consensus: 97.5% (39) yes, 2.5% (1) no, 0% (0) abstain (40 voters)
Recommendation 12.3
Bevacizumab can be safely administered in the neoadjuvant setting before and after IDS providing the interval between surgery and administration is at least 4–6 weeks.
Level of evidence: II
Strength of recommendation: B
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
13. Should weekly regimens be used in first line?
The JGOG 3016 trial,198 carried out in Japan, was the first multicentre RCT comparing first-line treatment with 3-weekly carboplatin (AUC6) and paclitaxel (180 mg/m2) with a dose-dense regimen of 3-weekly carboplatin and weekly paclitaxel (80 mg/m2). This showed improved PFS and OS rates but higher toxicity with the dose-dense regimen.198 In contrast, GOG 262199 (a multicentre phase III RCT) could not confirm this survival benefit despite using a similar study protocol. When patients did not receive bevacizumab, a subgroup analysis of the GOG 262 trial showed a significant increase in PFS in favour of weekly paclitaxel compared with 3-weekly. When receiving bevacizumab, no differences in PFS were shown.199 As this subgroup analysis was not pre-planned and only performed on 16% of the study population, weekly paclitaxel should not be regarded as a substitution for bevacizumab.
MITO-7, a multicentre open-label phase III RCT,200 was the first trial to compare 3-weekly carboplatin (AUC6) and paclitaxel (175 mg/m2) with weekly administration of carboplatin (AUC2) and paclitaxel (60 mg/m2). The weekly schedule showed similar survival rates but significantly better quality of life (QoL) (co-primary endpoint) with lower rates of ≥grade 3 neutropaenia, febrile neutropaenia, ≥grade 3 thrombocytopaenia, ≥grade 2 neuropathy, and alopecia. Van der Burg et al201 randomised patients to NACT with either weekly carboplatin (AUC4)/weekly cisplatin (70 mg/m2) and weekly paclitaxel (90 mg/m2) or 3-weekly carboplatin (AUC6)/cisplatin (75 mg/m2) and paclitaxel (175 mg/m2), and found similar response rates, PFS and OS between both groups.201 In contrast to the MITO-7 trial,200 (non)hematological toxicities were more frequent in the weekly schedule, probably caused by the higher dose intensity of platinum [cisplatin (40% of patients) or carboplatin] and higher doses of paclitaxel.
The first results of the ICON8 trial202 were presented at the ESMO 2017 Congress. As part of this trial, patients were randomised into three treatment arms: (1) 3-weekly carboplatin (AUC5/6) and weekly paclitaxel (80 mg/m2); (2) both weekly carboplatin (AUC2) and paclitaxel (80 mg/m2); and (3) standard 3-weekly carboplatin (AUC5/6) and paclitaxel (175 mg/m2). The use of weekly scheduling in the first-line treatment of EOC did not extend PFS, but, in contrast to the MITO-7 trial,200 no decrease in toxicity was seen (again, higher doses of paclitaxel were used).202 Therefore, weekly carboplatin/paclitaxel according to the MITO-7 schedule is an alternative to the 3-weekly schedule in Caucasian patients.
Recommendation 13.1
Incorporation of weekly chemotherapy into first-line treatment for women with EOC does not improve PFS or OS in the population of western countries.
Level of evidence: I
Strength of recommendation: A
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
Recommendation 13.2
The schedule of weekly chemotherapy with carboplatin (AUC2) and paclitaxel (60 mg/m2) shows better QoL and reduced toxicity (eg, alopecia, neuropathy) compared with the standard 3-weekly schedule and can be considered.
Level of evidence: I
Strength of recommendation: B
Consensus: 95% (38) yes, 0% (0) no, 5% (2) abstain (40 voters)
Recommendation 13.3
Weekly chemotherapy cannot be regarded as a substitute for bevacizumab.
Level of evidence: V
Strength of recommendation: B
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
Recommendation 13.4
3-weekly carboplatin/paclitaxel remains the standard-of-care chemotherapy of first-line ovarian cancer treatment.
Level of evidence: I
Strength of recommendation: A
Consensus: 100% (40) yes, 0% (0) no, 0% (0) abstain (40 voters)
14. Is there a place for intraperitoneal chemotherapy and hyperthermic intraperitoneal chemotherapy?
Several studies have been published, but due to their small sample size, incomparable treatment protocols and high levels of toxicity, intraperitoneal (i.p.) chemotherapy was not recommended for routine use.203–206 The GOG 172 trial randomised patients with stage III disease to either 3-weekly intravenous (i.v.) cisplatin/paclitaxel or i.v. paclitaxel followed by i.p. cisplatin/paclitaxel and showed a remarkable improvement in OS207 persisting even after 10 years.208 Despite these promising results, toxicity with i.p. (eg, grade 3–4 leukopaenia, gastrointestinal/renal AEs, infection and pain) was significantly higher with lower QoL and a lower completion rate207 for 6 i.p. cycles compared with previous reported studies.203 204 Moreover, the absence of an ITT analysis, the higher dosage of paclitaxel/cisplatin in the i.p. arm, the imbalance in PFS/OS benefit ratio and the low OS in the control group compared with published data209 210 further limit the clinical relevance and implementation of i.p. therapy in ovarian cancer.211 To address the pitfalls of the GOG 172 trial, a phase III RCT (GOG 252)212 was carried out on patients with stage II–IV EOC. As the first trial comparing i.p. and i.v. administration of similar doses of chemotherapy, the GOG 252 trial212 did not confirm PFS improvement with i.p. chemotherapy (presented at SGO 2016, still unpublished). Moreover, i.v. chemotherapy was better tolerated than i.p. chemotherapy.
The only RCT on the effect of hyperthermic intraperitoneal chemotherapy (HIPEC) in recurrent EOC has been widely criticised,212–215 and a meta-analysis216 of retrospective studies in advanced or recurrent EOC did not show any survival advantage but rather an increase in AEs (eg, anemia, acute kidney injury),217 218 precluding HIPEC from standard-of-care treatment. A recently published multicentre open-label phase III trial (OVHIPEC)219 randomised patients with stage III EOC with abdominal disease too extensive for UDS or after UDS with residual disease >1 cm, and after response to 3 cycles of NACT, to undergo IDS with or without HIPEC (cisplatin 100 mg/m2). The addition of HIPEC to IDS resulted in a significantly longer PFS and OS without increasing toxicity. However, as all stage IV patients were excluded and the majority of stage III patients could be primarily debulked to <1 cm,220–223 only a very small group of EOC patients with advanced disease fulfilled the criteria of inclusion, explaining the slow recruitment but also rendering extrapolation of these results to all patients with advanced disease impossible. Moreover, as OS was not a primary/co-primary endpoint, the small study size can induce significant bias, giving a possible explanation for the imbalance in PFS/OS improvement ratio.222 Furthermore, stratification was lacking for important prognostic factors like BRCA status, FIGO subclassification, response rates to NACT and histological type.222 223 Lastly, HIPEC toxicity appeared to be underreported as toxicity was reported equally in both study arms despite longer operation times, longer hospitalisation periods, more perioperative gastrostomies/stomas and vague reports on known AEs (eg, acute renal failure) when receiving HIPEC.222–225
At the ASCO 2017 Congress, Lim et al217 presented another trial including patients with stage III and IV ovarian cancer randomly allocated to the HIPEC arm (cisplatin 75 mg/m2, 90 min) or a control arm (no HIPEC) intraoperatively based on residual tumour (size <1 cm). The survival analysis did not show the statistical superiority of the HIPEC arm. Considering these concerns, HIPEC might provide additional survival benefit in EOC, but large prospective studies are required to further quantify the true efficacy of HIPEC and to compare its efficacy and compatibility with targeted therapy (eg, bevacizumab). In the meanwhile, HIPEC should not be considered as standard therapy and be limited to well-designed prospective RCTs.
Recommendation 14.1
i.p. chemotherapy is not a standard of care as first-line treatment.
Level of evidence: I
Strength of recommendation: A
Consensus: 95% (38) yes, 0% (0) no, 5% (2) abstain (40 voters)
Recommendation 14.2
HIPEC is not a standard of care as first-line treatment.
Level of evidence: II
Strength of recommendation: A
Consensus: 95% (38) yes, 0% (0) no, 5% (2) abstain (40 voters)
15. Is the standard of management of non-high-grade serous epithelial ovarian cancer different?
Similar to HGSC, optimal surgical treatment is the keystone of the treatment of advanced low-grade serous ovarian cancer.172 226 Regarding the less chemosensitive nature of low-grade serous ovarian cancer, even debulking with residual disease <1 cm may improve survival when complete cytoreduction is not feasible and can be an option. Also in the recurrent setting, a significantly increased PFS and OS was found after secondary cytoreductive surgery without residual disease.227 While carboplatin/paclitaxel is still the standard systemic therapy in low-grade serous ovarian cancer, multiple retrospective studies showed lower response rates and less survival benefit from chemotherapy compared with high-grade serous ovarian cancer, implicating a limited chemosensitivity.228–231 Similar findings were found in mucinous45 232 and clear cell EOCs.233 234 Being less chemosensitive, the role of surgery is enhanced and novel therapeutic strategies for systemic treatment of low-grade serous ovarian cancer are being investigated (eg, antihormonal and targeted therapies).
The majority of low-grade serous ovarian cancers have high ER and PR expression. Small retrospective studies suggest a possible therapeutic value of hormone therapy in first-line and recurrent settings.42 235 236 Despite promising results with selumetinib, an MEK1/2 inhibitor,237 no correlation was found between BRAF or KRAS mutation status and the therapeutic response in patients with recurrent low-grade serous ovarian cancer. Of note, a phase III RCT of an MEK inhibitor versus physician’s choice of chemotherapy in recurrent platinum-resistant low-grade serous ovarian cancer was prematurely closed for futility at the first interim analysis.
Regarding other targeted therapies, bevacizumab has shown activity in low-grade serous ovarian cancer in first-line and recurrent settings in three small retrospective cohorts.238–240 Hamanishi et al241 investigated the effect of nivolumab, an antibody that blocks programmed cell death protein 1 (PD-1) signaling, in patients with platinum-resistant ovarian cancer. One out of the two patients with clear cell histology included in this trial showed a complete remission with nivolumab. The high frequency of mismatch repair deficiency in clear cell carcinomas can provide an explanation for this behaviour towards PD-1 inhibitors. Pembrolizumab, another anti-PD-1 inhibitor, has been approved by the FDA in solid tumours with microsatellite/mismatch repair deficiency including ovarian cancer.242 Further investigation is currently ongoing.
Advanced (FIGO III and IV) non-high-grade serous ovarian cancer in first line
Recommendation 15.1
Primary debulking surgery with no macroscopic residual disease is of pivotal importance due to the low chemosensitivity in low-grade serous, mucinous and clear cell ovarian carcinoma.
Level of evidence: IV
Strength of recommendation: A
Consensus: 100% (38) yes, 0% (0) no, 0% (0) abstain (38 voters)
Recommendation 15.2
Even debulking with residual disease <1 cm in low-grade serous ovarian cancer may improve survival when complete cytoreduction is not feasible.
Level of evidence: IV
Strength of recommendation: C
Consensus: 100% (38) yes, 0% (0) no, 0% (0) abstain (38 voters)
Recommendation 15.3
Carboplatin in combination with paclitaxel is the standard chemotherapy. Addition of bevacizumab should be considered.
Level of evidence: I
Strength of recommendation: B
Consensus: 97.4% (37) yes, 0% (0) no, 2.6% (1) abstain (38 voters)
Recommendation 15.4
Maintenance antioestrogen therapy after chemotherapy can be considered in low-grade serous ovarian cancer.
Level of evidence: IV
Strength of recommendation: C
Consensus: 92.1% (35) yes, 0% (0) no, 7.9% (3) abstain (38 voters)
Recurrent non-high-grade serous ovarian cancer in first line
Recommendation 15.5
Secondary debulking surgery should be considered with the aim of no macroscopic residual disease.
Level of evidence: I
Strength of recommendation: B
Consensus: 100% (37) yes, 0% (0) no, 0% (0) abstain (37 voters)
Recommendation 15.6
In low-grade serous, low-grade endometrioid, mucinous and clear cell ovarian carcinoma, chemotherapy is an option but the magnitude of benefit is uncertain.
Level of evidence: IV
Strength of recommendation: B
Consensus: 100% (37) yes, 0% (0) no, 0% (0) abstain (37 voters)
Recommendation 15.7
Antioestrogen therapy can be considered in low-grade serous ovarian cancer and low-grade endometrioid ovarian carcinoma.
Level of evidence: IV
Strength of recommendation: B
Consensus: 97.3% (36) yes, 0% (0) no, 2.7% (1) abstain (37 voters)
Recurrent Disease
16. What is a reasonable monitoring and follow-up strategy following treatment of ovarian cancer?
Currently, evidence is lacking to demonstrate that routine follow-up of patients treated for ovarian cancer improves outcome.243–246 However, monitoring for recurrence might become more important if surgery for recurrent ovarian cancer is shown to improve survival.247 There is no evidence supporting a different follow-up regimen according to histotype, although it is recognised that not all tumours are associated with raised levels of CA125.248 At each visit, symptoms should be assessed and a physical examination should be carried out, although the latter has limited value in detecting relapse. Health-related QoL (HRQoL) measures, such as EORTC QLQ C30 and EORTC QLQ OV28, are potentially useful tools to assess symptoms,249 250 and could be adapted to be applied for routine use. Further to clinical examination and checking for symptoms, CA125 is the simplest tool to trigger imaging and is a better approach than regular routine imaging for diagnosis of recurrent ovarian cancer.244 251 Radiographic imaging, such as ultrasound, chest-abdomen-pelvis CT, whole-body MRI or PET-CT, should only be carried out if clinically indicated, based on symptoms, clinical examination or a rising CA125 level.252–255 Mucinous and clear cell ovarian cancers could represent a potential source of PET-negative findings.256 At present, CA125 remains the most important of the various biomarkers available for the detection of recurrent ovarian cancer257; however, an RCT258 did not show any survival advantage for initiating chemotherapy based on early detection of a higher CA125 concentration. It should be noted that this trial was not carried out in an era where surgery could be considered for selected cases, or where targeted therapies were used as a maintenance strategy for treatment of recurrent disease to lengthen disease control or survival.
A holistic approach, including patient education about signs and symptoms, monitoring and management of side effects, assessing the psychological and existential consequences of cancer is needed. Evaluation and support of family and social needs, counseling for genetic risk, guidance on fertility and contraception after ovarian cancer, management of menopausal symptoms and promotion of cardiovascular, bone, brain and sexual health should all be applied in the follow-up of ovarian cancer patients.259 Estrogen (+/- progestin) replacement is not contraindicated for severe menopausal symptoms, but the safety of hormonal replacement therapy in low-grade serous and low-grade endometrioid tumours is unclear.236 260
Follow-up is usually offered by gynaecological oncologists or dedicated medical oncologists. However, there is lack of evidence to show that it needs to be restricted to these groups, and specialised nurses or general practitioners could also be involved in the follow-up of ovarian cancer patients.261–263 Follow-up should be organised according to a locally agreed protocol. When follow-up is planned, a reasonable approach involves patient assessment every 3–4 months for the first 2 years, and every 6 months during years 3–5, but follow-up schemes may be individualised according to prognostic factors and treatment modalities. Further follow-up beyond 5 years should be individually discussed.248 264 Monitoring of maintenance therapy should be specialist-led and focus on the evaluation of toxicity and assessment of disease activity. Local protocols should be established specifically for the follow-up of patients on maintenance therapy. Imaging should be carried out according to symptoms and CA125 levels or periodically if the CA125 level was normal at the start of treatment. Follow-up after treatment of recurrent ovarian cancer should be specialist-led, as further recurrence is inevitable.
Recommendation 16.1
Follow-up should be offered, and the value should be discussed individually with patients, as there is uncertainty about the benefit of early diagnosis and treatment of recurrent disease.
Level of evidence: II
Strength of recommendation: C
Consensus: 100% (38) yes, 0% (0) no, 0% (0) abstain (38 voters)
17. What is the place of surgery for recurrent disease?
Cytoreductive surgery
Results of the Arbeitsgemeinschaft Gynäkologische Onkologie (AGO) DESKTOP III study265 demonstrated improved PFS and a longer time to first subsequent therapy (TFST) in patients with first recurrence randomised to secondary cytoreductive surgery. The PFS advantage of surgery was only seen following complete tumor resection and, therefore, complete resection should be regarded as a prerequisite for a potential OS benefit. OS in DESKTOP III is not yet mature and the results are expected in 2019. Recently shown data of an interim futility analysis of another trial (GOG 213)266 failed to demonstrate a PFS or OS advantage. It should be noted that patients in this trial were not systematically selected and the CRR was lower. Currently, the option of secondary cytoreductive surgery followed by platinum-based combination therapy should be discussed with all eligible patients.247 Patients should be selected if they have a high probability of having a complete resection and the following predictors for resection should be considered: platinum treatment-free interval (TFI) of >6 months, positive AGO score [good PS, complete resection at primary surgery and the absence of large volume (>500 mL) ascites], absence of probably irresectable lesions on imaging and absence of contraindications to surgery (eg, comorbidities, prior severe complications of surgery).267 It is important to note that platinum TFI and the AGO score have only been developed as positive predictors of complete resection and cannot be used to exclude patients from surgery. Additionally, centres offering secondary cytoreductive surgery should have the necessary resources and infrastructures, including an established multidisciplinary team coordinating the pre-, intra- and post-operative care needed to achieve complete resection in the majority of these procedures.191 In second or later recurrence there is limited evidence that highly selected patients (based on PS, tumour biology and localisation of metastasis) may benefit from complete cytoreductive surgery in specialised centres.268 269
Recommendation 17.1
Complete cytoreductive surgery followed by systemic treatment improves PFS and extends benefit to the next line of treatment in selected patients with first recurrence of ovarian cancer; OS data are not yet mature. Patients eligible for cytoreductive surgery should be informed about this option.
Level of evidence: I
Strength of recommendation: A
Consensus: 100% (38) yes, 0% (0) no, 0% (0) abstain (38 voters)
Recommendation 17.2
Complete cytoreductive surgery in second or later recurrence may provide benefit in selected patients and specialised centres.
Level of evidence: V
Strength of recommendation: A
Consensus: 100% (37) yes, 0% (0) no, 0% (0) abstain (37 voters)
HIPEC
Until now, there are no appropriately designed prospective studies on the effect of HIPEC added to secondary cytoreductive surgery in recurrent ovarian cancer. The results of multiple RCTs on HIPEC in recurrent ovarian cancer are awaited. Until these results are available, HIPEC remains an experimental therapy with potential harm and should only be offered in the context of well-designed, prospective RCTs. An objective benefit of HIPEC in relapsed ovarian cancer would need to take account of survival outcome and acceptability of the side effects.
Recommendation 17.3
In recurrent ovarian cancer, HIPEC added to cytoreductive surgery has not been proven to be beneficial in appropriately designed prospective studies.
Level of evidence: IV
Strength of recommendation: A
Consensus: 100% (38) yes, 0% (0) no, 0% (0) abstain (38 voters)
Palliative surgery
Malignant bowel obstruction (MBO) occurs frequently in patients with relapsed ovarian cancer. Although MBO is a frequent complication of ovarian cancer, the treatment given to patients is not based on high-level evidence. The available evidence on MBO has been summarised and integrated into a practical treatment algorithm (see Figure 5). In the medical management, corticosteroids (6–16 mg dexamethasone intravenously daily) may help to resolve MBO, with few side effects.270 Steroids should be tailed off after a few days if there is no benefit, and be appropriately reduced if there is a response to treatment. Octreotide can be added and is more effective than scopolamine butylbromide in controlling symptoms of MBO.271 Corticosteroids, octreotide and lanreotide have all been shown to provide some benefit in symptom control in recurrent ovarian cancer and MBO. The role of surgery for MBO remains unclear. One retrospective study showed a survival advantage following surgery for MBO compared with octreotide.272 In a Cochrane systematic review,273 the resolution of the symptoms of MBO following surgery varied from 26.7% to >68%, and successful oral feeding was established in 30–100% of patients. However, reporting on surgical management of MBO needs standardisation, as there are a wide variety of possible surgical techniques and indications.274 Perri et al275 suggested a scoring system to help select patients who were least likely to benefit from palliative surgery, based on age (>60 years), albumin (<25 g/L) and ascites (>2 L). In this study,275 patients who were eligible for bypass/resection and anastomotic procedures had a significantly better prognosis than those receiving a colostomy or ileostomy. Other surgical alternatives for MBO are percutaneous endoscopic gastrostomy tube and colorectal stent placement.276 277 Further data need to be collected prospectively on morbidity associated with both surgical and medical interventions for MBO. The role of surgery for MBO should be further clarified using objectified outcome measures, such as the ability to receive enteral feeding and QoL scores. Furthermore, data concerning re-obstruction rates, severe surgical complications, pain control, patient satisfaction and survival should also be collected in these studies.

Algorithm for the management of malignant bowel obstruction (MBO). PS, performance status.
Recommendation 17.4
MBO should be managed on an individual basis. There is a lack of evidence for optimal management and a need for clinical trials to evaluate medical, endoscopic and surgical approaches.
Level of evidence: V
Strength of recommendation: A
Consensus: 100% (37) yes, 0% (0) no, 0% (0) abstain (37 voters)
18. How should molecularly targeted therapy be integrated into the management of recurrent ovarian cancer?
Antiangiogenic therapy
Bevacizumab is approved in combination with platinum-based combination therapy and then as maintenance therapy in patients with a platinum-free interval (PFI) exceeding 6 months, and with non-platinum single-agent chemotherapy in patients with a shorter PFI. The OCEANS trial25 showed an improvement of PFS in patients treated with bevacizumab [15 mg/kg/every 3 weeks (q3w)] in combination with carboplatin/gemcitabine, who relapsed >6 months since last platinum and had no previous anti-VEGF treatment. OS was similar in both groups, which might partially be explained by the use of bevacizumab as a subsequent anticancer therapy in 43.9% of patients who were allocated to placebo in the study.278 The administration of bevacizumab in combination with paclitaxel/carboplatin in the GOG213 study279 showed a similar improvement in PFS. Also, the combination of bevacizumab with non-platinum single-agent chemotherapy [PEGylated liposomal doxorubicin (PLD), weekly paclitaxel or topotecan] improved PFS in patients who relapsed <6 months after a first or second line of platinum-based therapy.23 In the AURELIA trial,23 very strict inclusion criteria were used to limit the risk for gastrointestinal perforation. Patients were excluded if they had more than two prior lines of treatment, a history of bowel obstruction, platinum-refractory disease or significant serosal disease of the large bowel, especially if it involved the sigmoid colon. Overall, the addition of bevacizumab to chemotherapy with either weekly paclitaxel, PLD or topotecan significantly improved the median PFS. By using these criteria, only 2.2% of patients receiving bevacizumab developed a gastrointestinal perforation.23 The patient-reported outcomes (PROs) analysis of the study shows that chemotherapy combined with bevacizumab improved gastrointestinal symptoms more often compared with chemotherapy alone, especially in patients with ascites at the start of treatment.280 In both the AURELIA and GOG 2013 trials,29 214 only 10% of patients or less received prior bevacizumab treatment. Data presented at the ASCO 2018 Congress showed that, for patients previously treated with bevacizumab in first line and relapsing ≥6 months after last platinum treatment, re-challenge with bevacizumab in combination with platinum-based doublets was associated with a significantly prolonged PFS.281
Recommendation 18.1
Bevacizumab in combination with platinum-based second-line chemotherapy (gemcitabine or paclitaxel) followed by bevacizumab maintenance has proven benefit with respect to tumour response rate and PFS and could be recommended.
Level of evidence: I
Strength of recommendation: A
Consensus: 100% (38) yes, 0% (0) no, 0% (0) abstain (38 voters)
Recommendation 18.2
Bevacizumab in combination with second or third-line non-platinum chemotherapy (weekly paclitaxel, PLD, topotecan) has proven benefit with respect to tumour response rate and PFS, has been associated with improvement in QoL and could be recommended.
Level of evidence: I
Strength of recommendation: A
Consensus: 100% (38) yes, 0% (0) no, 0% (0) abstain (38 voters)
PARP inhibitors
Currently, there are three PARP inhibitors approved for the treatment of platinum-sensitive ovarian cancer. Olaparib maintenance treatment following platinum-based chemotherapy in patients with a BRCA mutation led to an improvement in PFS in study 1935 and in the SOLO2 trial.36 In study 19, patients without a BRCA mutation also derived a significant benefit in PFS. There was no significant OS benefit in study 19. In this study, 11% of patients remained on treatment for >6 years without evidence of progression. The OS data for SOLO2 are not yet mature.45 46 The NOVA trial38 with maintenance niraparib showed improved median PFS for both germline BRCA-mutated ovarian cancer and non-germline-mutated BRCA. The latter group included patients with a somatic BRCA mutation or BRCA WT.38 In ARIEL3,37 rucaparib given after a response to platinum-based therapy showed similar results in patients with BRCA mutations (germline or somatic mutations) as well as in the whole ITT group with high-grade cancer. Both NOVA and ARIEL3 trials included tumour testing for HRD, but neither was able to exclude a benefit from PARP inhibitors in HRD-negative patients. However, the magnitude of benefit of each of these PARP inhibitors was greatest in patients with a BRCA mutation, and least in those who were HRD-negative. Testing for a BRCA mutation is predictive for a response and provides an opportunity to identify mutations in unaffected family members who may benefit from cancer prevention strategies. Testing is recommended for all patients with non-mucinous ovarian cancers. Olaparib maintenance was permitted beyond progression, and both olaparib and niraparib studies led to an increase in the time to the next line of treatment, a clinically meaningful endpoint.35 36 38
Toxicity of PARP inhibitors is generally manageable through dose reductions and interruptions of therapy.36–38 Two studies282 283 have clearly shown a benefit for monotherapy with a PARP inhibitor in BRCA-mutated, relapsed high-grade ovarian carcinoma. A combination of two studies with rucaparib, ARIEL2 and study 10, led to the EMA approval of rucaparib in Europe as a monotherapy for relapsed or progressive BRCA-mutated (germline and/or somatic) HGSC, previously treated with ≥2 lines of platinum-based chemotherapy and unsuitable for further treatment with platinum-based chemotherapy.283 In Europe, the license for monotherapy is restricted to rucaparib and is only indicated for in patients with ‘platinum-sensitive’ disease.284 More recently, the SOLO 3 study randomised 266 patients with high-grade serous or endometrioid g-BRCA recurrent platinum-sensitive ovarian cancer to receive olaparib or non-platinum chemotherapy. Although the data have not been presented as yet, a public announcement reported statistically significant results in terms of response rate and PFS in favour of the olaparib arm.
Recommendation 18.3
PARP inhibitors (olaparib, niraparib, and rucaparib) when given as maintenance therapy following a response to platinum-based second or higher line of treatment, have proven benefit with respect to PFS and could be recommended. The benefit is greatest in, but is not limited to, patients with a BRCA mutation.
Level of evidence: I
Strength of recommendation: A
Consensus: 100% (34) yes, 0% (0) no, 0% (0) abstain (34 voters)
Recommendation 18.4
PARP inhibitors (rucaparib*, olaparib) are active as monotherapy in patients with a BRCA mutation and could be considered
*In Europe, only rucaparib is licensed by the EMA as a monotherapy for patients with ‘platinum-sensitive’ disease
Level of evidence: III
Strength of recommendation: B
Consensus: 100% (38) yes, 0% (0) no, 0% (0) abstain (34 voters)
19. What defines platinum resistance and how does that influence subsequent treatment?
How should platinum resistance be defined (primary and secondary resistance)?
Primary platinum resistance is a condition that is intrinsic to the tumour or occurs during first-line therapy, and leads to progressive disease during or immediately after therapy. Secondary platinum resistance is an acquired condition appearing or emerging after response to platinum therapy. Use of the terms ‘platinum-sensitivity’ or ‘-resistance’ varies; most commonly, ‘platinum-resistance’ has been a probabilistic definition, based on a likely poor response to platinum therapy. Similarly, ‘platinum-sensitivity’ has been defined as a patient likely to respond to platinum therapy. The latter must be separated from true observed platinum sensitivity in patients who respond to a platinum re-challenge and may be candidates for further maintenance therapy.
However, it is now questionable whether the historical prospective assumption of platinum sensitivity (or resistance) used for planning therapy in recurrent disease is valid. The PFI has been the main indicator to classify tumours as ‘platinum-sensitive’ or ‘-resistant’ based on a 6-month cut-off from the last platinum-based therapy.285 This definition, which evolved at a time when there were few options for treating recurrent disease other than platinum re-challenge, has several shortcomings and was abandoned during the Fifth Ovarian Cancer Consensus Conference (OCCC) of the GCIG.285 For example, increasingly the majority of patients undergo a complete resection of their advanced ovarian cancer during primary surgery, making a response evaluation afterwards impossible. Growth rate and tumour kinetics may differ among different histological types, and a 6-month cut-off cannot reliably separate those who responded or did not respond in this subgroup. Furthermore, not all patients having experienced a TFI from platinum (TFIp) longer than 6 months later respond to platinum and objective response rates range from 47.2 to 66%.25 279 286 287 In addition, TFIp shorter than 6 months is not always predictive of absence of response to platinum-based therapy. The interval may also depend on the frequency of follow-up and the sensitivity of diagnostic tools applied in a particular patient. Both weekly paclitaxel/carboplatin and carboplatin/gemcitabine displayed clinical efficiency in ‘platinum-resistant’ disease, with an overall response rate of 29% with both regimens.288 289BRCA-mutated patients in particular, but also BRCA WT patients, may respond to re-challenge with platinum-based chemotherapy, even with a TFIp of <6 months.47 For both groups, the response rate to platinum-based chemotherapy on relapse within 6 months after first-line treatment was higher compared with non-platinum regimens.47 Furthermore, the benefit of new biological drugs may not necessarily follow this historical paradigm; for example, PARP inhibitors are active in both cohorts of patients.290
How can we predict platinum resistance?
Currently, there are no validated, molecular, predictive biomarkers for platinum resistance. Several genetic modifications are associated with acquired resistance to platinum-based chemotherapy, such as inactivation of the tumour suppressors RB1, NF1, RAD51B and PTEN, reversions of germline or somatic BRCA1 or BRCA2 mutations, overexpression of the drug efflux pump MDR1 and CCNE1 amplification.51 The probability of platinum response also depends on the histological subtype, and, in the case of low-grade serous, clear cell or mucinous ovarian carcinomas, the response to platinum-based therapy is known to be poor. Low baseline global health status, poor physical function and the presence of abdominal/gastrointestinal symptoms are predictors of early discontinuation (within the first 8 weeks of treatment) of chemotherapy among patients with early relapse or after three lines of chemotherapy.291 Patients with a poor PS should be informed about the low probability of response to further platinum or non-platinum chemotherapy. However, all patients with recurrent ovarian cancer should be offered early palliative care, even though there are currently no data showing benefit specifically for ovarian cancer. A meta-analysis292 of randomised studies in advanced cancers (that cannot be cured) indicates that early palliative care may significantly improve QoL, decrease the intensity of symptoms and possibly improve survival.
The definition of platinum resistance should be therapy-oriented
As the TFI decreases, prognosis following subsequent treatment worsens; when the interval is ˂6 months, the anticipated median OS is around 10–12 months. At this point, the objective of treatment should be to control symptoms with a minimum of side effects, thereby preserving QoL. Response rates to platinum or non-platinum monotherapy regimens are all relatively similar. For patients for whom platinum-based therapy is no longer an option, sequential non-platinum therapy regimens can be offered. This group should be defined as those patients who have progressed while receiving platinum-based chemotherapy or experienced a symptomatic relapse soon after the end of the last platinum-based chemotherapy, and those for whom there is a contraindication to use further platinum-based treatment, such as allergy.293 Non-platinum drugs should be selected based on the toxicity profile and patient preference. The addition of bevacizumab to non-platinum regimens such as PLD, weekly paclitaxel or topotecan improves PFS and has also shown a reduction in ascites and improvement in gastrointestinal symptoms.23 24 280
Patients should be considered for further platinum therapy when platinum is not contraindicated or they do not have definite resistance, as described above. Tumour response rates to platinum are at least as good as to non-platinum drugs in this setting. Following a response, patients should be considered for maintenance treatment with a PARP inhibitor (see Figure 6). Additionally, platinum re-challenge could be considered following treatment with a non-platinum regimen (monotherapy or combination) if the criteria in Figure 6 suggesting that platinum ‘might not be the best option’ do not apply.
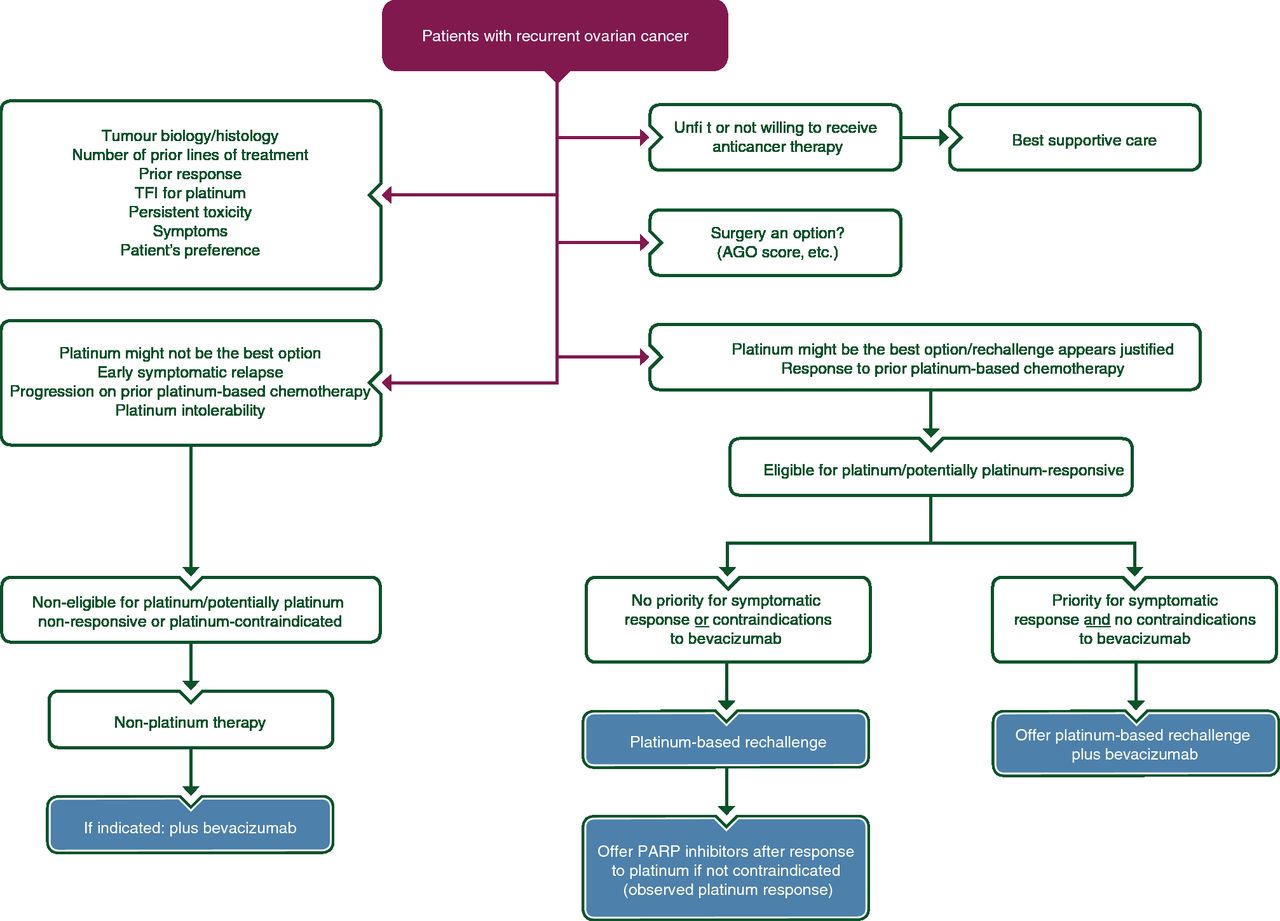
{kind=link}
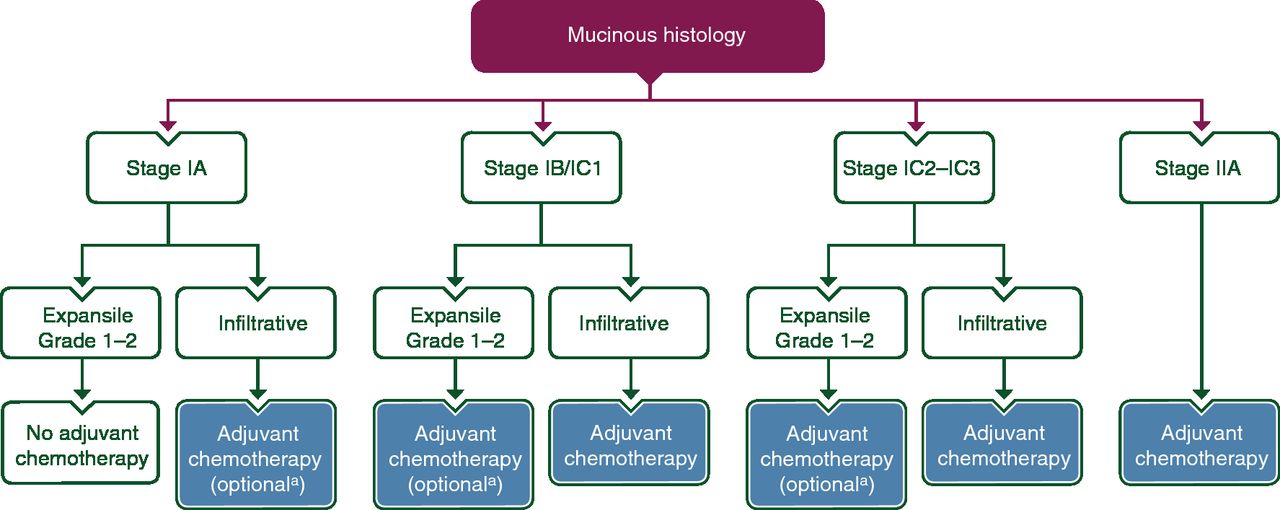{kind=link}
{kind=link}
{kind=link}
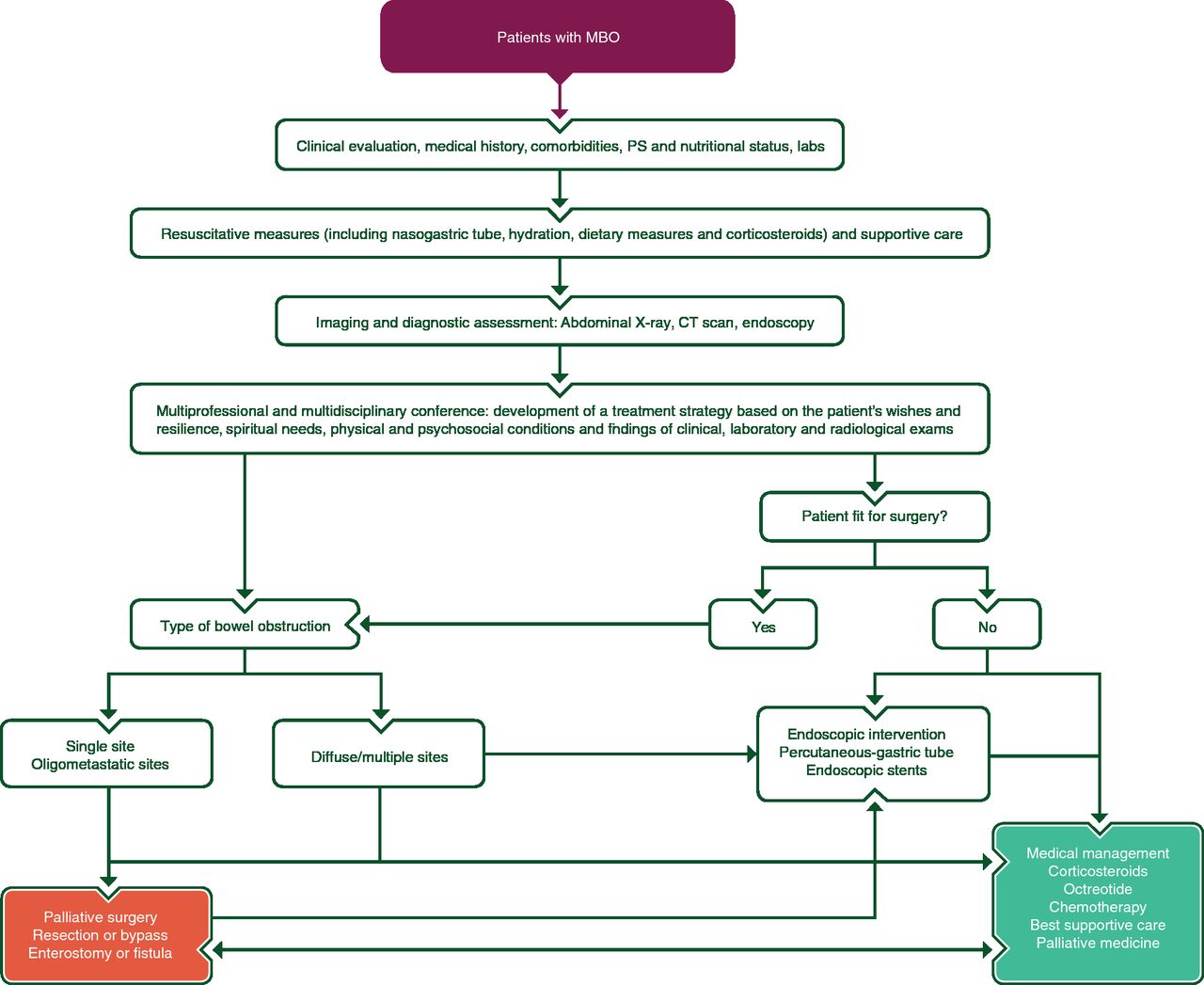{kind=link}
{kind=link}
Algorithm for the treatment of patients with recurrent ovarian cancer. AGO, Arbeitsgemeinschaft Gynäkologische Onkologie; PARP, poly(adenosine diphosphate-ribose) polymerase; TFI, treatment-free interval.
Treating patients with relapsed ovarian cancer
First, it should be determined if a patient is fit for anticancer therapy and willing to receive further treatment (see Figure 6). Next, the question of surgery should be considered (particularly for patients in first relapse) possibly by using the AGO scoring system. Tumour biology, histology, prior therapies, prior response to chemotherapy, TFIp (which continues to have prognostic value), persistent toxicity, patient preference and current symptoms all need to be taken into account when making a decision about whether or not to offer platinum-based therapy or non-platinum treatment. Patients for whom platinum-based chemotherapy might not be the best option are a heterogeneous group, containing both patients with early symptomatic relapse or progression during prior platinum-based chemotherapy and patients with platinum intolerability. These patients should be offered a non-platinum regimen, possibly in combination with bevacizumab. Patients who are potentially platinum-responsive should receive platinum re-challenge. In highly symptomatic patients who have no contraindications for bevacizumab the combination of platinum-based therapy with bevacizumab could be considered. Bevacizumab with platinum combinations (either paclitaxel or gemcitabine followed by bevacizumab maintenance) has demonstrated a significant benefit in PFS.25 266 278 279 Recently, PLD in combination with platinum and bevacizumab has been compared with carboplatin/gemcitabine and bevacizumab (ENGOT-ov18/AGO-OVAR 2.21294) and showed a significant PFS advantage compared with carboplatin/gemcitabine combined with bevacizumab. In patients with a BRCA mutation in this setting, there are no data comparing monotherapy with rucaparib to chemotherapy with bevacizumab, but the higher response rate seen when adding bevacizumab to chemotherapy would favour this combination. For asymptomatic patients with a BRCA mutation and PFI >6 months, either rucaparib monotherapy or platinum-based chemotherapy followed by a PARP inhibitor could be considered. Patients who have no priority for urgent symptomatic response, or in whom bevacizumab is contraindicated, such as thrombosis, fistula, etc, should be offered a PARP inhibitor if they respond to platinum re-challenge, irrespective of their BRCA mutation status. For relapsed ovarian cancer, licensed drugs in Europe include paclitaxel, PLD, topotecan, and the combination of trabectedin and PLD in patients with platinum-sensitive disease. This combination has shown superior efficacy compared with PLD monotherapy and can be considered in patients unable to tolerate further platinum, having relapsed >6 months after platinum.
Recommendation 19.1
There are currently no molecular biomarkers to predict platinum response.
Resistance to platinum in recurrent ovarian cancer is a therapy-oriented definition:
Proven platinum resistance: progression during platinum therapy
Assumed/expected platinum resistance: early symptomatic relapse with low probability of response to platinum; these patients should be treated with sequential non-platinum therapy adding bevacizumab if indicated.
Sensitivity to platinum in recurrent ovarian cancer is a therapy-oriented definition:
Proven platinum sensitivity: response to platinum; these patients can receive maintenance PARP inhibitors
Assumed/expected platinum sensitivity: previous response to platinum without early symptomatic relapse; these patients should be treated with platinum-based therapy adding bevacizumab or followed by maintenance PARP inhibitor therapy, if indicated. This group includes those who did not receive prior platinum or those who received adjuvant platinum post-surgery without any evaluable residual disease to assess chemotherapy response.
Level of evidence: I–IV
Strength of recommendation: A
Consensus: 85.7% (30) yes, 11.4% (4) no, 2.9% (1) abstain (35 voters)
Recommendation 19.2
Platinum re-challenge following treatment with a non-platinum regimen (monotherapy or combination) could be considered if a patient had not progressed during prior platinum therapy.
Level of evidence: IV
Strength of recommendation: A
Consensus: 100% (34) yes, 0% (0) no, 0% (0) abstain (34 voters)
Recommendation 19.3
Early palliative care should be integrated into the management of patients with recurrent ovarian cancer.
Level of evidence: V
Strength of recommendation: A
Consensus: 100% (34) yes, 0% (0) no, 0% (0) abstain (34 voters)
Recommendation 19.4
Incorporating HRQoL tools in the care of patients with a low probability of response to platinum may identify patients for whom subsequent therapy is futile, and this information should be discussed with the patient.
Level of evidence: III
Strength of recommendation: A
Consensus: 100% (34) yes, 0% (0) no, 0% (0) abstain (34 voters)
20. How long should therapy be continued in recurrent disease?
There are no RCTs studying the recommended length of treatment in recurrent ovarian cancer. In the CALYPSO trial295 and the AGO 2.5 study protocol,286 most patients received 6 cycles of carboplatin in combination with PLD/paclitaxel/gemcitabine. However, in CALYPSO,295 approximately 10% of patients received 9 cycles of chemotherapy instead of 6. Similarly, in the AGO-OVAR 2.5 study,286 in which administration of 9–10 cycles of carboplatin/gemcitabine was allowed at the physician’s discretion, a limited number of patients received >6 cycles. The ICON4 study protocol287 stated that at least 6 cycles of carboplatin/paclitaxel should be given, but the exact number of cycles was not published. In non-platinum-based studies protocols usually state that treatment can be given to progression (or toxicity). Frequently, the number of cycles is ˂6. For example, in a study296 comparing PLD and topotecan, platinum-resistant patients received on average 4.9 cycles of PLD and 5.7 cycles of topotecan. However, without evidence to the contrary, non-platinum treatment is often given until progression or toxicity occurs.
Stopping chemotherapy
Recommendation 20.1
For platinum-based chemotherapy, 6 cycles are recommended. More or fewer cycles have not been shown to be beneficial, and consideration should be given to the toxicity.
Level of evidence: V
Strength of recommendation: B
Consensus: 100% (34) yes, 0% (0) no, 0% (0) abstain (34 voters)
Recommendation 20.2
For non-platinum chemotherapies, treatment may be continued as long as there is clinical benefit and treatment is well-tolerated.
Level of evidence: V
Strength of recommendation: B
Consensus: 100% (34) yes, 0% (0) no, 0% (0) abstain (34 voters)
In the OCEANS and GOG 213 trials,278 279 maintenance therapy with bevacizumab treatment was stopped on disease progression. In the AURELIA trial,23 bevacizumab was not offered as a maintenance therapy; chemotherapy in combination with bevacizumab was continued to progression. Based on these results, it remains unclear when to stop bevacizumab treatment. Caution should be exercised in stopping treatment too early on the basis of a slow rise in CA125, either alone or with minor CT abnormalities. It is difficult to state that a patient at this point will no longer benefit from continuing bevacizumab. Consideration should be given to continuing bevacizumab until symptomatic progression or the next line of treatment is started.
Stopping bevacizumab
Recommendation 20.3
Recommended length of treatment remains unclear. Treatment is usually continued until disease progression. The continuation of bevacizumab beyond progression has not been evaluated in the recurrent setting.
Level of evidence: V
Strength of recommendation: B
Consensus: 97.1% (33) yes, 2.9% (1) no, 0% (0) abstain (34 voters)
Both in study 19 and SOLO2, progression was determined by Response Evaluation Criteria In Solid Tumours (RECIST) v1.1 criteria, but patients could continue olaparib beyond progression.34 36 For these patients the TFST could provide insight into the effect of treating beyond progression. For SOLO2,36 TFST analysis was preplanned and showed an additional advantage of 7.2 months, comparing the difference between the median TFST and PFS for patients who received olaparib compared with placebo. In the NOVA and ARIEL3 trials,43 44 PARP inhibitor treatment was discontinued on progression. Currently, the recommended length of PARP inhibitor treatment, based on these results, remains unclear. However, treatment beyond progression, until the next line of chemotherapy, should be considered and may have clinical value.
Stopping maintenance PARP inhibitors
Recommendation 20.4
Recommended length of treatment remains unclear. Despite an increase in TFST demonstrated for olaparib and niraparib, the benefit of continuing treatment beyond progression has not been demonstrated conclusively to date.
Level of evidence: III
Strength of recommendation: A
Consensus: 100% (34) yes, 0% (0) no, 0% (0) abstain (34 voters)
In gynaecological oncology practice, there is consensus on the importance of PROs (QoL and symptoms) and the incorporation of PRO endpoints in advanced or relapsed disease.250 297–300 The Standard Protocol Items: Recommendations for Interventional Trials patient-reported outcome (SPIRIT-PRO) guidelines could be used for preplanned PROs hypothesis.301 Currently, there are several QoL questionnaires available, such as the functional assessment of cancer therapy (FACT) Ovarian Symptom Index, the European Organisation for Research and Treatment of Cancer (EORTC) QLQ-OV28, and Measure of Ovarian Symptoms and Treatment (MOST); however, there is no gold standard available among the QoL questionnaires.302 Toxicity reported by the patients using the Patient-Reported Outcomes version of the Common Terminology Criteria for Adverse Events (PRO-CTCAETM) is a valuable measurement and could improve the reporting of side effects and toxicity in the future. However, reporting of toxicity by the physicians should also be adapted to evaluate the clinical relevance by including frequency, timing and duration, in addition to severity and incidence rates.303 304 Utility questionnaires such as EQ-5D and QTwist are developed to calculate QoL-adjusted PFS; they could add complementary information.
Velikova et al305 demonstrated that implementation of routine evaluation of HRQoL is feasible, increases awareness of physicians for the importance of QoL, and can have a positive impact on the well-being of patients. Recently, Basch et al304 showed that self-evaluation of symptoms could significantly improve QoL during treatment, decrease emergency admissions, and even improve survival of patients with advanced cancers. The possible negative impact of treatment on QoL due to AEs should be considered and balanced against the possible positive effects of treatment to reduce or delay cancer symptoms. Regular PRO measurement can help to evaluate the benefit a patient has and can expect from the treatment, and can follow the side effects of the treatments (in order to help the physician make adjustments to therapy).
Recommendation 20.5
PROs and HRQoL should be integrated into the decision-making and the evaluation of treatment efficacy in all patients with recurrent ovarian cancer.
Level of evidence: V
Strength of recommendation: A
Consensus: 100% (34) yes, 0% (0) no, 0% (0) abstain (34 voters)
Recommendation 20.6
Follow-up of QoL and symptoms should be integrated into routine practice.
Level of evidence: V
Strength of recommendation: A
Consensus: 100% (34) yes, 0% (0) no, 0% (0) abstain (34 voters)
Psycho-Oncological Support
Ovarian cancer is a life-threatening condition and its treatment may produce significant toxicities, which cause substantial short- and long-term side effects and functional loss in various behavioural and life domains, as well as psychosocial distress. Therefore, QoL and functional status of the patient may be substantially reduced. In coping and adjusting to life with cancer, women and their families face multiple challenges.
Early detection of psychosocial distress, sexual dysfunction and psychiatric comorbidity, as well as identification of psychosocial care needs, are of major importance. A stepped care model of interventions including counseling, psychoeducation, and psychotherapy seems to be the best approach in all areas of psychosocial care for patients with ovarian cancer. To empower patients to cope with physical and psychosocial long-term side effects of disease and therapy and to preserve QoL they should receive a personalised survivorship care plan (see Section 2 of supplementary data, IJGC, available online).
Supplemental material
Acknowledgments
The authors thank Jennifer Lamarre, Claire Bramley, Sarah Escuin, Alexandra Ospanova, Renata Brandtnerova and all ESMO and ESGO staff for their support throughout the whole consensus process. The authors also wish to express sincere gratitude to Annette Hasenburg and Joachim Weis for describing the psycho-oncological aspects in this article.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- 114.↵
- 115.↵
- 116.↵
- 117.↵
- 118.↵
- 119.↵
- 120.↵
- 121.↵
- 122.↵
- 123.↵
- 124.↵
- 125.↵
- 126.↵
- 127.↵
- 128.↵
- 129.↵
- 130.↵
- 131.↵
- 132.↵
- 133.↵
- 134.↵
- 135.↵
- 136.↵
- 137.↵
- 138.↵
- 139.↵
- 140.↵
- 141.↵
- 142.↵
- 143.↵
- 144.↵
- 145.↵
- 146.↵
- 147.↵
- 148.↵
- 149.↵
- 150.↵
- 151.↵
- 152.↵
- 153.↵
- 154.↵
- 155.↵
- 156.↵
- 157.↵
- 158.↵
- 159.↵
- 160.↵
- 161.↵
- 162.↵
- 163.↵
- 164.↵
- 165.↵
- 166.↵
- 167.↵
- 168.↵
- 169.↵
- 170.↵
- 171.↵
- 172.↵
- 173.↵
- 174.↵
- 175.↵
- 176.↵
- 177.↵
- 178.↵
- 179.↵
- 180.↵
- 181.↵
- 182.↵
- 183.↵
- 184.↵
- 185.↵
- 186.↵
- 187.↵
- 188.↵
- 189.↵
- 190.↵
- 191.↵
- 192.↵
- 193.↵
- 194.↵
- 195.↵
- 196.↵
- 197.↵
- 198.↵
- 199.↵
- 200.↵
- 201.↵
- 202.↵
- 203.↵
- 204.↵
- 205.↵
- 206.↵
- 207.↵
- 208.↵
- 209.↵
- 210.↵
- 211.↵
- 212.↵
- 213.↵
- 214.↵
- 215.↵
- 216.↵
- 217.↵
- 218.↵
- 219.↵
- 220.↵
- 221.↵
- 222.↵
- 223.↵
- 224.↵
- 225.↵
- 226.↵
- 227.↵
- 228.↵
- 229.↵
- 230.↵
- 231.↵
- 232.↵
- 233.↵
- 234.↵
- 235.↵
- 236.↵
- 237.↵
- 238.↵
- 239.↵
- 240.↵
- 241.↵
- 242.↵
- 243.↵
- 244.↵
- 245.↵
- 246.↵
- 247.↵
- 248.↵
- 249.↵
- 250.↵
- 251.↵
- 252.↵
- 253.↵
- 254.↵
- 255.↵
- 256.↵
- 257.↵
- 258.↵
- 259.↵
- 260.↵
- 261.↵
- 262.↵
- 263.↵
- 264.↵
- 265.↵
- 266.↵
- 267.↵
- 268.↵
- 269.↵
- 270.↵
- 271.↵
- 272.↵
- 273.↵
- 274.↵
- 275.↵
- 276.↵
- 277.↵
- 278.↵
- 279.↵
- 280.↵
- 281.↵
- 282.↵
- 283.↵
- 284.↵
- 285.↵
- 286.↵
- 287.↵
- 288.↵
- 289.↵
- 290.↵
- 291.↵
- 292.↵
- 293.↵
- 294.↵
- 295.↵
- 296.↵
- 297.↵
- 298.↵
- 299.↵
- 300.↵
- 301.↵
- 302.↵
- 303.↵
- 304.↵
- 305.↵
Footnotes
Funding All costs relating to the consensus conference were covered from ESMO and ESGO funds. There was no external funding of the event or manuscript production.
Disclaimer These consensus statements were developed by the European Society for Medical Oncology (ESMO) and the European Society of Gynaecological Oncology (ESGO) and are published jointly in the Annals of Oncology and the International Journal of Gynecological Cancer. The two societies nominated participants who attended the consensus conference and co-authored the final manuscript.
DISCLOSURE NCol has reported advisory roles for Roche, PharmaMar, AstraZeneca Clovis, Tesaro, Pfizer, Takeda and Biocad and speaker’s honoraria from Roche, PharmaMar, AstraZeneca and Tesaro; CS has reported advisory board for Clovis; AdB has reported advisory boards and/or lectures (without being member of a speakers’ bureau) for Roche, AstraZeneca, Pfizer, Tesaro, Clovis, BioCad and Genmab/Seattle Genetics; JL has reported research grants from AstraZeneca and MSD/Merck, speaker’s bureau from AstraZeneca and Clovis Oncology and advisory boards for AstraZeneca, Pfizer, Clovis Oncology, Tesaro and Merck/MSD; IMN has reported advisory roles for AstraZeneca, Clovis, Tesaro and Takeda; SP has received honoraria from Roche, AstraZeneca, Clovis, Tesaro, MSD and Pfizer and reported research funding from Roche; IRC has reported conducting clinical studies sponsored by AstraZeneca and Roche; IV has reported advisory boards for Advaxis Inc., Eisai Inc., MSD Belgium, Roche NV, Genmab A/S, Genmab US, F. Hoffmann-La Roche Ltd, PharmaMar, Millennium Pharmaceuticals, Clovis Oncology Inc., AstraZeneca NV, Tesaro Bio GmbH, Tesaro Inc., Oncoinvent AS, Immunogen Inc. and conducting research sponsored by Amgen and Roche; TB has reported research grant from Amgen, travel expenses from Amgen and Roche and advisory board membership for Tesaro; SB has reported educational grants, advisory boards, travel expenses and/or lectures for AstraZeneca, Clovis, Gamamabs, Merck, PharmaMar, Seattle Genetics, Roche, Tesaro and Janssen-Cilag; PB has received honoraria for lectures and written opinions from Roche Polska and AstraZeneca Polska; NCon has reported funding for travel, accommodations and expenses from Roche, Genmab and Amgen and consulting or advisory role with Seattle Genetics and AstraZeneca; RG has reported consultancy/advisory boards for AstraZeneca, Tesaro, Clovis, Sotio, Roche and Immunogen; research funding from Lilly/Ignyta, Boehringer Ingelheim and Roche; expenses to attend meetings from AstraZeneca, Tesaro and Roche and participation in research sponsored by AstraZeneca, Tesaro, Clovis, Immunogen and Pfizer; AGM has reported that he is a member of advisory boards for AstraZeneca, Clovis, Tesaro, Roche, PharmaMar, Immunogen, Genmab, Pfizer/Merck and MSD and speaker’s fees for Roche, AstraZeneca, Tesaro and PharmaMar; FJ has reported advisory boards, travel expenses and lectures for Tesaro and AstraZeneca; FK has reported educational grants from PharmaMar; DL has reported advisory boards for AstraZeneca, Merck, Clovis and Tesaro and institutional research support from PharmaMar and Clovis; SM has reported research support, advisory board, honoraria and travel expenses from AstraZeneca, Clovis, Medac, MSD, Novartis, PharmaMar, Roche, Sensor Kinesis, Tesaro and Teva; MRM has reported links (not specified) with Advaxis, AstraZeneca, Boehringer Ingelheim, Clovis Oncology, Genmab, Karyopharm, Novocure, Pfizer, Roche, Seattle Genetics, Tesaro, Oncology and Sera Prognostics; SN has reported advisory boards for Roche, Tesaro, AstraZeneca and Clovis and research funding from AstraZeneca; DOD has received financial support for travel and accommodation costs from AstraZeneca; PP has reported conducting a clinical study sponsored by PharmaMar; JS has reported advisory boards and lectures for PharmaMar, AstraZeneca, Clovis, Roche and Tesaro; DSPT has reported conducting research sponsored by Roche, AstraZeneca and Pfizer, receiving research funding by AstraZeneca and received honoraria from Roche and AstraZeneca; WGMC, PM, IB, AD, SO, FP, DQ, IB, DC, NC, BD, MDS, AF, VHS, JWK, MM, AR, FS, NS, DT, GT, JvdV, POW and AZ have reported no conflicts of interest.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.