Article Text

Abstract
Objective To investigate the prognostic factors for survival and toxicities in elderly (≥65 years) patients with endometrial cancer who underwent post-operative radiotherapy. Additionally, to compare the treatment outcomes between the older elderly (≥75 years) and younger elderly (65–74 years) patients.
Methods Medical records of patients with enometrial cancer treated between January 1998 and July 2019 were reviewed. Patients with stage IA to IIIC2, all histology subtypes, and any grade were included. All patients underwent total abdominal hysterectomy and received adjuvant radiotherapy with or without chemotherapy. All but 67 (8.4%) of 801 patients had lymph node dissection. Clinicopathological factors and treatment strategies were compared between the two age groups. The prognostic factors for overall survival and progression-free survival were investigated.
Results A total of 801 patients with enometrial cancer, 627 patients (78.3%) younger elderly and 174 patients (21.7%) in the older elderly group were included. Median follow-up was 74.3 months (range 0.4–224.6). The older elderly patients had significantly higher rates of grade 3 tumors (51.7% vs 40.8%; p=0.04), cervical glandular involvement (21.8% vs 14.0%; p=0.03), and cervical stromal invasion (34.5% vs 27.9%; p=0.04) than the younger elderly patients. The rates of lymph node dissection (p=0.2), radiotherapy modalities (p=0.92), and systemic chemotherapy (p=0.2) did not differ between the two groups. The 5-year locoregional control and distant metastasis rates were 88.3% and 23.8%, respectively. The 5-year cause-specific survival and progression-free survival rates for younger and older elderly patients, were 79.8% vs 74.3% (p=0.04) and 67.5% vs 57.8% (p<0.001), respectively. In multivariate analysis, larger tumor size, non-endometrioid histology, cervical stromal involvement, and stage III disease were associated with poor cause-specific survival and progression-free survival. Age was an independent predictor of worse progression-free survival, but not of cause-specific survival. There was no significant difference in acute and late gastrointestinal and genitourinary toxicities between age groups.
Conclusions Post-operative radiotherapy for elderly patients with endometrial cancer is effective and well tolerated. Advanced age should not preclude appropriate treatment, especially in those with adequate quality of life, life expectancy, and functional status.
- radiotherapy
- endometrium
Data availability statement
Data are available upon reasonable request.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Despite the fact that the incidence of endometrial cancer has increased and will continue to rise in the aging population, its treatment in the elderly remains debatable.
WHAT THIS STUDY ADDS
Older elderly patients have worse tumor characteristics than younger elderly patients, indicating that older elderly patients require more adjuvant therapies. All treatments were well tolerated by elderly patients, with no significant differences in toxicity rates between younger and older elderly patients.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Based on the risk factors and co-morbidity scores evaluated prior to radiotherapy, our findings suggest that elderly patients should be treated with adjuvant radiotherapy, with or without chemotherapy. Age should not be a barrier to appropriate treatment, especially for those with a reasonable quality of life, life expectancy, and functional status.
INTRODUCTION
Endometrial cancer is the most common gynecologic cancer, and it is frequently diagnosed in elderly patients.1 Nearly two-thirds of patients with endometrial cancer in developed countries are over 65 years old at the time of diagnosis, and the incidence is rising as life expectancy increases worldwide.2 3 Several studies have shown that older age is an indicator of a poor prognosis in patients with endometrial cancer.4 5 Although older age at diagnosis is associated with more aggressive tumor characteristics, necessitating more aggressive treatment strategies, previous studies have shown that elderly women with endometrial cancer undergo less aggressive surgery and adjuvant therapy than their younger counterparts.6 7 However, it is unclear whether the poor outcome in elderly patients with endometrial cancer is entirely due to a more advanced stage at the time of diagnosis, poor prognostic factors, a lack of radical treatments, and co-morbidities, or whether endometrial cancer in the elderly is inherently more aggressive than in younger patients.
Adjuvant radiotherapy is recommended both in patients with early stage and locally advanced endometrial cancer to improve locoregional control.8 9 Previous studies have investigated the use and outcomes of adjuvant radiotherapy in elderly women with both early and advanced stage endometrial cancer.2 6 10 Radiotherapy is well tolerated by elderly patients with endometrial cancer, with more than 90% of patients completing their treatments.11 12 However, the treatment and toxicity outcomes of elder patients with endometrial cancer treated with adjuvant radiotherapy has been rarely evaluated.3 13 A few reports have described an increase in radiotherapy complications, while others have indicated that the incidence of complications among older populations is comparable to that of younger populations.3 13
Based on these findings, we conducted a multi-institutional retrospective analysis with patients undergoing relatively similar treatment strategies to investigate the impact of adjuvant radiotherapy on outcomes in elderly patients with endometrial cancer in the hopes of providing more information on survival benefit and toxicity.
METHODS
Patient Selection
We reviewed the electronic medical records of 801 patients with endometrial cancer aged 65 or older treated at three academic hospitals between January 1998 and July 2019. All patients underwent a total hysterectomy, bilateral salpingo-oophorectomy, with or without pelvic and para-aortic lymph node dissection. Patients with distant metastases, neoadjuvant chemotherapy prior to surgery, previous pelvic irradiation, and ineligibility for adjuvant radiotherapy were excluded from the study. This study was approved by Baskent University Institutional Review Board (Project no: KA20/62).
Treatment Protocol
All patients were treated in accordance with the clinicians’ practices and department policies. Depending on the disease stage, patient performance status, and risk factors, patients received post-operative external radiotherapy or vaginal cuff brachytherapy only, external radiotherapy in conjunction with brachytherapy, or radiotherapy with chemotherapy.
All patients received adjuvant radiotherapy using either three-dimensional conformal radiotherapy or intensity-modulated radiotherapy. Over a 5-week period, the median dose of external radiotherapy was 50.4 Gy (range 41.4–60 Gy), with a daily median fraction size of 1.8 Gy (range 1.8–2 Gy).14 Patients with para-aortic lymph node metastasis also received irradiation to the para-aortic field. Brachytherapy was administered to the vaginal cuff using either a two-dimensional or three-dimensional technique with a high dose rate afterloading system. The vaginal proximal 3–5 centimeters were treated, and the dose was prescribed to the vaginal mucosa or 5 mm below the surface of the cylinder. The median fraction dose, fraction number, and total brachytherapy dose were 5.5 Gy (range 3.0–7.5 Gy), 5 fractions (range 2–7 fractions), and 25 Gy (range 12–35 Gy), respectively.
Patients with high-risk characteristics, such as lymph node metastasis or non-endometrioid histology, also received adjuvant chemotherapy and radiotherapy sequentially or sandwich-style, as previously defined.15 The chemotherapy protocols were designed in accordance with institutional protocol and primarily consist of paclitaxel and carboplatin for up to six cycles or paclitaxel alone for up to 12 weeks.
During the treatment period, treating physicians graded the acute toxicities each week. Acute and late toxicities were defined as any event occurring within 90 days of the beginning of radiotherapy and beyond 90 days, respectively. Treatment toxicities were assessed according to the ‘Common Terminology Criteria for Adverse Events’, version 4.0. Late toxicity was scored according to ‘Late effects on normal tissues-Subjective Objective Management Analytic’. The acute gastrointestinal system toxicities, nausea, diarrhea, and proctitis, were recorded, while dysuria and cystitis were used to define acute genitourinary system toxicities. Toxicities were reported as the absolute number of patients and their relative rates.
Statistical Analysis
For statistical analysis, SPSS 22.0 (SPSS for Windows, IBM Corp., Armonk, New York, USA) and MedCalc version 20.111 (MedCalc Software Ltd., Ostend, Belgium) were used. The primary endpoints were cause-specific survival and progression-free survival, while secondary endpoints included local control, distant metastasis, and acute and late toxicities. Cause-specific survival was computed using the interval between the date of diagnosis and the date of cancer-related death or the most recent follow-up. Progression-free survival was determined by subtracting the last day of radiotherapy from the date of radiological detection of local progression, distant metastases, or death, whichever occurred first. According to the age cut-off point of 75 years, patients were divided into two groups: younger elderly (from 65 to 74 years) and older elderly (75 years and older). The χ2 test or Student’s t-test was used to compare clinical and pathological factors between two groups. Overall survival, progression-free survival, and local control rates were calculated using the Kaplan-Meier method. Univariate analysis was performed using the log-rank test. Covariates with a p value <0.05 in the univariate analysis were included in the Cox proportional hazards model for multivariate analyses. Those p values lower than 0.05 were deemed statistically significant.
RESULTS
Patient Characteristics
Table 1 summarizes the patient, tumor, and treatment characteristics for the entire cohort and by age group. Median ages for the entire patient population, younger elderly and older elderly groups were 69 years (range 65–90), 68 years (range 65–74), and 77 years (range 75–90), respectively. Patients in the older age group had significantly higher rates of grade 3 tumor, cervical glandular involvement, and cervical stromal invasion than those in the younger age group.
Patient and tumor characteristics for the entire cohort and by patient age group
The rate of lymph node dissection, adjuvant radiotherapy modalities, and systemic chemotherapy were not significantly different between two groups. Lymph node dissection was performed in 91.6% (n=734) of all patients, 92.5% (n=580) of younger elderly and 88.5% (n=154) of older elderly patients. The median number of dissected lymph nodes was 33 (range 1–164) in the entire cohort, with younger elderly patients having significantly more lymph nodes dissected (34, range 1–164) than older elderly patients (28, range 1–136) (p=0.04). Brachytherapy was administered to 649 patients, with no statistically significant difference between the younger and older elderly groups (81.3% vs 79.9%; p=0.37).
Treatment Outcomes
Median follow-up time for the entire cohort was 74.3 months (range 0.4–224.6). Disease progression was observed in 214 patients (26.7%). Of these patients, 38 (17.8%) had local or locoregional failure, 138 (64.5%) developed distant metastasis, and 38 (17.8%) had both local recurrence and distant metastasis. At last follow-up, 523 patients (65.3%) were alive (40 patients (5%) with disease), and 278 patients (34.7%) had died (176 patients (22%) with disease and 102 patients (12.7%) without disease). A total of 129 patients (20.6%) in younger elderly group and 47 patients (27%) in older elderly group died because of endometrial cancer (p=0.04). The rate of death from other causes was significantly higher in older age groups than in younger age groups (20.1% vs 10.7%; p=0.001).
The 1- and 2 year recurrence rates for patients who remain alive were 12.2% and 13.8%, respectively. There was no difference in 1-year (12.1% vs 12.3%; p=0.51) and 2-year recurrence rates (13.9% vs 13.5%; p=0.43) between younger elderly and older elderly patients who were still alive at the time of the last visit.
Cause-specific Survival and Progression-free Survival
The 5-year cause-specific survival and progression-free survival rates for the entire cohort were 78.6% and 65.5%, respectively. The median cause-specific and progression-free survival times were 16.9 years (95% CI 14.2 to 18.6 years) and 9.2 years (95% CI 7.4 to 11.1 years), respectively. The 5-year cause-specific survival rate was significantly higher in younger elderly patients than in older elderly patients (79.8% vs 74.3%; p=0.04, Figure 1A). Similarly, the 5-year progression-free survival rates in younger elderly patients were significantly higher than in older elderly patients (67.5% vs 57.8%; p<0.001, Figure 1B).

Kaplan-Meier plots of (A) cause-specific survival (CSS) and (B) progression survival (PFS) for patients aged 65 to 74 years (blue line) and ≥75 years (yellow line).
Tumor size, histology, tumor grade, lymphovascular space invasion, depth of myometrial invasion, cervical glandular and stromal invasion, lymph node metastasis, and International Federation of Gynecology and Obstetrics (FIGO) stage were significant prognostic factors for cause-specific survival and progression-free survival on univariate analysis (Table 2). Age is an additional prognostic factor for progression-free survival. In multivariable analysis, larger tumor (>4 cm), non-endometrioid histology, cervical stromal invasion, and FIGO stage III disease (Figure 2) were all negative predictors of cause-specific survival and progression-free survival; older age is an additional predictor for worse progression-free survival. In multivariable analysis, we were unable to demonstrate the significance of age on cause-specific survival. Age as a continuous variable was also a significant prognostic factor for progression-free survival (HR=1.07, 95% CI 1.02 to 1.12; p=0.005) in multivariable analysis. Grade 3 disease was also associated with poor overall survival and progression-free survival, but only marginally.
{kind=link}
{kind=link}
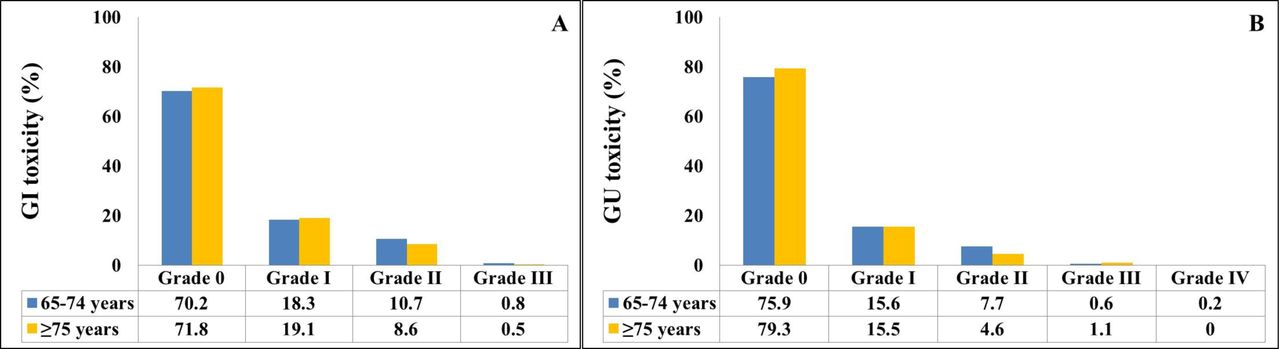
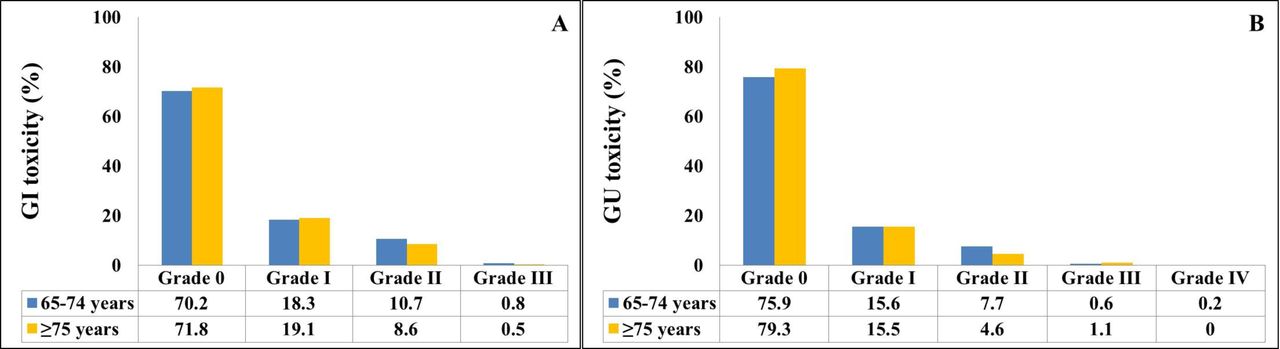
Bar graphics demonstrating the incidence of (A) acute gastrointestinal (GI) toxicity and (B) acute genitourinary (GU) toxicity.
Prognostic factors for overall survival and progression-free survival
Local Recurrence and Distant Metastasis
The 5-year locoregional control rate was 88.3% and the distant metastasis rate was 23.8%. The 5-year locoregional control rates for younger and older elderly patients were 88.3% and 88%, respectively (p=0.73). Similarly, there was no difference in distant metastasis rates between two age groups (23.9% vs 24.4%; p=0.29). In multivariate analysis, tumor size greater than 4 cm and a FIGO stage III disease were associated with a higher risk of locoregional recurrence (online supplemental Table). A multivariate analysis revealed that a higher tumor grade, glandular and stromal invasion of the cervical cavity, and the presence of lymph node metastasis were all significant predictors of distant metastasis.
Supplemental material
Toxicity
There was no significant difference in acute and late gastrointestinal and genitourinary toxicities at any grade between age groups (29.8% vs 28.2%; p=0.86, Figure 2). Most patients did not experience severe adverse events that necessitated the cessation of radiotherapy, except for one (0.2%) patient in the younger elderly group who developed grade 4 genitourinary toxicity (vesicovaginal fistula). Late grade 2 or higher complications occurred in 40 patients (5.0%) for entire cohort. There was no significant difference in grade 2 or higher late toxicities between younger elderly and older elderly patients (4.6% vs 6.3%; p=0.43).
DISCUSSION
Summary of Main Results
In this study, we found that older elderly patients with endometrial cancer had a lower survival rate than their younger elderly counterparts, despite receiving similar treatments. This may be due to high risk factors and potential co-morbidities. Additionally, elder patients tolerated all treatment well with no significant difference in toxicity rates between younger elderly and older elderly patients. Because the majority of patients had high-risk features, our findings suggest that older age should not preclude appropriate treatment, particularly in those with a reasonable quality of life, life expectancy, and functional status.
Results in the Context of Published Literature
The treatment of elderly patients with endometrial cancer will become a significant challenge for physicians due to the permanent aging of the population and the rising incidence of endometrial cancer in older women.12 16 A number of factors contribute to the higher mortality rate among elderly patients with endometrial cancer, including late presentation at diagnosis, increased disease aggressiveness, and undertreatment of elderly patients.17 Previous studies found that older patients with tumors had unfavorable prognostic factors like non-endometrioid histology, grade 3 tumors, more aggressive immunological characteristics, and more aggressive disease than younger patients.5 18 19 These findings are consistent with our findings. We demonstrated that older women were more likely to have non-endometrioid histology, grade 3 disease, cervical glandular and stromal invasion, which was reflected in an increase in the proportion of older women with an intermediate or high risk of recurrence.
According to current guidelines, older patients are more likely than younger patients to receive adjuvant treatment and lymphadenectomy in this context.6 9 However, older women have been underserved, which may be contributing to their low survival rates. According to the literature, lymphadenectomy, radiotherapy, and systemic treatment are less likely to be performed in older women.2 6 7 16 However, the majority of studies demonstrated that patients over the age of 65 were not lost due to co-morbidities, indicating that age may not have been the primary factor related to the survival of elderly patients with endometrial cancer after correct treatment.3 20 In order to evaluate the outcomes of elderly patients, this study evaluated only patients who received post-operative radiotherapy. The rates of lymph node dissection, radiotherapy modalities, vaginal vault brachytherapy, and systemic chemotherapy were not statistically different between the two groups.
Numerous studies have examined the effects of advanced age on endometrial cancer, with contradictory findings (Table 3).2 3 12 19–22 In a German Cancer registry trial, Eggemann et al12 analyzed the overall survival rates of 1550 patients with endometrial cancer. With a median follow-up of 76.8 months, the authors discovered that the 10-year disease-specific overall survival was 77.1% for patients younger than 70 years and 58.9% for patients older than 71 years of age (p<0.001). In a National Cancer Database trial evaluating 20 468 patients with endometrial cancer with advanced stage (3 and 4) disease, Raul-Hain et al2 found that the median overall survival for patients aged 60–74 years, 75–84 years, and 85 years or older was 28.6 months, 20.5 months, and 5.4 months, respectively. Rovirosa et al3 found a significant difference in 5-year cause-specific survival between the patients aged ≥65 years and younger patients (p=0.006) in 438 patients with endometrial cancer receiving post-operative radiotherapy.
Different definitions of age as an older population, various treatment strategies, and various study endpoints contribute to a wide range of results across studies. In addition, the majority of studies evaluated patients who received inadequate treatment. Although the definition of ‘elderly’ varies, the World Health Organization (WHO) uses the age of 65 as a cut-off point for elderly classification. Therefore, we preferred to use the age of 65 to define elderly patients. Instead of comparing patients younger than 65 years and older than 65 years, we evaluated all elderly patients and stratified them into younger elderly, aged 65 to 74 years, and older elderly, aged 75 or older. We found that age, both as a cut-off value and as a continuous variable, was a significant predictor of worse progression-free survival, but not of cause-specific survival. We found that larger tumor size, non-endometrioid histology, cervical stromal invasion, and FIGO stage 3 disease were more predictive of overall survival and progression-free survival than undertreatment in elderly patients.
Published data on elderly endometrial cancer
Some studies looked at the effect of co-morbidity scores on the survival of elderly patients with endometrial cancer.3 21 However, due to the retrospective nature of these studies, most of the available data do not mention co-morbidity scores, as in our current study. For this elderly population, the main obstacle to co-morbidity may be the aggravation of radiation toxicity. In conjunction with our findings, other research has demonstrated that acute radiation toxicity is moderate and independent of co-morbidity scores. In addition, in our study, there was no difference in acute and late radiation-related toxicities between older elderly patients with endometrial cancer and their younger counterparts.
Strengths and Weaknesses
The current study’s strengths include a large sample size with a longer follow-up period and its multicentric nature. Furthermore, even though the study population consisted of elderly patients with enometrial cancer, all patients underwent complete surgical staging. Last, we assessed survival and also progression patterns in order to better evaluate the prognostic factors influencing survival as well as local and distant recurrence.
Our study has some limitations that should be mentioned. First and foremost, due to its retrospective design, we did not perform any comprehensive geriatric assessment prior to radiotherapy. Second, we included all stages and histopathologies of endometrial cancer. Third, the estimation of overall toxicity may be inaccurate because toxicity analysis was performed retrospectively using patient records. We were able to analyze only acute gastrointestinal and genitourinary system toxicities; hematological toxicities and pelvic bone insufficiency fractures seen as late complications were not taken into account, and we were unable to report toxicities in detail. Finally, because we evaluated only patients aged 65 and over, we were unable to compare our findings with those of younger patients.
Implications for Practice and Future Research
The tumor characteristics of older elderly patients are worse than those of younger elderly patients, indicating that older elderly patients require more adjuvant treatments. Although older age is a detrimental factor for survival, we recommend that elderly patients be treated with adjuvant radiotherapy, with or without chemotherapy, based on risk factors and co-morbidity scores evaluated prior to receiving radiotherapy. However, larger prospective randomized trials with well-defined patient populations will be required to confirm our findings.
CONCLUSIONS
In this study, we demonstrated that adjuvant radiotherapy is a safe and effective treatment option for patients with endometrial cancer undergoing total abdominal hysterectomy with or without lymph node dissection. The elderly patient population is more likely to have high-risk factors and co-morbidities than the younger patient population, but this should not prevent the provision of adjuvant treatment modalities.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Baskent University Institutional Review Board (Project No: KA20/62) and supported by Baskent University Research Fund. Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors GY and CO established the study design, participated in data analysis, and revised, wrote the manuscript, and approved the final manuscript. OCG, EO, SYS participated in data acquisition and analysis, MG, FY, CO performed data and statistical analyses, and approved the final manuscript. CO is the guarantor of this study.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.