Article Text

Abstract
Objective To examine the utilization of hormone replacement therapy (HRT) among newly diagnosed cervical cancer patients who experienced premature menopause due to primary treatment.
Methods The MarketScan Databases were used to identify newly diagnosed cervical cancer patients <50 years of age with premature menopause after hysterectomy with bilateral salpingo-oophorectomy (primary surgery) or primary external beam pelvic radiation (primary radiotherapy). We examined the cumulative utilization of HRT until 24 months after the loss of ovarian function. Fine-Gray subdistribution hazard models were developed to examine the factors associated with cumulative HRT use. The duration of HRT use was analyzed by Kaplan-Meier curves.
Results A total of 1826 patients, including 352 (19.3%) who underwent primary surgery and 1474 (80.7%) who received primary radiotherapy, were identified. Overall, 39.0% of patients received HRT within 24 months of primary treatment. HRT was used in 49.4% of those who underwent primary surgery and in 36.6% of those who received primary radiotherapy (p<0.0001). The median duration of HRT use was 60 days among the entire cohort and was significantly shorter for the primary radiotherapy group than the primary surgery group (35 vs 90 days, p<0.0001). Primary radiotherapy, older age, residency in the Northeastern USA, and Black race were associated with a lower likelihood of HRT use.
Conclusions HRT was prescribed to less than half of patients with newly diagnosed cervical cancer under the age of 50 who experienced premature menopause due to primary treatment. Among those who used HRT the duration of use was short.
- cervical cancer
- palliative care
- hysterectomy
- radiation
Data availability statement
No data are available. Embargo on data due to commercial restrictions.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Little is known about the use of hormone replacement therapy (HRT) among newly diagnosed cervical cancer patients who experienced premature menopause due to primary treatment.
WHAT THIS STUDY ADDS
Overall, 39.0% of patients received HRT within 24 months of primary treatment. The median duration of HRT use was 60 days
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Strategies to enhance HRT use among cervical cancer patients may improve quality of life and prevent long-term sequelae of estrogen deprivation.
Introduction
The median age of patients with cervical cancer is 50 years1 and, of the 13 000 patients with newly diagnosed cervical cancer in the USA each year,2 approximately 50% are pre-menopausal.2 3 While some younger patients may be candidates for fertility-sparing treatment options, primary therapy for cervical cancer most commonly involves either hysterectomy, often in combination with bilateral oophorectomy, or primary chemoradiation.4 5 Both treatments result in estrogen deprivation through surgical menopause or ovarian ablation, respectively.
As the incidence and mortality rates for cervical cancer have declined due to widespread screening and improved treatment options,6 7 there is a growing recognition of the impact that cervical cancer treatments may have on patients’ quality of life and overall health.5 Premature menopause results in symptomatic sequelae as well as potential long-term consequences such as an increased risk of cardiovascular disease, osteoporosis, and neurological and cognitive disorders.4 5 The abrupt decrease in estrogen also causes vasomotor symptoms, mood and sleep disorders, and vulvovaginal symptoms.8
According to the National Comprehensive Cancer Network, hormone replacement therapy (HRT) should be considered among cervical cancer survivors, particularly pre-menopausal patients, as a treatment option for the physical and psychosocial effects related to estrogen deprivation.9 While HRT does not appear to impact oncologic outcomes,10 11 small studies have suggested that HRT is used infrequently in this population.10 12 In their position paper on HRT, the North American Menopause Society noted minimal safety concerns with prescribing HRT to patients with cervical cancer, unless patients have had prior estrogen-sensitive breast or endometrial cancer.13
Given that little is known regarding HRT use among young cervical cancer patients, the objective of this study was to examine the uptake and patterns of HRT use among pre-menopausal patients with newly diagnosed cervical cancer who experienced loss of ovarian function due to primary cancer-directed therapy.
Methods
We analyzed data from the IBM Watson Health MarketScan Research Databases. The database contains more than 350 payers and captures claims from over 273 million enrollees with commercial insurance from all states and 7 million enrollees with Medicaid insurance from 12 US states.14 This study was considered non-human subjects research by our Institutional Review Board.
We identified patients aged 18 to 64 years with newly diagnosed cervical cancer from 2008 to 2019 to include all adults fully covered by commercial or Medicaid insurance. To capture pre-menopausal patients, our final analytical cohort was restricted to patients under 50 years of age (Online supplemental figure 1). We identified cervical cancer patients based on International Classification of Diseases, ninth revision (ICD-9) diagnosis codes (180.x) and ICD-10 diagnosis codes (C53.x). Patients needed to have at least two claims 30 days apart within 180 days since the first cancer claim to be included in the study. We excluded patients who had cancer claims other than gynecological cancer within 180 days before the first cervical cancer claim date. To capture incident cervical cancer, the cohort was limited to subjects who underwent either hysterectomy or external beam radiotherapy (Online supplemental table 1). The surgery group was further limited to patients who underwent bilateral oophorectomy in combination with hysterectomy. Patients in the radiotherapy group who underwent ovarian transposition were excluded. In order to best capture patients’ full utilization of medical services and medication prescriptions, patients had to have continuous health insurance and prescription benefit coverage from 6 months prior, until at least 6 months after primary cancer treatment. Primary treatments are defined as any hysterectomy or radiation within 120 days of the first cancer claim date.
Supplemental material
Supplemental material
The maximum duration of health insurance and drug coverage was noted for each patient after primary treatment. HRT use was defined as any estrogen prescription filled within 24 months since loss of ovarian function due to primary cancer treatment. The index date of loss of ovarian function was defined as the date of bilateral salpingo-oophorectomy for the surgery group or the first date of whole pelvic radiotherapy.
Estrogen replacement therapy medications were identified by collecting generic drug names and national drug codes using the MarketScan RED BOOK.15 We included estrogens commonly used for menopausal HRT and oral contraceptives, and included all formulations of estrogen including oral, transdermal, and vaginal. We captured patients who received either estrogen alone or those who received estrogen in combination with progesterone. For each patient, we captured the time from the index date of loss of ovarian function until the first HRT prescription date and the duration of HRT use. The duration of HRT use was defined as the time period in days from the first estrogen prescription filled until the end of the continuous prescription or until a 30-day interruption of HRT prescriptions.
Clinical and demographic characteristics included year of primary treatment (2008–2010, 2011–2013, 2014–2016, 2017–2019), age group (18–34, 35–39, 40–44, 45–49), race (White, Black, other/unknown), insurance status (commercial, Medicaid), metropolitan statistical area (yes, no, unknown), geographic region of residence (Northeast, North Central, South, West, unknown), and use of adjuvant/concurrent chemotherapy. Pre-existing comorbidities were identified by ICD-9-CM (clinical modification) and ICD-10-CM codes, and classified using the Elixhauser comorbidity score (0, 1, 2, >3). In the MarketScan dataset, information on race and ethnicity was only available for Medicaid beneficiaries, while geographic data, such as metropolitan statistical area (MSA) and region, were only captured for commercially insured patients.
The cumulative utilization of HRT was calculated through a cumulative incidence function (CIF), and Gray’s test was used to compare the CIF curves by primary treatments and age groups. Fine-Gray subdistribution hazard models were developed to examine the association between covariates and cumulative HRT use in the overall cohort and the primary treatment groups. Events were defined as patients receiving HRT within 24 months since loss of ovarian function. Patients were censored if they had a full 2 years of follow-up but did not receive HRT. Patients who were lost to follow-up prior to 2 years after primary treatment without an HRT prescription noted were defined as competing risks given that their HRT use was unknown. The results were reported as adjusted hazard ratios (aHR) with 95% confidence intervals (95% CI).
Among patients who received HRT, we also examined duration of use using Kaplan-Meier curves. Events were defined as the end of HRT use. Patients were censored if they continued to receive the prescription at the end of each observation time-point. Log-rank tests were used to compare median duration of HRT use. All hypothesis tests were two-sided. All analyses were conducted using SAS Studio version 3.71 (SAS Institute Inc, Cary, NC). The figures were created with SAS and R version 4.0.5 (R Core Team, Vienna, Austria).
Results
A total of 1826 patients experienced loss of ovarian function during primary treatment for newly diagnosed cervical cancer, including 352 (19.3%) patients who underwent hysterectomy with bilateral salpingo-oophorectomy and 1474 (80.7%) patients who received pelvic radiation without ovarian transposition. The median age of the cohort was 41 years (IQR 36–46 years). Overall, 350 (19.2%) patients were aged 18–34 years, 387 (22.0%) were 35–39 years, 485 (26.6%) were 40–44 years, and 604 (33.1%) were 45–49 years. The median age was slightly older in the primary surgery group than in the primary pelvic radiation group (43 vs 41 years). Within the cohort, 1215 (66.5%) patients had commercial insurance and 611 (33.5%) were Medicaid recipients. The patients in the primary radiation group were more likely to receive adjuvant or concurrent chemotherapy than those in the primary surgery group (92.8% vs 42.6%, p<0.0001) (Table 1).
Clinical and demographic characteristics of the study cohort by primary treatment
Within 24 months of primary treatment, 39.0% (95% CI 36.8 to 41.3%) of patients received HRT. Patients in the primary surgery group were more likely to receive HRT than those treated with primary radiotherapy (49.4%, 95% CI 44.2 to 54.6% vs 36.6%, 95% CI 34.1 to 39.1%, Gray’s test p<0.0001) (Table 2, Figure 1A). Within 6 months of primary treatment, HRT was initiated in 39.8% (95% CI 34.6% to 44.9%) of patients who underwent primary surgery and in 22.7% (95% CI 20.6% to 24.9%) of patients who received primary radiotherapy.
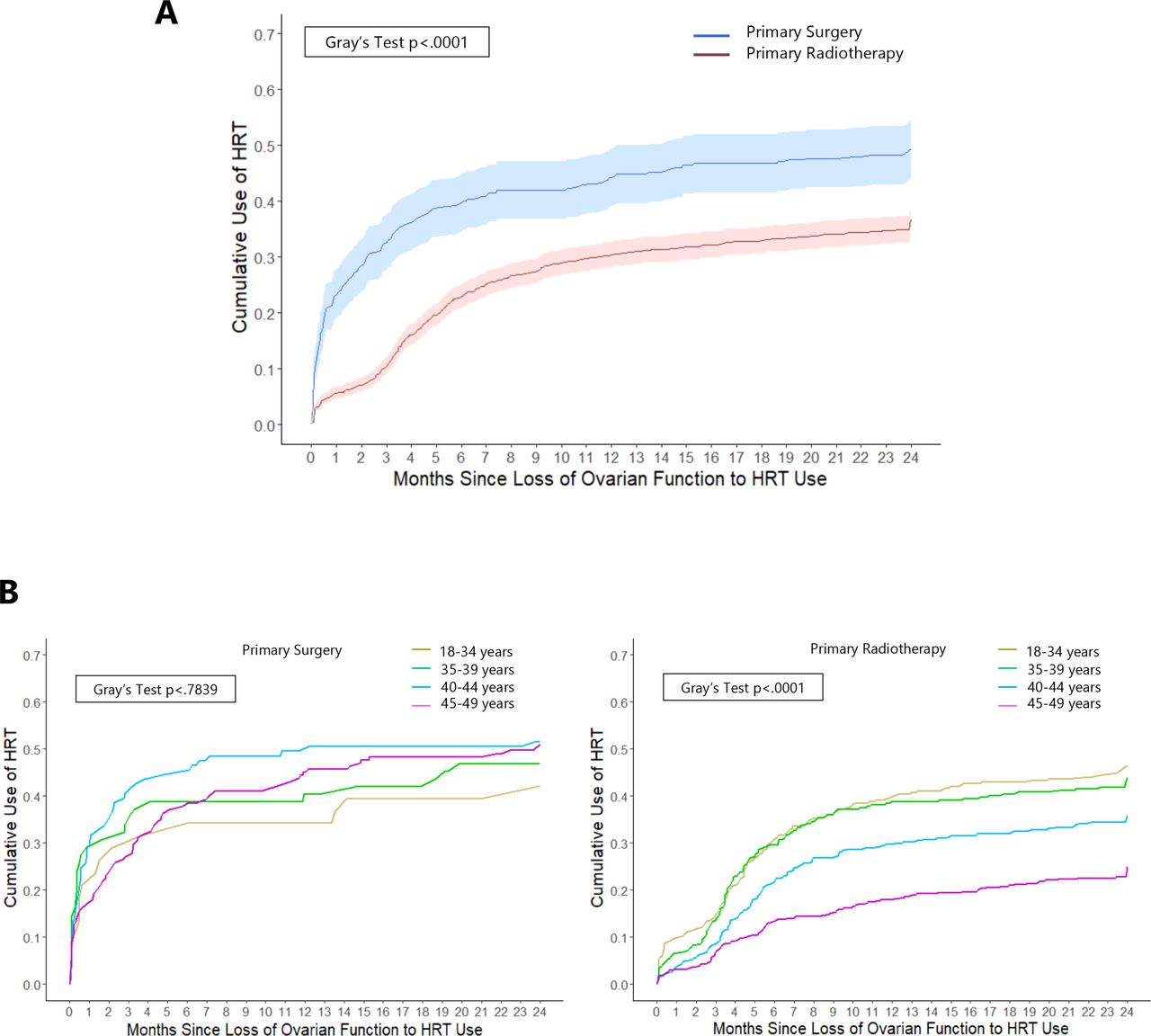
Cumulative utilization of hormone replacement therapy (HRT) since loss of ovarian function stratified by primary treatments (A) and by age groups (B). The shaded area indicates 95% CI.
Cumulative incidence rate of hormone replacement therapy use at 6, 12, 24 months after loss of ovarian function stratified by primary treatment
Within the primary surgery group, HRT was initiated within 24 months in 42.1% (95% CI 26.1% to 57.3%) of patients aged 18–34 years, 46.8% (95% CI 33.9% to 58.7%) of those 35–39 years, 51.5% (95% CI 41.3% to 60.8%) of those 40–44 years, and 51.0% (95% CI 42.7% to 58.7%) of those 45–49 years (Table 2, Figure 1B). The corresponding rates of HRT use by age in the primary radiotherapy group were: 46.5% (95% CI 40.8% to 51.9%), 44.0% (95% CI 38.5% to 49.3%), 35.9% (95% CI 31.2% to 40.7%), and 24.9% (95% CI 21.1% to 29.0%) (Table 2, Figure 1B, Gray’s test p<0.0001).
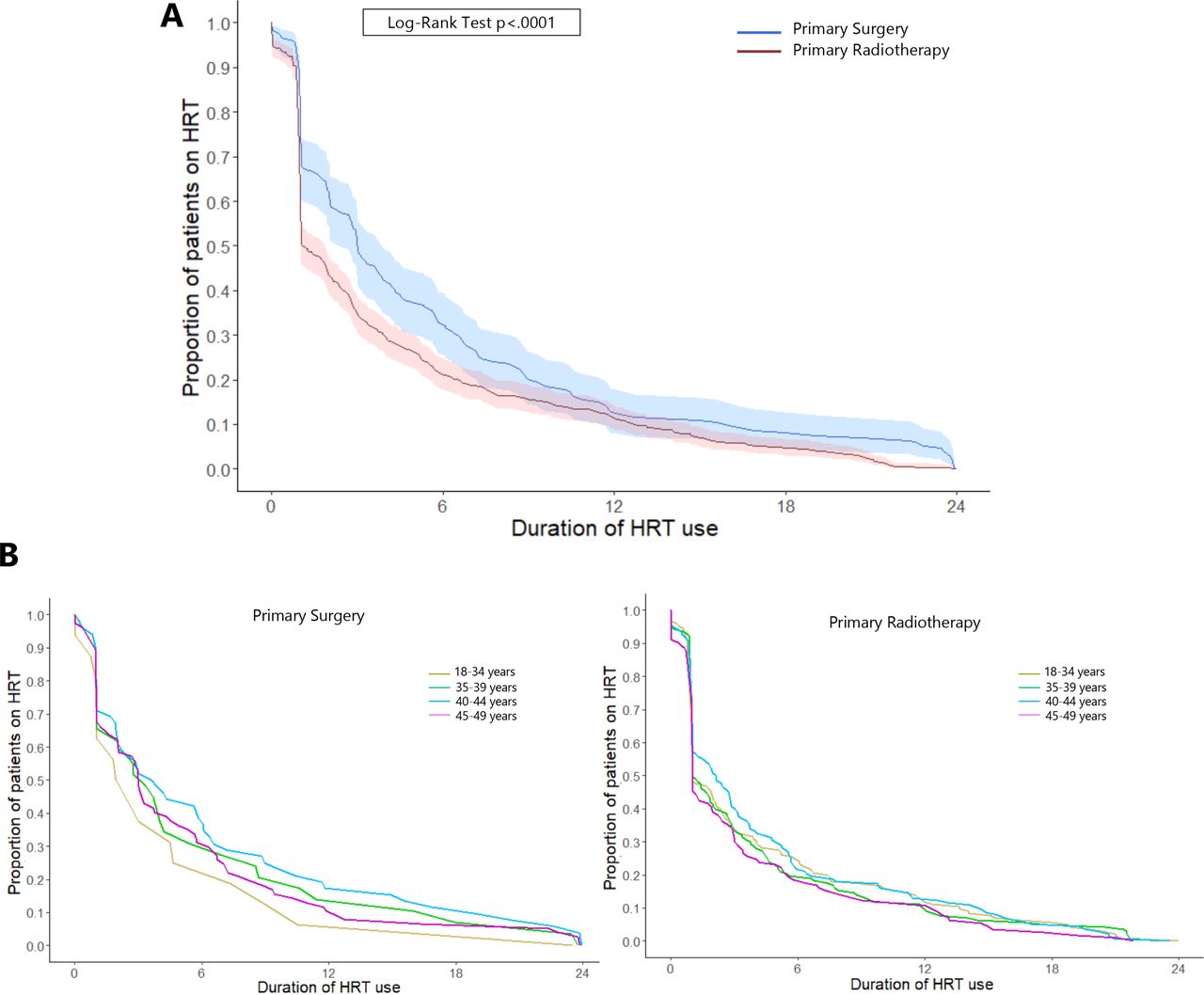
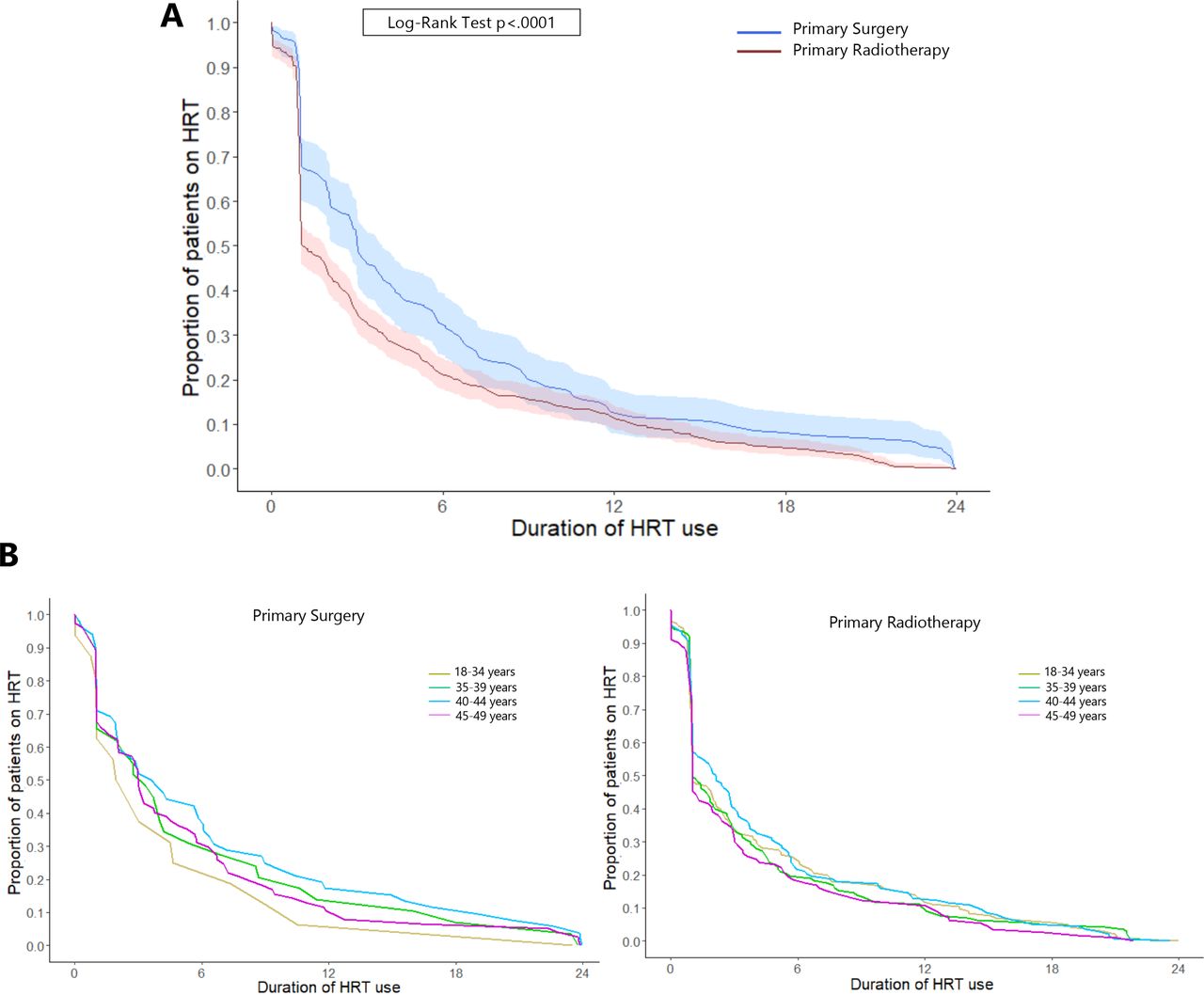
The median duration of HRT use was 60 days (IQR 30–182) for the entire study population. Patients in the primary surgery group had a longer median duration of HRT use than those treated with primary radiotherapy (90 days (IQR 30–220) vs 35 days (IQR 28–156), log-rank test p<0.0001) (Figure 2).
{kind=link}
{kind=link}
Proportion of patients on hormone replacement therapy (HRT) by duration of HRT use stratified by primary treatments (A) and by age groups (B). The shaded area indicates 95% CI.
In a multivariable Fine-Gray subdistribution hazard model, patients treated with pelvic radiotherapy were 32% less likely to receive HRT than patients who underwent primary surgery (aHR 0.68, 95% CI 0.55 to 0.85) after adjusting for other covariates. Younger age and residency in the West and South were associated with an increased likelihood of HRT use compared with older age and residency in the northeastern USA, respectively. Black patients were 36% less likely to receive HRT than White patients (aHR 0.64, 95% CI 0.47 to 0.88) (Table 3). Almost 70% of the patients had missing data on their race, and around 35% of the patients had missing data on their residency. In a sub-analysis limited to either those treated with surgery or radiotherapy, results were similar, except that no association was observed between patient age and HRT use in the primary surgery group (Table 3).
Multivariable fine-Gray subdistribution hazard models of hormone replacement therapy use in the overall cohort and stratified by primary treatment
Discussion
Summary of Main Results
We noted that less than 40% of newly diagnosed cervical cancer patients under 50 years of age who experienced loss of ovarian function received HRT within 2 years of primary cancer directed treatment. The patients who received pelvic radiotherapy as a primary curative treatment were considerably less likely to be prescribed HRT than those who underwent primary surgery with bilateral salpingo-oophorectomy. Given the well-known short- and long-term sequelae induced by ovarian failure, it is recommended that cervical cancer patients under 50 years old be offered HRT until the age of expected natural menopause in the absence of known risk factors or contraindications.13 16 Nevertheless, the rate of HRT use in our study cohort was less than 50%, even among patients under 40 years of age. Additionally, among patients who received HRT, the median duration of use was 2 months which is significantly shorter than clinical guideline recommendations.
Results in the Context of Published Literature
With approximately half of cervical cancer patients diagnosed and treated before menopause,2 3 most will experience premature menopause secondary to treatment that may include bilateral salpingo-oophorectomy, radiotherapy, chemotherapy, or some combination. Data have shown that patients with cancer who have experienced treatment-related menopause tend to have more troublesome and severe vasomotor symptoms than women who experience natural menopause.17 18 This is likely due to the abrupt deprivation of hormones caused by treatment compared with a more gradual decline of hormone levels which occurs during natural menopause. Moreover, cervical cancer patients, many of whom receive pelvic radiation, often experience symptoms related to sexual dysfunction such as vaginal dryness and dyspareunia,19 which may be partly improved by HRT.19 In addition to menopausal symptoms, iatrogenic premature menopause may also impact long-term outcomes, such as cardiovascular disease, osteoporosis, and all-cause mortality. Given the high rates of cure and favorable prognosis among early-stage cervical cancer patients, HRT in pre-menopausal women can confer important long-term overall health benefits. Prior work has suggested that fewer than half of cervical cancer patients who were pre-menopausal received HRT,10–12 which was consistent with our study.
Underuse of HRT is likely multifactorial. It is likely that there is concern among patients and providers about adverse oncologic outcomes, including risk of recurrence, if taking HRT. Given that cervical cancer is not thought to be hormonally mediated, unlike endometrial and ovarian cancers, the risk of cancer progression or recurrence related to exogenous estrogen exposure should be negligible.4 10 20 21 Supporting this, one randomized controlled trial from 1987 suggested that HRT did not affect oncologic outcomes among cervical cancer patients.22 However, there is a lack of high-quality prospective studies examining the association between HRT and oncologic outcomes in cervical cancer patients, which may have contributed to the limited clinical guidance on how to prescribe and manage HRT use among patients diagnosed with cervical cancer.10 11 While multiple organizations, including the American College of Obstetricians and Gynecologists, the North American Menopause Society, the European Society of Human Reproduction and Embryology, the European Menopause and Andropause Society, and the International Gynecologic Cancer Society, support the use of HRT among cervical cancer patients, stating minimal safety concerns and potentially significant benefits,13 23–25 contemporaneous prospective studies on the effectiveness and safety of HRT use among cervical cancer patients to support these statements and guidelines are largely lacking.
In our study, we excluded patients who underwent ovarian transposition as endogenous estrogen production would be preserved, affecting their need for HRT. However, the proportion of ovarian transposition before primary pelvic radiotherapy was very low in this study, which is consistent with what we reported in a prior study where 8.2% of cervical cancer patients underwent ovarian transposition before radiotherapy.26 Despite patients who received ovarian transposition accounting for a small subset of cervical cancer patients, this group may warrant future investigation regarding the role and timing of HRT after the procedure.
Strengths and Weaknesses
Our study benefits from the inclusion of a large sample of patients from across the USA. Further, all patients within the cohort had comprehensive prescription drug coverage. Our study had several limitations. First, given the unspecific billing codes for oophorectomy concurrent with hysterectomy, the performance of oophorectomy could not be determined in a sizeable number of patients. We intentionally restricted our study cohort to patients for whom we were certain about performance of bilateral oophorectomy. Second, we lack data on tumor characteristics as well as clinical conditions such as symptoms of estrogen deprivation that may have influenced the use of HRT. Third, due to a relatively small cohort and the switch of health insurance plan, the maximum follow-up time period for each patient was limited to 24 months after primary treatment. While we did not analyze use of HRT beyond 24 months, we expect that most patients who initiated hormonal therapy would have done so within 2 years of treatment. Lastly, we cannot exclude the possibility of selection bias in creation of the cohort.
Implications for Practice and Future Research
HRT is under-utilized among pre-menopausal cervical cancer patients, despite clinical guidance supporting its short- and long-term health benefits as well as safety. Among cervical cancer patients under age 50 who have experienced premature menopause, HRT should be routinely discussed. Further investigation is needed to understand the reasons for HRT under-utilization among both patients and providers.
Conclusion
HRT was prescribed to less than 40% of patients with newly diagnosed cervical cancer under age 50 who experienced premature menopause due to primary treatment. Among those who used HRT the duration of use was short.
Data availability statement
No data are available. Embargo on data due to commercial restrictions.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
YS and YH contributed equally.
Contributors All authors have made substantial contributions to the conception, design, acquisition, analysis, or interpretation of data for the manuscript. Conception and design: YS, YH, JSF, AK, DLH, JDW. Methodology: YS, YH, JDW. Data acquisition and analysis: YS, YH, JDW. Data interpretation: YS, YH, JSF, AK, DLH, JDW. Manuscript writing: YS, YH, AK, JDW. Reviewing and editing: all authors. Final approval of manuscript: all authors. Guarantor: JDW.
Funding YS received the 2021 JMWH Bayer Grant conferred by the Japan Society for Menopause and Women’s Health.
Competing interests JDW has received royalties from UpToDate and received research funding from Merck.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.