Article Text

Statistics from Altmetric.com
Case presentation
A 65-year-old woman, gravida 1, parity 0 (G1P0100) presented to her doctor with post-menopausal bleeding for 3 months. A pelvic ultrasound revealed a thickened endometrial stripe of 1.5 cm. Her past medical history was significant for obesity with a body mass index of 40 kg/m2. She denied having any prior surgeries. Her family history was unremarkable. On physical examination she was noted to have a normal appearing cervix and a mobile uterus without palpable adnexal masses; however, the exam was limited by her habitus. An endometrial biopsy was performed and revealed an International Federation of Gynecology and Obstetrics (FIGO) grade 1 endometrioid adenocarcinoma and she was referred to gynecology oncology. Unfortunately there was a >6 month delay between referral and oncologic evaluation, for social reasons.
Dr Rauh-Hain
What would be your approach to counseling a patient with this diagnosis?
Endometrial cancer most frequently presents in post-menopausal women with the incidence peaking between the age of 60 and 70 years. Generally speaking, the malignancy produces abnormal uterine bleeding symptoms that prompt an evaluation that ultimately leads to a diagnosis before it becomes an advanced stage. In fact, the majority of cases (60–70%) are diagnosed at an early stage and over 90% of cases are considered type 1 neoplasms, which have a low-grade endometrioid histology and comprise the majority of endometrial cancers.1 Reassuring elements of this patient’s pathologic diagnosis include that it is a well-differentiated (grade 1) malignancy with endometrioid histology.
Dr Tandon
The endometrial biopsy was composed of superficial fragments of endometrial endometrioid adenocarcinoma, FIGO grade 1 (Figure 1A and B). Immunohistochemical staining demonstrated retained expression of MMR (mismatch repair) proteins (microsatellite stable).

Hematoxylin and eosin stain of endometrial biopsy at diagnosis at 4× (A) and 10× (B) magnification.
Dr Rauh-Hain
Did you pursue any additional pre-operative work-up in this case?
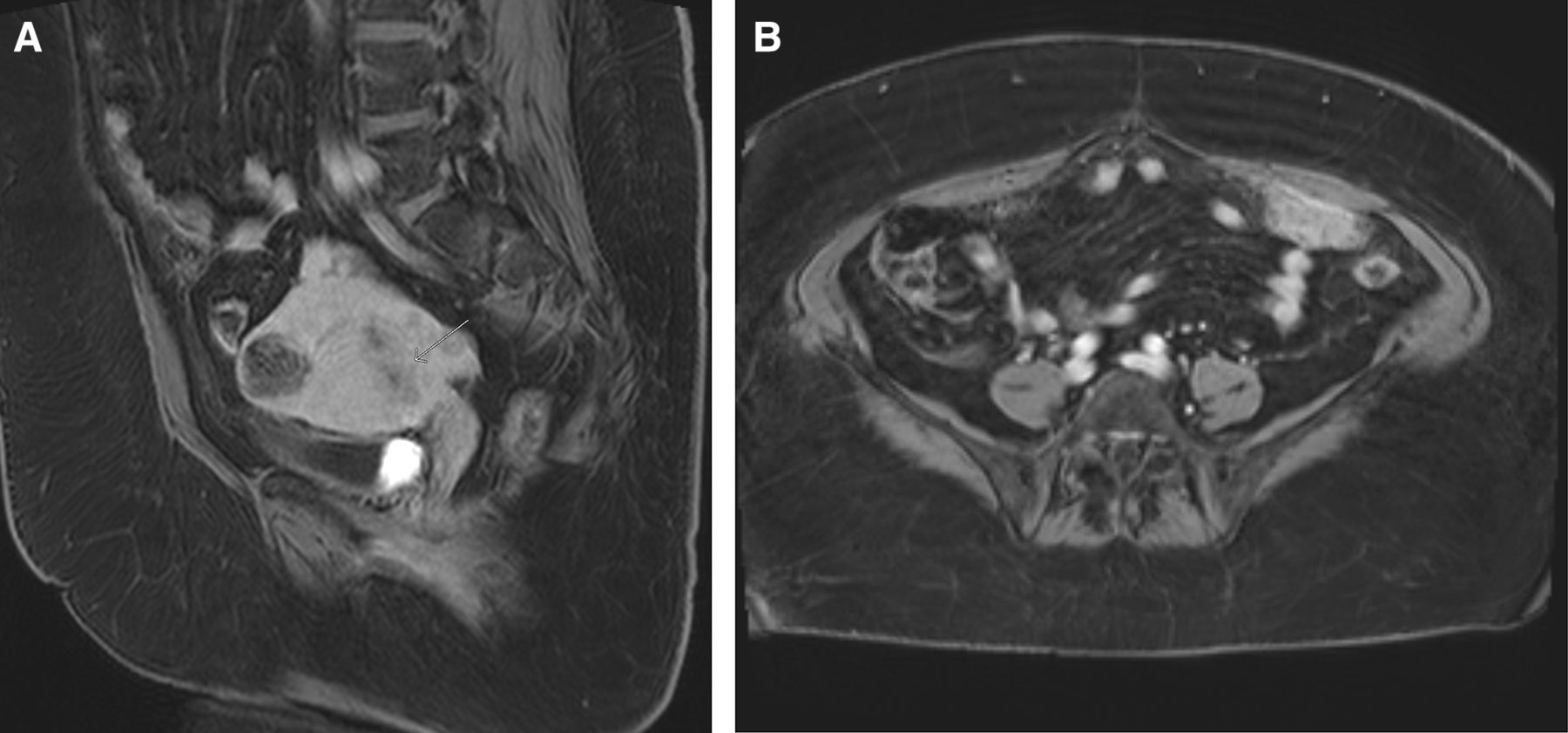
Classically, endometrial cancer is surgically staged but pre-operative imaging with either transvaginal ultrasound or magnetic resonance imaging (MRI) are important tools to assess the degree of myometrial invasion, the presence of cervical stromal involvement, and also can identify possible distant spread.2 Computed tomography can also be utilized; however, it is less valuable for interpreting myometrial invasion compared with MRI.3 In this case, given the delay between initial sampling and the patient’s clinical evaluation, an MRI of the pelvis was obtained to assist in management planning and to rule out more advanced stage disease. The patient was counseled that provided she had early-stage disease, the standard of care management would be surgical. Survival outcomes in this setting are >95% at 5 years and cure is achievable in early grade, early-stage disease.1 In her case, the MRI was notable for a hypoenhancing lesion in the endometrium consistent with the biopsied endometrial cancer, but also raised concern for widely metastatic disease given findings consistent with peritoneal carcinomatosis (Figure 2). Additionally, an enhancement was noted in the liver, which was also concerning for metastasis.

MRI of the pelvis demonstrating (A) a multi-fibroid uterus with hypoenhancing tumor lesion in the endometrial cavity (white arrow) and (B) enhancing carcinomatosis with omental caking.
Dr Rauh-Hain
What would be your discussion with the patient at this time with the imaging findings raising concern for metastatic disease?
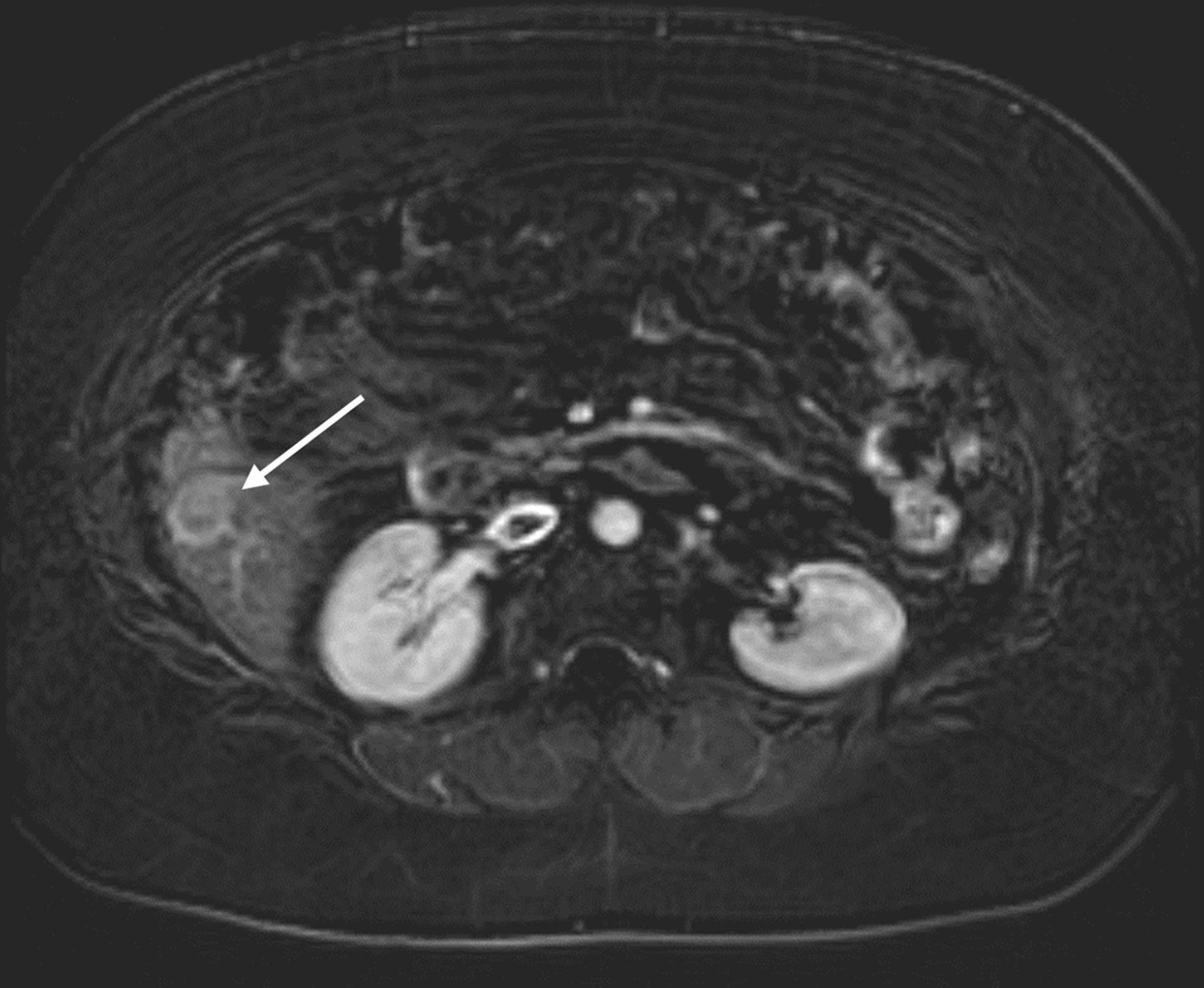
Although endometrial cancer is often diagnosed at an early stage, these imaging findings were concerning for widespread metastatic disease. While it is atypical for low grade histology such as the patient’s to widely metastasize in such fashion, the presence or absence of metastatic disease would alter her treatment strategy. If the imaging findings were to indeed represent widely metastatic disease that was not amenable to surgical resection, one treatment approach would be neoadjuvant chemotherapy with a platinum-based regimen prior to attempting complete surgical resection.4–7 However, if the liver lesion was deemed more likely to be a benign entity, the treatment approach would be surgical with a total hysterectomy and bilateral salpingo-oophorectomy with lymph node staging. Lymph node staging would be omitted if there was evidence of carcinomatosis or extra-uterine spread as this would up-stage the patient, rendering lymph node dissection irrelevant. Therefore, at this juncture I would counsel that it is reasonable to obtain additional focused imaging of the liver as well as a liver biopsy to more definitively ascertain whether the liver mass represented a malignant versus benign process, as this would significantly impact the treatment approach. A dedicated MRI of the liver was therefore subsequently obtained and demonstrated an enhancing hepatic lesion measuring up to 2 cm (Figure 3).
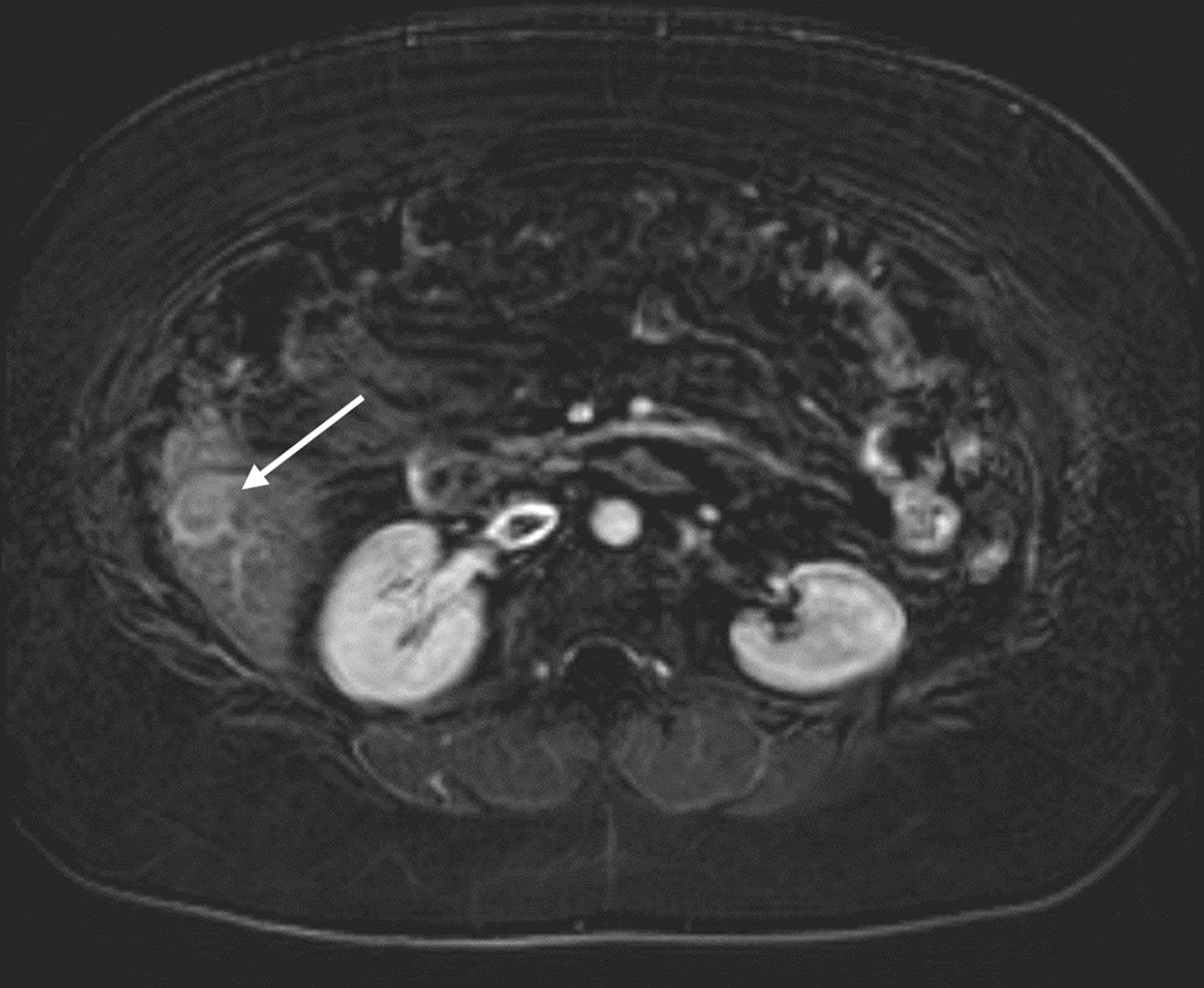
Axial post-contrast MRI with enhancing observations in the right hepatic lobe (segment 6, white arrow) measuring approximately 2 cm concerning for metastasis.
Dr Tandon
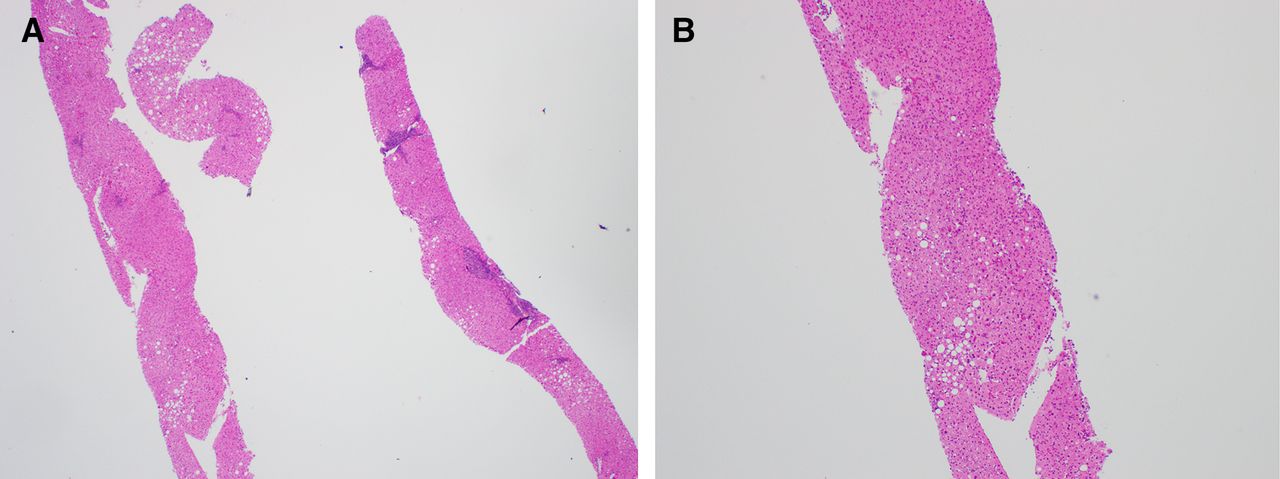
The patient underwent biopsy of the segment 6 liver lesion, which showed benign hepatic parenchyma (Figure 4A and B). No evidence of malignancy was identified.

Liver biopsy (A) and (B) showing benign hepatocytes.
Dr Rauh-Hain
Based on the pathologic findings of the liver biopsy, what would be your recommendations for this patient?
The biopsy findings are reassuring that the lesion does not represent a metastatic disease. While this was encouraging, we know that only 10–25% of the endometrial cavity is sampled with an endometrial biopsy and that a high-grade malignancy could potentially be identified on resampling.1 Therefore, the patient was counseled on the risks/benefits of proceeding with definitive surgical management versus re-sampling the endometrium, and she elected to proceed with definitive surgery with a total hysterectomy, bilateral salpingo-oophorectomy with sentinel lymph node mapping, and tumor debulking.
What were your surgical considerations and what were the intra-operative findings?
Given the discrepancy between the patient’s uterine pathology and pre-operative imaging, there was consideration of performing a diagnostic laparoscopy with intra-operative frozen specimens of any areas of demonstrated disease to determine the presence or absence of widely metastatic disease. If this were to be identified, an assessment of feasibility of laparoscopic staging and tumor reductive surgery could be performed. And, while the GOG-LAP2 trial demonstrated that laparoscopic surgical staging with clinical stage I to IIA uterine cancer is feasible and safe, the standard of care for more advanced endometrial cancer is less clear cut.8 In fact, according to the National Comprehensive Cancer Network, both open and minimally invasive surgery are acceptable treatment approaches for advanced endometrial cancer.4 Given the enlarged multi-fibroid uterus and the potential for metastatic disease seen on pre-operative imaging, an open approach was selected in this case. On entering the abdomen, peritoneal carcinomatosis was noted with disease involving the uterus, omentum, and bilateral hemidiaphragms along with numerous small (2–3 mm) nodules over the bowel mesentery, but without disease over the bowel serosa. There were also several small nodules on the liver in addition to a larger, approximately 2 cm lesion, that had been biopsied pre-operatively. An optimal cytoreductive surgery was ultimately performed and included a total abdominal hysterectomy, bilateral salipingo-oophorectomy, supra-colic omentectomy, and argon beam coagulation of implants to the liver, mesentery, and diaphragm.
Dr Tandon
What was the final pathologic diagnosis in this case?
On gross examination, the omentum showed multiple tan-white nodules, with the largest nodule measuring 7 cm in greatest dimension. The uterus showed an endometrial tumor measuring 4.5 cm. No myometrial invasion was identified grossly. One of the fallopian tubes showed a hemorrhagic cyst measuring 4.5 cm, while the contralateral fallopian tube and bilateral ovaries were grossly unremarkable. Histological examination demonstrated a synchronous malignancy with a stage IIIC peritoneal high grade Mullerian carcinoma and a stage IA FIGO grade 2 endometrial endometrioid adenocarcinoma.
The high grade Mullerian carcinoma was composed of mixed serous and endometrioid carcinoma (Figure 5A, B and C). Immunohistochemical stains showed that the tumor was diffusely and strongly positive for p53 (Figure 5D) and p16 with focal positive staining for estrogen receptor and progesterone receptor. The serous component of the tumor showed focal positive staining for WT1, while the endometrioid component was negative for WT1. The high grade Mullerian carcinoma involved the uterine serosa, and one fallopian tube and ovary. The liver nodule showed minute foci of extensively crushed atypical cells (Figure 5E). The atypical cells were positive for pancytokeratin. They showed diffuse, strong staining for p53 and weak staining with estrogen receptor consistent with metastatic high grade Mullerian carcinoma.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Hematoxylin and eosin stains and immunohistochemistry of uterine and ovarian malignancy. (A) Omentum showing high grade Mullerian carcinoma with mixed serous and endometrioid carcinoma. (B) Serous carcinoma component of high-grade Mullerian carcinoma with marked nuclear atypia. (C) Endometrioid carcinoma component of high-grade Mullerian carcinoma. (D) P53 showing diffuse, strong staining. (E) Liver nodule with crushed atypical cells (thick arrow) and benign hepatocytes (thin arrow). (F) Endometrial tumor with no myometrial invasion.
The endometrial tumor was submitted entirely for histological examination and showed a grade 2 endometrioid adenocarcinoma (Figure 5F). No serous carcinoma or other high-grade component was identified. Immunohistochemical stain, p53, showed wild-type staining pattern. The tumor involved the lower uterine segment; however, no myometrial or lymphovascular space invasion was identified. The tumor in the omentum was morphologically and immunohistochemically distinct from the endometrial tumor, precluding a metastasis from endometrium.
Dr Rauh-Hain
What would be your discussion with the patient regarding adjuvant treatment strategies?
The rate of synchronous uterine and ovarian cancers is approximately 10% for patients with ovarian cancer and 5% for patients with endometrial cancer, respectively.9 10 The need for adjuvant therapy for an early-stage endometrial cancer is dependent on uterine factors such as depth of invasion, lymphovascular space invasion, and histologic subtype.4 In this case, the patient’s endometrial cancer would not warrant adjuvant therapy. However, her concurrent stage IIIC ovarian cancer certainly merited adjuvant treatment.8 9 11 Because endometrioid histology is the most common histologic subtype in both sites of synchronous ovarian and uterine cancers, differentiation between three clinical situations is important: primary endometrial cancer with metastases to ovaries, primary ovarian cancer with metastases to endometrium, or two synchronous primary cancers. Interestingly, the survival outcomes for synchronous malignancies are somewhat paradoxical in that those patients with low-stage synchronous primary ovarian and endometrial cancers have favorable survival outcomes compared with patients with single ovarian cancers. However, in this case, the patient was diagnosed with an advanced stage ovarian cancer and her survival outcome would be expected to mirror patients without a synchronous diagnosis, and her treatment strategy will be focused on her advanced staged ovarian malignancy.4 10
Closing summary
Synchronous cancers of the ovary and endometrium are rare, representing just 3% of all epithelial ovarian cancer cases.9 Identification and distinction of this diagnosis has important clinical implications for treatment strategies as well as prognostic differences. In patients with low grade uterine cancer who demonstrate imaging findings of advanced stage disease it is important to remain vigilant and consider a synchronous primary ovarian malignancy. In these cases where pre-operative imaging and histologic diagnosis are discordant, a repeat endometrial biopsy could provide additional evidence of a higher-grade endometrial lesion missed on initial sampling or help lead to further consideration of a synchronous primary ovarian malignancy. In this case, where the pre-operative imaging findings were concerning for metastatic disease, one could consider a diagnostic laparoscopy with frozen section of the omentum or other areas amenable for biopsy, to allow for a more objective assessment of the diagnosis to further guide the treatment planning and determine the feasibility of optimal cytoreductive surgery. It is well known that optimal cytoreductive surgery (resected to <1 cm gross residual disease) in ovarian cancer is associated with improved survival6; and, while the data are more limited in endometrial cancer, these findings are often extrapolated from ovarian cancer.9 10 Therefore, determination of whether a case represents an advanced stage uterine versus ovarian malignancy can ultimately guide the provider in selecting the appropriate course for either neoadjuvant treatment followed by surgery or for adjuvant therapy after surgical cytoreduction.
Often, as in this case, the path to treatment recommendations in synchronous ovarian and uterine cancers ultimately depends on the final pathologic diagnosis and does not necessarily proceed in a straightforward fashion. Here, we demonstrate a case for reconsideration of the diagnosis when pre-operative imaging findings of metastatic disease are not in keeping with an initial pathologic diagnosis of low-grade endometrial carcinoma. These sorts of scenarios highlight the importance of thorough discussions, careful consent processes, and shared decision-making with patients when moving forward with treatment recommendations.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Footnotes
Contributors DMG is the presenter, NT is the pathologist, NF is the radiologist, and RJH is the discussant.
Funding The research reported here is supported in part by the T32 training grant (CA101642) for DMG.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.