Article Text

Abstract
Introduction/Background Recently, ESGO/ISUOG/IOTA/ESGE Consensus Statement on pre-operative diagnosis of ovarian tumors implied that neither Human epididymis protein 4 (HE4) nor Risk of Ovarian Malignancy Algorithm (ROMA) improve the discrimination between benign and malignant masses compared with CA 125 alone. This statement may be reassessed if a novel algorithm, more powerful than ROMA, will be developed. Thereby the aim of this study was to elaborate a new predictive algorithm, based on serum CA125&HE4, which performs better than ROMA
Comparison of the performance of ROCK-I and ROMA

{kind=link}
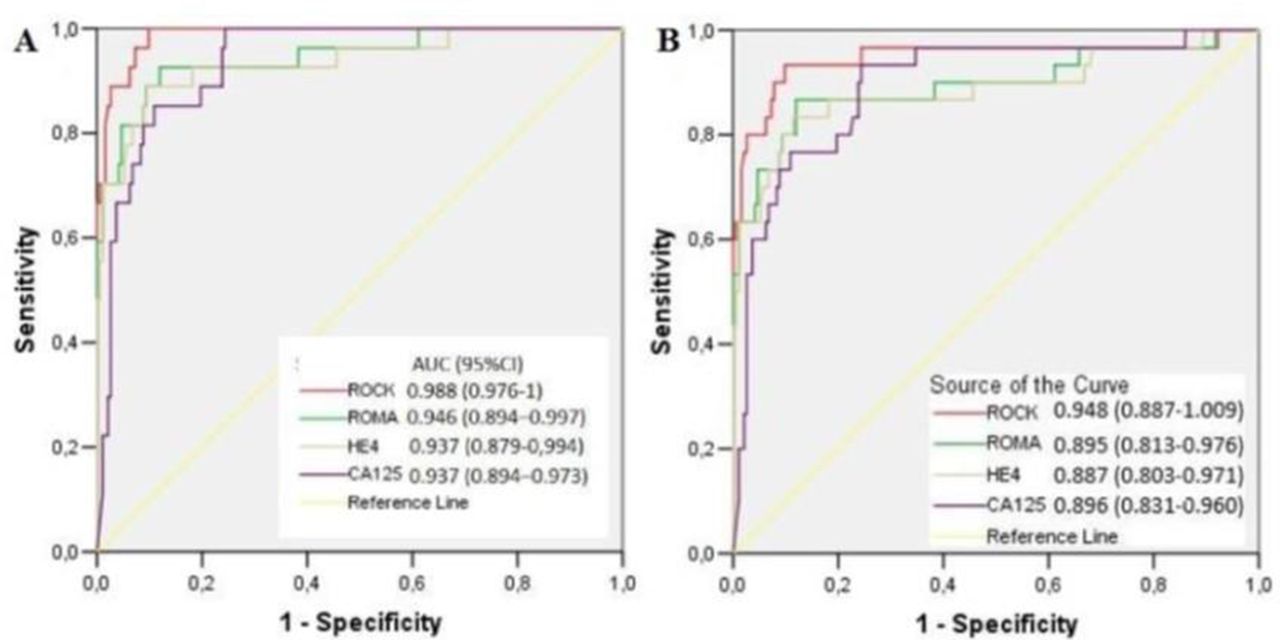
ROC-curves for ROCK-index, ROMA, CA125 and HE4 in the validating dataset. A) ‘bening’ vs ‘all stages of EOC & stages Ic2-III of BOT’; B) ‘bening’ vs ‘all malignant diseases & stages Ic2-III of BOT’. EOC – epithelial ovarian cancer; BOT – borderline ovarian tumors
Methodology A novel algorithm, based on serum HE4, CA125 and patient’s age as variables, has been developed using a training dataset. This algorithm was named Risk of Ovarian Cancer Kazan Index (ROCK-I). The validating group consisted of 227 consecutively operated premenopausal patients with pelvic mass out of which there were 193 cases of benign diseases, 27 cancers and 7 borderline ovarian tumors (BOT).
Results ROCK-I demonstrated two fold less false positive results than ROMA. Thus, in the validating dataset, there was a statistically significant superiority of ROCK-I over ROMA in the specificity (92.2% and 84.5% respectively, p=0.017). Meanwhile, the sensitivity of ROCK-I was also numerically higher in all the scenarios of discrimination (table 1). When the scenario of discrimination ‘benign disease vs the joint group of EOC (all stages) together with BOT stage Ic2-III’ was used, ROC-AUC of ROCK-I, ROMA and CA 125 were 0.988, 0.946 and 0.937 respectively (figure 1). The difference in ROC-AUC between ROCK-I and CA125 was statistically significant (p=0.01) while the difference between ROMA and CA125 was not (p=0.79).
Conclusion ROMA provides a suboptimal prediction, at least, in premenopausal patients. If a large independent validation shows similar or even slightly lower superiority of the novel ROCK-I over ROMA, it may provide a new basis of routine-use of HE4 in the preoperative assessment of premenopausal patients with pelvic mass.