Article Text

Abstract
Introduction/Background Past management of cervical intra-epithelial neoplasia-2 (CIN-2) has centred around treatment via excision. Contemporaneously, more onus has been placed on conservative management of this disease in women of reproductive age. This is namely to prevent future preterm birth.
Methodology A retrospective analysis was completed of patients undergoing conservative management of biopsy confirmed CIN-2 between 2017–2021 in a single tertiary centre. This included 6 monthly colposcopic assessment for a total 24 months with either smear or biopsy alternatively. Excision was offered in the event of progression or patient choice. Primary outcome was divided into successful regression and discharge back to routine monitoring, progression or persistence requiring intervention, and patient adherence (drop-out or loss to follow-up). Further secondary measures were also examined, including pregnancy outcomes, and a sub-group analysis of smokers and those aged over 35 years old. Statistical analysis was completed using R Studio Ver 1.2.5033.
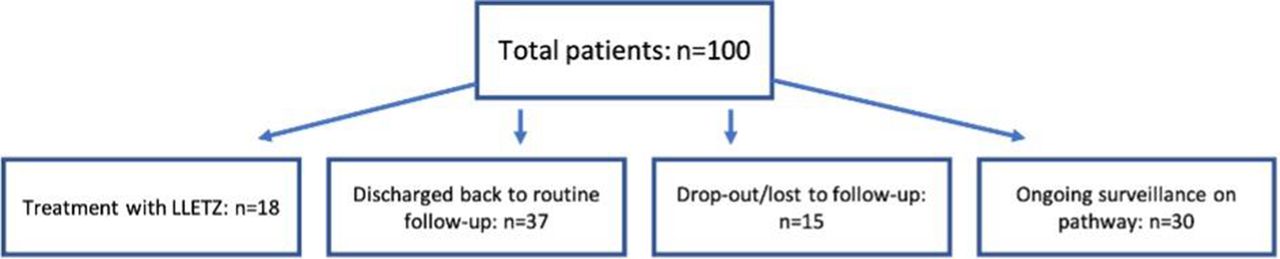
Results A total of 100 patients underwent conservative management. Primary outcomes are summarised in figure 1. A total of 18 women were treated with LLETZ, including 6 for patient choice. No women had progression of disease to malignancy, and 5 progressed to CIN-3. The average time to dropout was 12.42 months (1–22). Smokers and those over 35 were not significantly more likely to require intervention then the rest of the population (p=1.0000 and p=0.5936 respectively). 15 women became pregnant either during or after management. A total of 12 live births occurred, and 3 losses between 6–12 weeks gestation. A single preterm delivery occurred due to other reasons.

{kind=link}
Conclusion • Conservative management represents a safe management to those of reproductive age.
• Therefore, critical reductions in preterm birth and pregnancy loss are possible.
• Patient drop-out is a concern. Further data should focus on patient selection for wider intervals to improve adherence rates.