Article Text

Abstract
Introduction/Background A large body of research has validated several quality indicators of end-of-life (EOL) cancer care, but few have examined these in gynecologic cancer. Early palliative care (PC) is associated with improved patient quality of life, less aggressive EOL care, and prolonged survival. We examined provincial palliative and EOL care patterns.
Methodology This population-based, retrospective cohort study of gynecologic cancer decedents in Ontario from 2006–2018 used linked administrative health care databases. Quality indices included: emergency department (ED) use, hospital or intensive care unit (ICU) admissions, chemotherapy ≤14d of death, PC home visits, and death in hospital. Multivariable logistic regression examined factors associated with aggressive and supportive care.
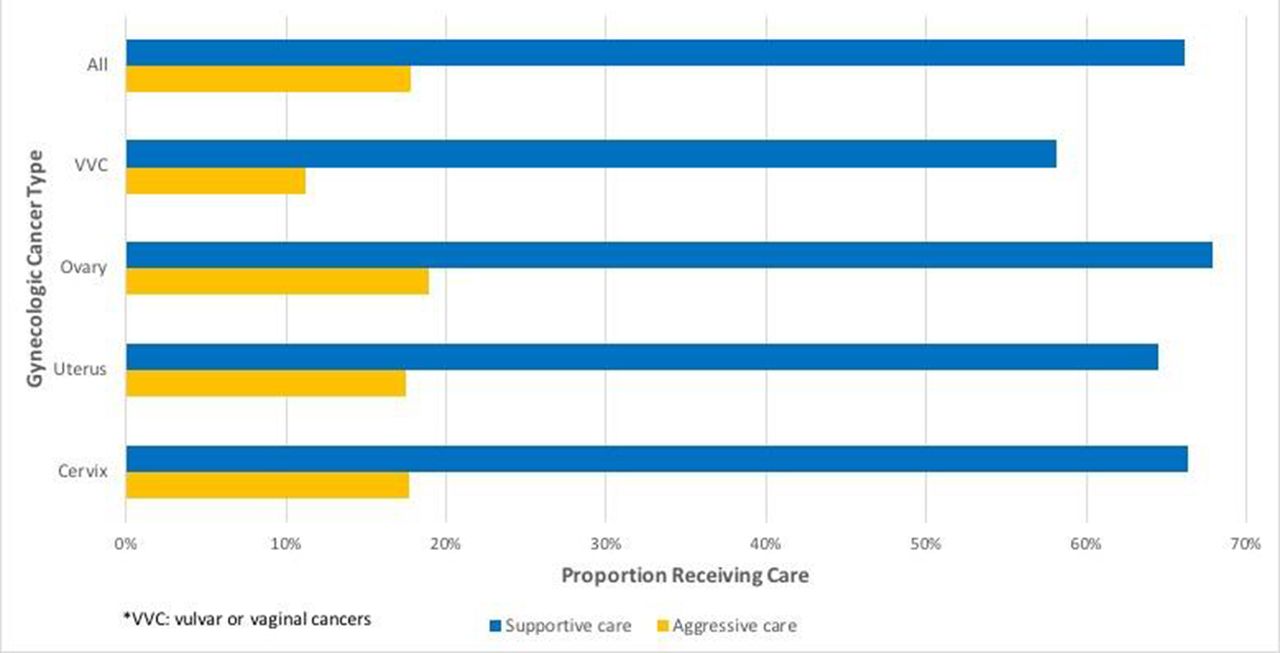
Results There were 16,237 included decedents. Hospital death rates decreased from 47% to 37%, supportive care use rose from 65% to 74%, and aggressive care remained stable (16%). Within 30d of death, 50% were hospitalized, 5% admitted to ICU, and 67% accessed palliative homecare. Within 14d of death, 31% visited the ED and 4% received chemotherapy. Vulvovaginal cancer patients accessed the least resources. Factors associated with aggressive EOL care included younger age, shorter survival, lower income, and rurality. Palliative care was accessed by 93.4% of decedents a median 127d before death, with first contact as outpatients for 68.8% and institutionally for 31.2%. Those accessing PC used median 8 institutional days and 41 community days. While use of community PC gradually increased toward end-of-life, use of institutional PC exponentially increased from 12 weeks until death.
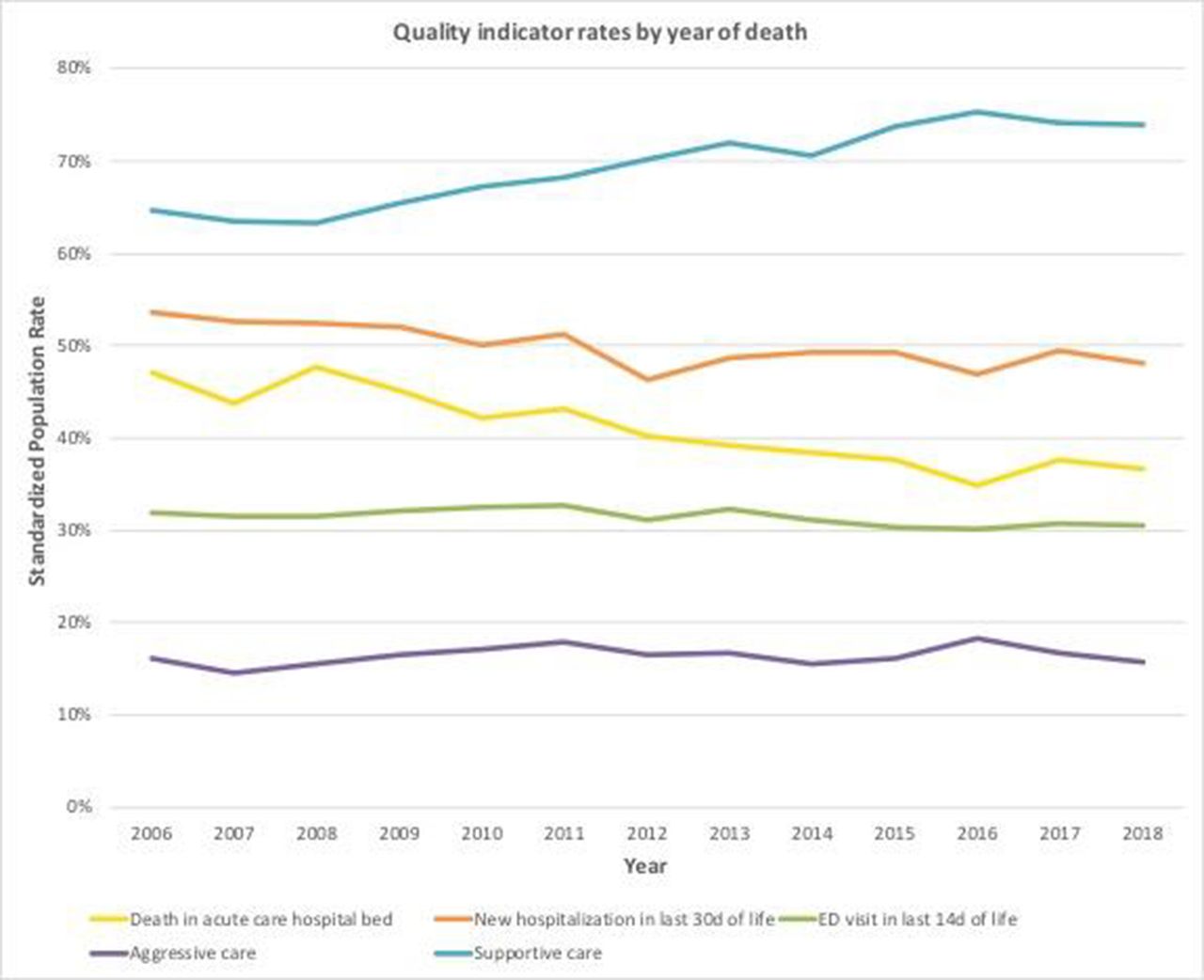
Rates of supportive and aggressive end-of-life care received by patients with gynaecologic cancers in Ontario Canada from 2005–2018

{kind=link}
{kind=link}
Conclusion Over time, fewer women dying with gynecologic cancers in Ontario experienced death in hospital, and more accessed supportive care. However, most were hospitalized and a significant proportion received aggressive care. While >90% of gynecologic cancer decedents accessed PC, median initiation was within the last 4 months of life (late PC), which may result in suboptimal care quality.