Article Text

Abstract
Introduction/Background Over the last twenty years, data from more than 2000 patients from thirty studies on sentinel lymph node (SLN) mapping in early-stage cervical cancer were published. Many of these reports come from small single-centre studies or retrospective data from the time when detection rates were much lower. We present final results on SLN mapping from the Sentix study, the largest prospective cohort study of more than 700 patients.
Methodology Eligible were patients with cervical cancer stages T1a1 L1 – T1b2 (<4 or ≤2 cm for fertility sparing), common tumour types and no suspicious lymph nodes on preoperative imaging. All detection techniques (blue dye, radiocolloid, indocyanine green) and combinations were allowed. Preoperative lymphoscintigraphy was not required and not used. All approaches, laparotomy, laparoscopy, or robotic surgery were acceptable. Intraoperatively pelvic (external iliac, interiliac, common iliac, presacral) and low paraaortic regions were examined for the presence of SLN. All patients with successful bilateral SLN detection and a completed postoperative data continued in the study.
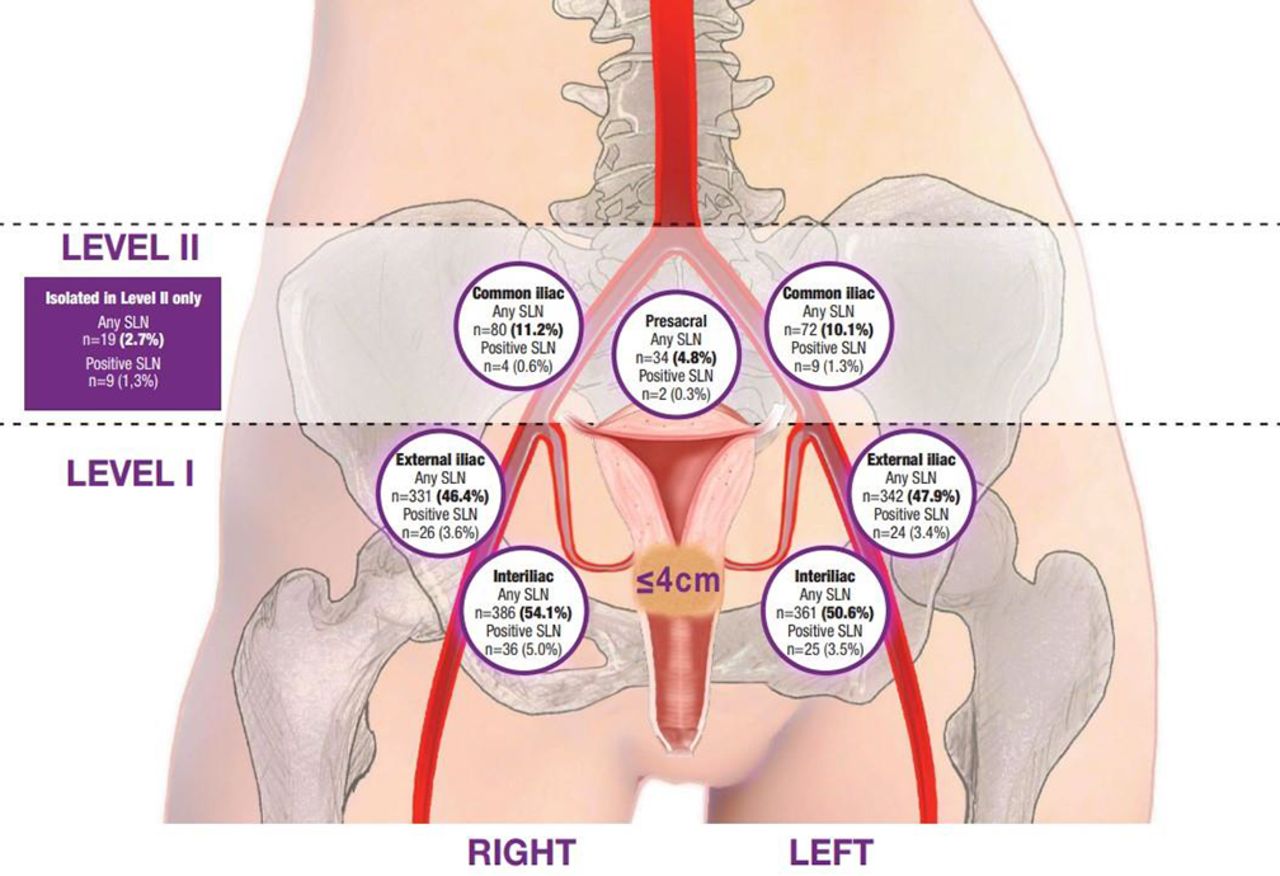
Results Final cohort of 714 patients were analysed, enrolled between 2016–2020 in 47 centres and 18 participating countries. Bilateral SLN detection rate reached 92.3% with the median of 3 SLNs per patient. All SLNs were detected in the pelvis, no SLN in the low paraaortic region. The majority (97.3%) were localized in the pelvic level I, below the interiliac bifurcation. There was an extremely low rate (1.3%) of isolated positive SLNs in pelvic level II. No laterally distinct distribution of SLNs was found.
{kind=link}
Conclusion During SLN biopsy, surgical pelvic dissection should focus on the bilateral anatomical area below the interilical bifurcation, the external iliac vessels region, and the obturator fossa, where SLNs are most frequently located. Occurrences outside this region are rare with an extremely low risk of isolated metastatic SLN in the pelvic level II.