Article Text

Abstract
Introduction/Background Radical vaginal trachelectomy (RVT) is an alternative curative-intended fertility preserving procedure for women with a fertility desire and cervical cancer FIGO 2009 stage IA2 and IB1 with a tumor size ≤ 2 cm. In Denmark RVT was introduced and centralised to Rigshospitalet in 2003, and data from all patients undergoing trachelectomy has been prospectively reported to The Danish Gynaecological Cancer Database (DGCD). In 2014, the procedure advanced to a robotic-assisted approach (RRT). In this study, we present the largest single-center cohort to date of patients undergoing RRT versus RVT, evaluating surgical radicality, length of recurrence-free survival and cancer-specific mortality.
Methodology This is a retrospective cohort study of patients undergoing RVT and RRT from 2003 to 2021. Clinical and pathological data was extracted from DGCD and validated through electronic medical journals. All analyses were performed with SPSS.
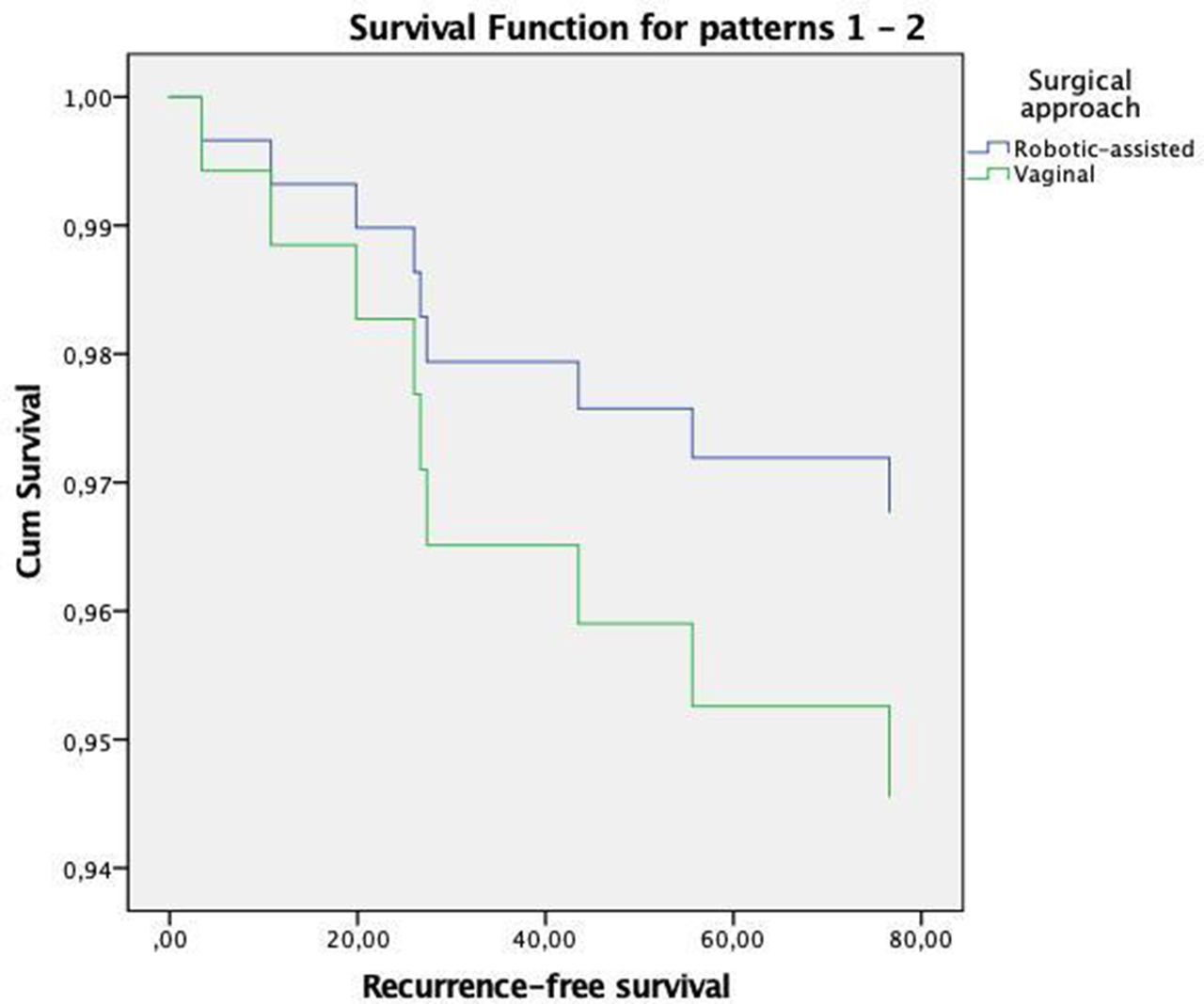
Results A total of 206 patients were included, of which 78 underwent RRT and 128 underwent RVT. There were no significant differences in age, smoking status, ASA score, FIGO 2009 stage, histology, invasion or tumor size. Median BMI in the VRT and RRT group was 23.0 (range 17.7–48.7) and 24.3 (range 18.0–48.4), respectively (p=0.032). The rate of microscopic free-margins in the VRT and RRT group was 99.2% and 97.4%, respectively (p=0.558), The rate of lymph node metastases was 2.3% and 1.3%, respectively (p=1.000), and the rate of surgical radicality was 96.0% and 96.2%, respectively (p=1.000). Hazard ratio for recurrence in the RRT group was 0.59 (CI95% 0.12–2.86, p=0.509), 0.77 (0.14–4.15, p=0.763) when adjusting for BMI, FIGO 2009 and LVSI, and 0.84 (0.16–4.50, p=834) when additionally excluding patients with lymph node metastasis at surgery (n=4). The rate of cancer-specific mortality in the VRT and the RRT was 2.3% (n=3) and 2.5% (n=2), respectively.
{kind=link}
Conclusion RRT seems oncologically safe for radical trachelectomy compared with RVT.