Article Text

Abstract
Introduction/Background Sentinel lymph node (SLN) technique identifies the first node(s) draining any organ and uses ultra-staging to detect micro-metastases. SLND reduces surgical-related morbidity, lymphedema, lymphocyst formation and operative time. It detects nodal metastases at aberrant sites and upstages 18–20% in high-risk patients.
Methodology Women requiring lymphadenectomy in intermediate & high-risk endometrial cancer at Guy’s and St Thomas’ Cancer Centre were included. Data was collected prospectively and results analysed. Intra-cervical IndoCyanine Green (ICG) was injected at two sites and surgery performed using Xi Davinci robot. SLN were mapped using firefly fluorescent camera and sampled. Bilateral pelvic lymphadenectomy (BPLND) was performed following SLN sampling.
{kind=link}
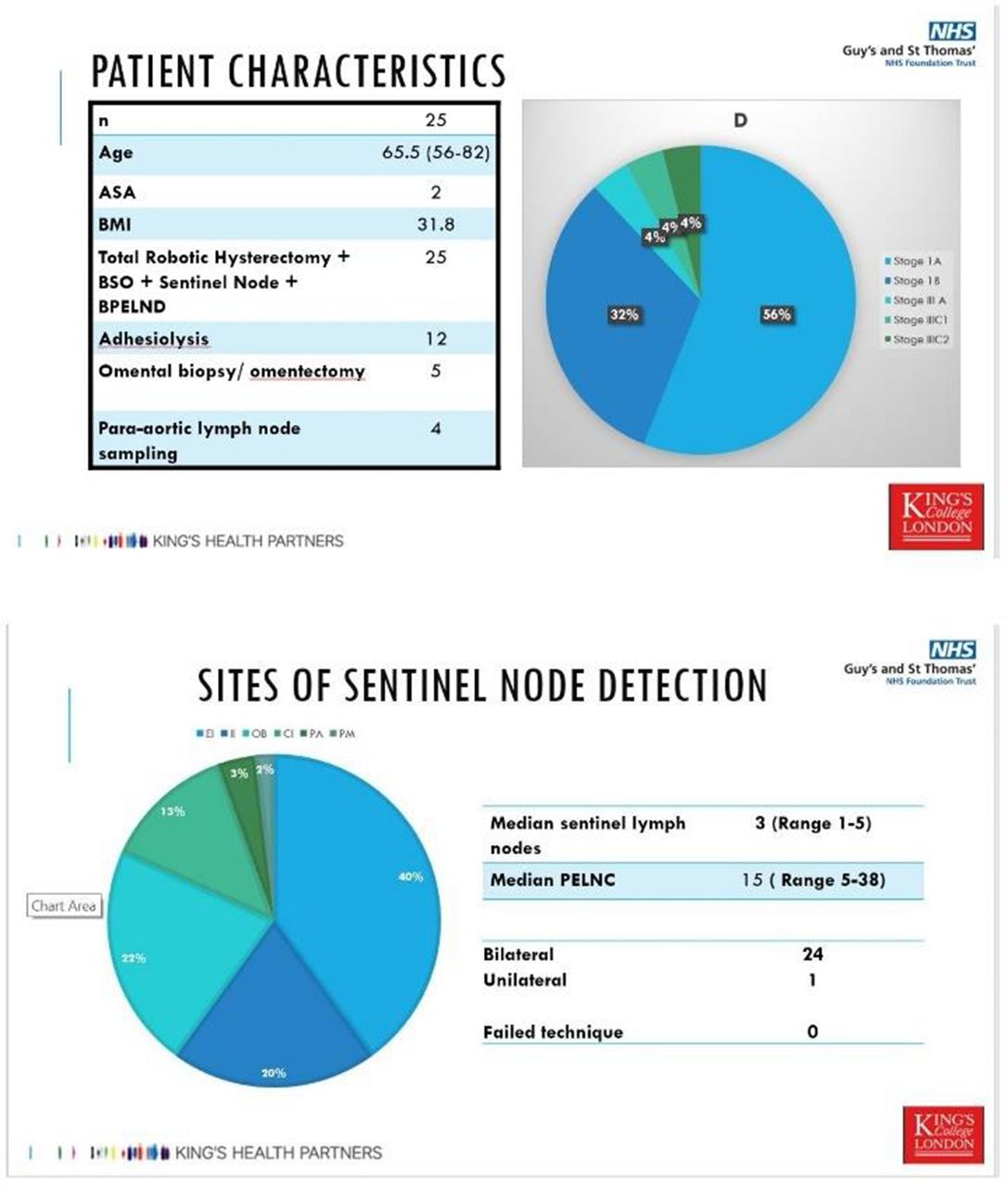
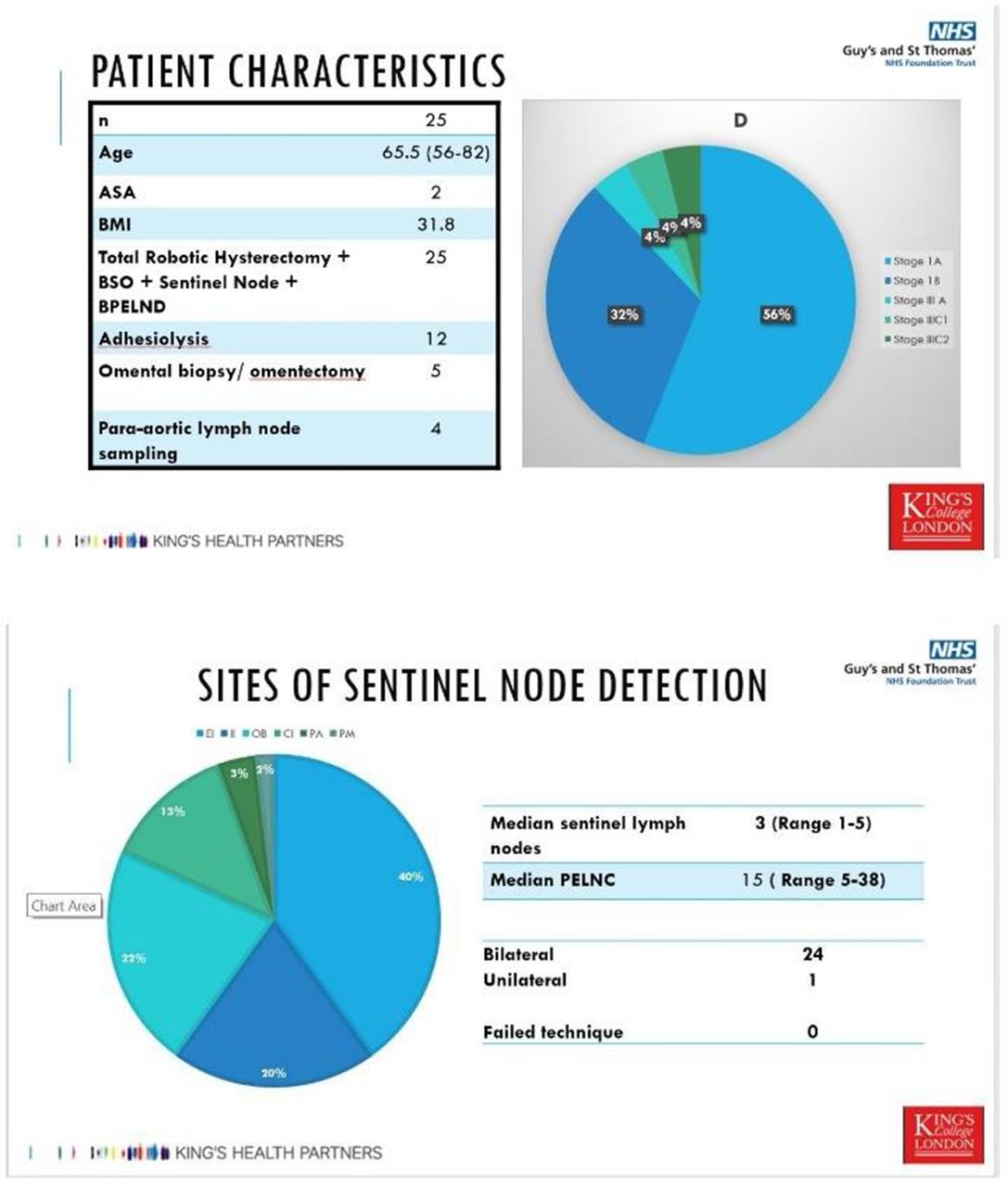
Results 25 patients underwent SLND during robotic staging for intermediate and high-risk endometrial cancer. Mean age was 65.5 years (56–82), ASA score=2 and mean BMI=31.8. Women underwent total hysterectomy and bilateral salpingo-oophorectomy in all, adhesiolysis (48%), omental sampling (20%) and para-aortic sampling (16%). The FIGO stages included stage-I (88%) and Stage-III (12%). Median lymph node count in SLN was 3 (1–5) and BPLND was 15 (5–38). Nodal metastasis was 8%. Para-aortic lymph node positivity was 4%. SLND sensitivity was 100%, specificity 96.15%, false-negative rate 0%, negative predictive value 100%. Median time for SLND was 15 min (10–22) while BPLND was 35 min (25–40). Bilateral SLND was achieved in 96%. Obturator node was the most common SLN site (40%). 8% SLN were detected in paraaortic and parametrial sites. Complication rate was 1.8%.
Conclusion Our pilot study shows that SLND with ICG in intermediate and high-risk endometrial cancer is accurate with high negative predictive values. The quality of nodal assessment was improved by identifying aberrant location in 8% women with SLND. Our series is comparable to international standards and mandates a change in institutional practice. SLND-only is accurate technique for nodal assessment in surgical staging for intermediate and high-risk endometrial cancers.