Article Text

Statistics from Altmetric.com
The loco-regional metastatic or non-metastatic status of related lymph nodes (LN), is critical to managing adjuvant therapy for most cancer patients. This is because the presence or absence of lymphatic metastases is essential for the accurate staging of the disease.1 The introduction of sentinel lymph node (SLN) biopsy was an important evolution in oncologic surgery. In endometrial cancer (EC) staging, SLN is now approved by European and National Comprehensive Cancer Network (NCCN) guidelines, even in high-risk diseases.1 2 However, SLN procedures for EC have several limitations, including reliability, accuracy and potential procedure-related complications. The risk of SLN complications is always present, but is most commonly related to technical issues due to a lack of experience.3 Common mistakes, especially at the early stages of the learning curve, include inadequate injection sites, removal of second/third level nodes, and/or empty nodes.3 4 To overcome these difficulties, a surgical algorithm exists and is published in the NCCN.2 However, adherence to this algorithm may vary and these variations of surgical techniques potentially impact diagnostic accuracy and oncological outcomes.
This video provides a surgical guide for SLN dissection in endometrial cancer and aims to improve surgical practices. For laparoscopic SLN, the most widespread tracer is indocyanine green based near-infrared fluorescence. This video highlights the importance of exposing the hypogastric and obturator spaces to accurately identify the SLN and the neighboring anatomical structures (external vessels, internal iliac artery, ureter, obliterated umbilical artery) which could be injured during dissection. The first important anatomical landmark to identify is the umbilical artery, along which the dissection and detection of the lymphatic channel and SLN occurred. Once removed, the SLN should be extracted in a protected condition.
In conclusion, completed randomized controlled trials have confirmed the role of sentinel node mapping.5 The proposed step-by-step approach could improve adherence to guidelines and thus increase the accurate identification of SLN and avoid possible complications.

{kind=link}
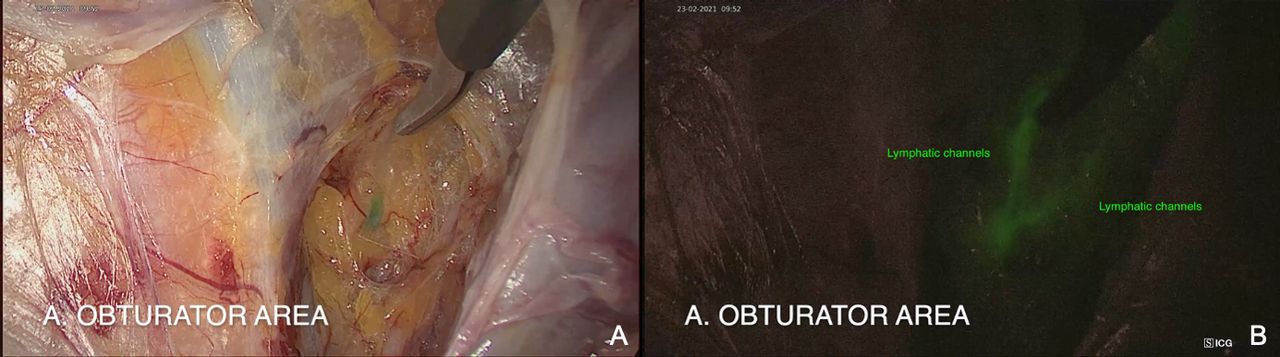
Lymphatics channels in obturator area, real image (A) and ICG image (B). The dissection technique consists of identifying the lymphatic channels in the lateral spaces and avoiding disturbing them in order to accurately target the sentinel lymph node.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Institutional Board: CNIL (Commission Nationale Informatique et Libertés)reference CNIL 2225513 v 0 Participants gave informed consent to participate in the study before taking part.
Footnotes
Contributors Conceptualization: LL, ML. Validation: LL, ML, CM, DQ, CA. Formal analysis: LL, ML, CM. Investigation/Data curation: LL, ML. Original draft: LL. Review: All authors. Visualization: LL, ML, CM. Supervision: BG, CA, DQ. Guarantor: LL.
Funding This study was funded by Plan Investissements d’Avenir” and ANR (ANR-10-IAHU-02).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.