Article Text

Abstract
Objectives The goal of our study was to identify preoperative factors in patients with endometrial intraepithelial neoplasia that are associated with concurrent endometrial cancer to select patients who may benefit from sentinel lymph node (SLN) assessment at the time of hysterectomy.
Methods Retrospective single institution cohort study of patients with a preoperative diagnosis of endometrial intraepithelial neoplasia who underwent hysterectomy with or without staging from January 2010 to July 2020. Modified Poisson regression was used to calculate risk ratios (RR) and 95% confidence intervals (CI).
Results Of 378 patients with a preoperative diagnosis of endometrial intraepithelial neoplasia, 275 (73%) had endometrial intraepithelial neoplasia and 103 (27%) had invasive cancer on final pathology. Age (p=0.003), race (p=0.02), and hypertension (p=0.02) were significantly associated with concurrent endometrial cancer. The median preoperative endometrial stripe was significantly greater in the endometrial cancer group (14 mm (range 10–19)) than in the endometrial intraepithelial neoplasia group (11 mm (range 8–16); p=0.002). A preoperative endometrial stripe ≥20 mm was associated with double the risk of endometrial cancer on final pathology (crude RR 2.0, 95% CI 1.3 to 2.9) and preoperative endometrial stripe ≥15 mm was 2.5 times more likely to be associated with high risk Mayo criteria on final pathology (crude RR 2.5, 95% CI 1.2 to 5.2). Of those with concurrent endometrial cancer, 5% were stage IB, 29% had tumors >2 cm, and 1% had grade 3 histology. Only 3% of all patients underwent lymph node evaluation.
Conclusions In a large cohort of patients with a preoperative diagnosis of endometrial intraepithelial neoplasia, less than a third had invasive cancer and even fewer had pathologic features considered high risk for nodal metastasis, arguing against the use of routine SLN dissection in these patients. Endometrial stripe ≥15 mm may be a useful preoperative marker to identify patients at higher risk for concurrent endometrial cancer and may be an important criterion for use of selective SLN dissection in carefully selected patients with endometrial intraepithelial neoplasia.
- endometrial hyperplasia
- endometrial neoplasms
- lymph nodes
- sentinel lymph node
- SLN and lympadenectomy
Data availability statement
Data are available upon reasonable request. In accordance with the journal’s guidelines, we will provide our data for the reproducibility of this study in other centers if such is requested.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
There are no clear consensus guidelines regarding lymph node assessment in patients with endometrial intraepithelial neoplasia, and even in cases of endometrial cancer the extent of nodal evaluation is debated.
WHAT THIS STUDY ADDS
Patients with preoperative endometrial stripe ≥20 mm were twice as likely to have endometrial cancer on final pathology and those ≥15 mm were 2.5 times more likely to be high risk by the Mayo criteria. These data suggest that there are preoperative factors that may help us to stratify a patient’s risk of concurrent endometrial cancer.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Endometrial stripe may be a useful preoperative marker to identify patients at higher risk for concurrent endometrial cancer and should be considered a criterion for use of a selective SLN algorithm in patients with endometrial intraepithelial neoplasia. Endometrial stripe ≥15 mm may also be a useful parameter for gynecologists to use as a threshold to refer to gynceologic oncologists for surgical staging.
Introduction
Endometrial intraepithelial neoplasia is a common premalignant lesion of the endometrium that is associated with an approximate 40% risk of concurrent endometrial cancer.1 2 As a result, the standard of care treatment for endometrial intraepithelial neoplasia is hysterectomy, with or without adnexal surgery.3 Of those patients diagnosed with concurrent endometrial cancer, the majority are low risk and early stage; however, approximately 10% have high risk disease that warrants lymph node evaluation.1 4 5 Presently, there are no clear consensus guidelines regarding lymph node assessment in patients with endometrial intraepithelial neoplasia. Further, while surgical staging is recommended for endometrial cancer, the extent of nodal evaluation for all patients has been debated.
In 2000, Mariani et al proposed stratifying patients with endometrial cancer by risk for lymph node metastasis using pathologic criteria, known as the Mayo criteria. Patients considered low risk had a<5% chance of nodal involvement and a 96% 5 year recurrence free survival rate.6 7 Thus one commonly employed practice in patients with preoperative diagnoses of endometrial intraepithelial neoplasia is to use frozen section analysis to assess for invasive cancer and then defer lymph node evaluation in those patients considered low risk by Mayo criteria, while performing pelvic lymphadenectomy in all others.8
Pelvic lymphadenectomy, however, increases surgical time and risk of intraoperative and postoperative complications, which can lengthen hospital stays, increase healthcare costs, and decrease quality of life.6 9 10 Data from GOG 244 suggest bilateral pelvic lymphadenectomy is associated with an 18% risk of symptomatic lymphedema, and this risk is directly correlated with the number of nodes removed.11 12 Furthermore, data from the ASTEC trial found that, in patients with early endometrial cancer, routine pelvic lymphadenectomy provided no benefit in terms of overall survival or progression free survival.13
Given the associated morbidity, lack of therapeutic benefit, and marked improvements in sentinel lymph node (SLN) technology, many gynecologic oncologists have shifted to using routine SLN algorithms for staging endometrial cancer.3 4 14–18 The question of using SLN algorithms in patients with premalignant conditions such as endometrial intraepithelial neoplasia, however, remains a topic of current research. Although lymph node evaluation in patients with endometrial intraepithelial neoplasia has been relatively stable over the past 10 years, data suggest a 17.5-fold increase in the use of SLN dissection in this population from 2012 to 2018.19 Because SLN mapping cannot be performed after hysterectomy due to disruption of the lymphatic channels, the decision must be made prior to assessment for endometrial cancer in patients with endometrial intraepithelial neoplasia. As a result, some surgeons perform SLN dissection in all patients with a preoperative diagnosis of endometrial intraepithelial neoplasia at the time of surgery, prior to hysterectomy. However, given the low rates of invasive cancer in patients with preoperative diagnoses of endometrial intraepithelial neoplasia, routine SLN dissection appears to have limited benefit, and also be a more costly staging method, than hysterectomy with frozen section.20 21 These data have raised the question of preoperative stratification to inform the use of a more selective SLN algorithm.
We sought to identify preoperative characteristics associated with concurrent endometrial cancer at the time of hysterectomy among patients with endometrial intraepithelial neoplasia, to identify characteristics that may predict high risk disease, and to define a subset of patients who may benefit from SLN dissection at the time of hysterectomy.
Methods
Data Extraction
We performed a retrospective cohort study of all patients diagnosed with endometrial intraepithelial neoplasia at a single tertiary academic medical center from January 2010 to July 2020. We identified patients using the International Classification of Diseases, 10th revision code N85.02 (endometrial intraepithelial neoplasia) and International Classification of Diseases ninth revision code 621.33 (endometrial hyperplasia with atypia). A retrospective chart review was performed to extract pertinent clinical, pathologic, and oncologic data. Race and ethnicity were self-reported.
Pathology Review
Pathologic diagnoses were obtained via endometrial biopsy or dilation and curettage prior to referral for treatment. This institution’s pathology department fully adopted the endometrial intraepithelial neoplasia terminology, and its distinct classification criteria, in 2005. Therefore, all patients referred from outside institutions with a diagnosis of endometrial intraepithelial neoplasia, endometrial hyperplasia with atypia, or complex atypical hyperplasia, the equivalent of endometrial intraepithelial neoplasia in the prior WHO 94 classification system, had their pathology re-reviewed by internal gynecologic pathologists and reclassified with the endometrial intraepithelial neoplasia terminology before any medical or surgical treatment was initiated. In any situation where the primary pathologist was equivocal about the diagnosis of endometrial intraepithelial neoplasia, a second pathologist evaluated the specimen to achieve a consensus.
Inclusion Criteria
We excluded patients without pathologic confirmation of endometrial intraepithelial neoplasia after internal pathology department review, as well as those who opted for non-surgical management. Thus the study population included only patients with a confirmed preoperative diagnosis of endometrial intraepithelial neoplasia who underwent hysterectomy. Patients were not required to have preoperative imaging, however; when reported, endometrial stripe data were obtained from preoperative ultrasound. Intraoperative lymph node evaluation and frozen section analysis were performed at the discretion of the surgeon. SLN dissection, when performed, was done via a minimally invasive technique with cervical injection of indocyanine green dye and available fluorescence detection technology.
Statistical Analysis
Descriptive data are presented as median (interquartile range) or proportion. Categorical data were compared using the χ2 or Fisher’s exact test, while continuous data were compared using the Wilcoxon rank sum test. Modified Poisson regression was used to estimate risk ratios (RR) and 95% confidence intervals (CIs). All tests were two sided and p values<0.05 were considered statistically significant. Data were analyzed with SAS 9.4 (SAS Institute Inc, Cary, North Carolina, USA).
Results
Patient Characteristics
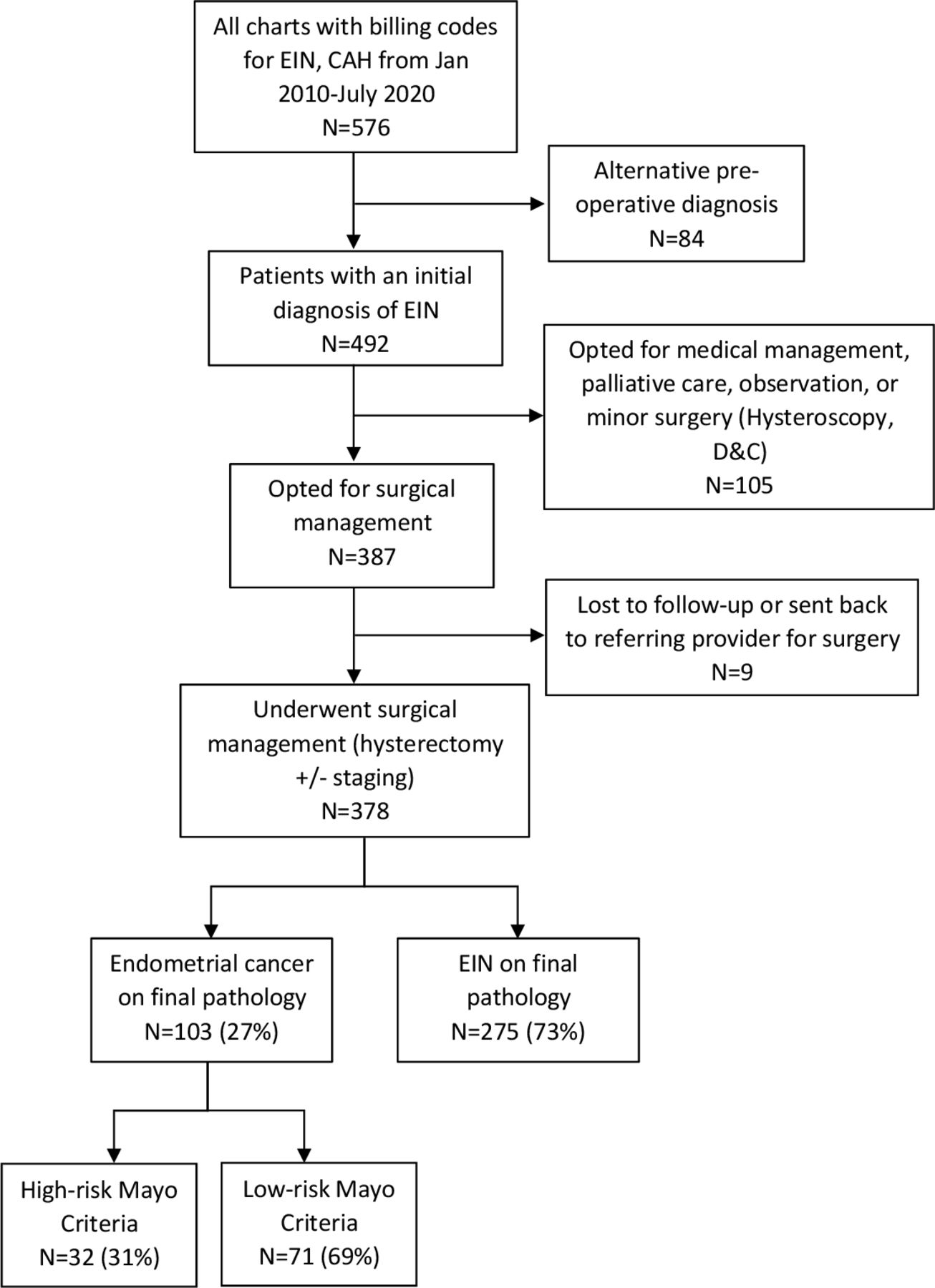
We identified 576 patients with endometrial intraepithelial neoplasia or endometrial hyperplasia with atypia. After excluding those without pathologic preoperative confirmation of endometrial intraepithelial neoplasia (n=84), those who opted for non-surgical management (n=105), and those who chose to return to alternate providers for surgery or were lost to follow-up (n=9), the study population included 378 patients with a preoperative diagnosis of endometrial intraepithelial neoplasia who underwent hysterectomy. There were 103 (27%) patients with endometrial cancer and 275 (73%) with endometrial intraepithelial neoplasia or no residual disease on final pathology (Figure 1). Most patients had surgery with gynecologic oncologists (96%, n=362); however, hysterectomies performed by generalists (2%, n=8) and specialists in minimally invasive gynecologic surgery (2%, n=8) or female pelvic medicine and reconstructive surgery (0.3%, n=1) were also included.
{kind=link}
Flow diagram of the cohort selection process and surgical pathology. Data are n (%). CAH, complex atypical hyperplasia; D&C, dilation and curettage; EIN, endometrial intraepithelial neoplasia.
Demographics for the study population are reported in Table 1. The median age of the cohort was 55 years (range, 48–62), and most self-identified as White (74%) and non-Hispanic/Latinx (81%). Compared with the endometrial intraepithelial neoplasia group, patients with endometrial cancer on final pathology were older (p=0.003), more likely to self-identify as White (p=0.02), and more likely to have hypertension (p=0.02). However, other characteristics, such as parity, body mass index, tobacco use, type II diabetes mellitus, exposure to hormonal therapies, and functional status, as determined by the American Society of Anesthesiologists physical status classification system, were not significantly different between groups (all p≥0.05).
Cohort characteristics among patients with preoperative diagnosis of endometrial intraepithelial neoplasia from 2010 to 2020
Notably, median preoperative endometrial stripe, as measured by ultrasound, was significantly greater in the endometrial cancer group (14 mm (range 10–19)) than in the endometrial intraepithelial neoplasia group (11 mm (range 8–16); p=0.002) (Table 1). The median time between preoperative ultrasound and surgery was 12 weeks (range 7–18). Patients with a preoperative endometrial stripe ≥20 mm were twice as likely to have endometrial cancer than those <20 mm (crude RR 2.0, 95% CI 1.3 to 2.9). Results were similar when comparing patients with endometrial stripe ≥15 mm with those <15 mm (crude RR 1.8, 95% CI 1.2 to 2.5). The RRs were slightly attenuated but remained statistically significant when controlling for age (Table 2).
Association between preoperative endometrial thickness and risk of endometrial cancer on final pathology
Endometrial Cancer Characteristics
Table 3 describes the tumor characteristics of patients diagnosed with endometrial cancer at the time of hysterectomy. All patients had endometrioid histology, 99% were International Federation of Gynecology and Obstetrics (FIGO) grade 1 or 2, 95% had myometrial invasion <50% (stage IA), and 71% had primary tumor diameter ≤2 cm. Only one patient (1%) had FIGO grade 3 disease, 5% had ≥50% myometrial invasion (stage IB), and 29% had primary tumor diameter >2 cm. There were no instances of stage II or greater disease. Using Mayo criteria, 69% were considered low risk for lymph node metastasis while 31% were considered high risk, representing 9% of the entire study population (Figure 1). Most of the high risk patients (84%) met Mayo criteria due to primary tumor diameter >2 cm alone.
Tumor characteristics of patients with endometrial cancer on final pathology
When stratifying patients by Mayo criteria, 45% of patients with endometrial stripe ≥15 mm were considered high risk, as opposed to 18% with endometrial stripe <15 mm (crude RR 2.5, 95% CI 1.2 to 5.2). Similar results were found when stratifying by 20 mm; however, they were not statistically significant (Table 4).
Association between preoperative endometrial thickness and Mayo criteria among patients with endometrial cancer on final pathology
Lymph Node Evaluation
Ten (3%) patients underwent intraoperative lymph node evaluation. Four of these patients had endometrial intraepithelial neoplasia on final pathology and six had endometrial cancer. Five patients underwent SLN mapping, and five patients underwent lymphadenectomy. There were no positive lymph nodes identified in this cohort. The median number of nodes evaluated was 4 (range 3–18). Of the five patients with stage IB disease, only two (40%) underwent intraoperative lymph node evaluation. Of the remaining three patients, one did not undergo frozen section and two had frozen section that incorrectly demonstrated myometrial invasion <50%. One of these patients subsequently returned to the operating room for lymphadenectomy. All five patients with stage IB disease underwent adjuvant radiation therapy.
Survival
At the time of medical record review, no documented recurrences of endometrial cancer or deaths from endometrial cancer or complications of surgery were noted. The median elapsed time from diagnosis to time of chart review was 48 months (range 26–76). Recommended follow-up was in line with National Comprehensive Cancer Network recommendations and based on final pathology. Thirty-two patients were lost to follow-up after surgery, defined as >2 years since presentation to care within this health network.
Discussion
Summary of Main Results
In a large cohort of patients with a preoperative diagnosis of endometrial intraepithelial neoplasia, we found that 27% had concurrent endometrial cancer on final pathology, with the majority being low grade and early stage. Most (69%) patients with endometrial cancer were considered low risk for lymph node metastasis by Mayo criteria, while the remaining 31% were considered high risk for nodal metastasis requiring intraoperative lymph node assessment. Of the five cases of stage IB disease noted on final pathology, at least two cases were misidentified on frozen section as <50% myometrial invasion, resulting in missed opportunities for intraoperative lymph node assessment.
When examining preoperative characteristics, older age, and increased endometrial stripe were associated with a higher risk of concurrent endometrial cancer. Patients with a preoperative endometrial stripe ≥20 mm were twice as likely to have endometrial cancer, and patients with endometrial cancer and endometrial stripe ≥15 mm were 2.5 times more likely to meet high risk Mayo criteria requiring intraoperative lymphadenectomy.
Results in the Context of Published Literature
Although lymph node evaluation remains a cornerstone in the surgical management of endometrial cancer, there remain no clear consensus guidelines regarding lymph node evaluation in patients with endometrial intraepithelial neoplasia. Several studies have demonstrated that routine SLN dissection in all patients with endometrial intraepithelial neoplasia has limited benefit and is not cost effective.20–22 Given the low grade and early stage disease in this cohort, routine SLN dissection in all patients would have resulted in overtreatment in up to 98% of patients, supporting the argument against routine SLN mapping in all patients with endometrial intraepithelial neoplasia.
In this cohort, we also observed misdiagnosis on frozen section of 40% (2 of 5) of cases of invasive stage IB carcinoma, leading to reoperation of one patient and missed opportunities for staging. Previous studies have demonstrated that, even in large academic centers with specialized pathologists, errors in frozen section at the time of surgery for endometrial intraepithelial neoplasia can lead to underdiagnosis of malignancy by up to 75%.20 Further, many patients undergoing hysterectomy for endometrial intraepithelial neoplasia may be having surgery in centers where frozen section is either unavailable or less reliable. Thus in certain circumstances, in may be appropriate to employ a risk stratification system to inform the use of selective SLN dissection in certain patients with endometrial intraepithelial neoplasia.
Data from this study suggest that increasing endometrial stripe is associated with an increased risk of concurrent endometrial cancer, particularly in patients with endometrial stripe ≥15 mm. This is consistent with prior data from Vetter et al which demonstrated that in a cohort of 169 patients with a preoperative diagnosis of endometrial intraepithelial neoplasia, those with preoperative endometrial stripe ≥20 mm were four times more likely to have concurrent endometrial cancer, and 44% of patients with a preoperative endometrial stripe ≥20 mm were considered high risk by Mayo criteria.23 Together, these data suggest that in select circumstances, preoperative endometrial stripe may be useful in identifying patients who could benefit from SLN mapping at the time of surgery.
Strengths and Weaknesses
Strengths of this study include the relatively large study population, the 10 year time frame, and specialized pathology review using endometrial intraepithelial neoplasia terminology for all specimens. Limitations include that this was a single center study with predominantly White patients in a northeast urban area which may limit its generalizability. Additionally, relatively few patients underwent lymph node evaluation, consistent with prior studies performed on patients with preoperative diagnoses of endometrial intraepithelial neoplasia. The low incidence of lymphadenectomy was likely due to surgeon preference to forego lymphadenectomy for primary tumor diameter >2 cm alone if the patient had otherwise low risk pathology on frozen section. In addition, although the cohort was larger than prior studies, it was not large enough to suggest a predictive score that would be generalizable to a significant portion of the population.
Implications for Practice and Future Research
In a large cohort of patients with a preoperative diagnosis of endometrial intraepithelial neoplasia, less than a third had invasive cancer on final pathology, with no patients having greater than stage IB disease and no patients demonstrating recurrence or death from disease, arguing against the use of routine SLN mapping in all patients with a preoperative diagnosis of endometrial intraepithelial neoplasia. However, 9% of patients undergoing hysterectomy for endometrial intraepithelial neoplasia in this cohort met high risk Mayo criteria, for which the standard of care is lymph node assessment. There are therefore clinical circumstances in which employing selective use of an SLN algorithm may be warranted. For example, institutions where frozen section is unavailable or unreliable, in patients who are high risk for morbidity from complete lymphadenectomy or re-operation, or in older patients, given the association with increased age and concurrent endometrial cancer in this cohort.
Data from this study suggest that endometrial stripe ≥15 mm may be a useful preoperative marker to identify patients not only at higher risk for concurrent endometrial cancer but also more likely to meet high risk Mayo criteria (adjusted RR 2.2). Therefore, in the above clinical scenarios, the authors believe that endometrial stripe ≥15 mm could be considered a criterion for using a selective SLN mapping algorithm in patients with a preoperative diagnosis of endometrial intraepithelial neoplasia. Additionally, for benign gynecologists offering surgical management to patients with endometrial intraepithelial neoplasia, preoperative endometrial stripe ≥15 mm may be a useful criterion for referral to a gynecologic oncologist given that this subset of patients was more likely to meet criteria for lymph node assessment.
Conclusion
Close examination of a large cohort of patients with a preoperative diagnosis of endometrial intraepithelial neoplasia who underwent hysterectomy revealed no recurrences or deaths from disease with minimal use of lymph node assessment of any kind, arguing against the routine use of SLN mapping for all patients undergoing hysterectomy for endometrial intraepithelial neoplasia. However, 9% of patients did meet high risk Mayo criteria, for which the standard of care is lymph node assessment. While continued use of frozen section to identify high risk patients is reasonable, it is not available in all practice settings and accuracy is variable. Further, there are patients for whom total pelvic lymphadenectomy would be highly morbid and SLN dissection is preferred. Ideally, preoperative risk stratification in patients with endometrial intraepithelial neoplasia would inform the use of a selective SLN algorithm which could help ensure accurate staging while decreasing morbidity. Prospective studies are warranted to further establish whether selective SLN dissection for endometrial intraepithelial neoplasia based on ultrasound endometrial stripe is a safe and cost effective alternative to current standards of care. In addition, efforts to collect data from a larger more diverse cohort is an important next step in creating a predictive score for the risk of endometrial cancer that will further inform the use of SLN dissection in this population.
Data availability statement
Data are available upon reasonable request. In accordance with the journal’s guidelines, we will provide our data for the reproducibility of this study in other centers if such is requested.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the Beth Israel Deaconess Medical Center institutional review board.
References
Footnotes
Presented at This work was presented as an oral presentation at the Society for Gynecologic Oncology Annual Meeting in March 2021, which was held virtually in the setting of COVID-19.
Contributors DA: writing-original draft preparation, data curation. AM: methodology, formal analysis, and data curation. RB: methodology and formal analysis. KME: writing-reviewing and editing. MRH: methodology, formal analysis, and writing-reviewing and editing. JD: conceptualization, methodology, supervision, writing-reviewing, editing, and guarantor.
Funding This work was conducted with support from Harvard Catalyst, The Harvard Clinical and Translational Science Center (National Center for Advancing Translational Sciences, National Institutes of Health Award UL 1TR002541), and financial contributions from Harvard University and its affiliated academic healthcare centers.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.