Article Text

Statistics from Altmetric.com
Case Presentation
A 64-year-old woman presented in July 2020 complaining of abnormal post-menopausal vaginal bleeding. She had a history of arterial hypertension, type 2 diabetes mellitus, and antiphospholipid syndrome. Physical examination showed Eastern Cooperative Oncology Group (ECOG) 0 and body mass index 23 kg/m2. Pelvic examination showed normal external genitalia and cervix, and a uterus measuring approximately 12 cm without parametrial or rectovaginal septum involvement. A transvaginal ultrasound showed a uterus with intramural fibroids and a diameter >12 cm, endometrial thickening up to 17 mm, and normal tubes and ovaries. A hysteroscopy endometrial biopsy was performed in August 2020. Pathology showed a serous adenocarcinoma. MRI demonstrated an endometrial neoplastic lesion, with invasion of >50% of the myometrium, with involvement of the cervical stroma. In addition, an enlarged retroperitoneal left para-aortic lymph node at the renal hilum level, and an enlarged retroperitoneal paracaval lymph nodes around the inferior vena cava at the distal abdominal aorta level, with the largest diameter of 5 cm, were demonstrated. The omentum and appendix appeared normal. No other intra-abdominal disease was noted (Figure 1). The patient was scheduled for laparotomy due to the size of the uterus. Anticoagulation of the patient for antiphospholipid syndrome at the time of diagnosis was suspended, and an inferior vena cava filter was inserted before surgery.

Preoperative MRI. Sagittal T2 weighted sequence shows an ill-defined endometrial infiltrative neoplastic lesion with loss of the junctional zone definition and myometrial invasion (arrows). Multiple nodular low signal myomas are also identified (A). Axial T2 weighted fat saturated FIESTA sequence images show an enlarged retroperitoneal left para-aortic lymph node at the renal hilum level, and enlarged retroperitoneal paracaval lymph nodes around the inferior vena cava at the distal abdominal aorta level (white thick arrow in B and C). FIESTA, fast imaging employing steady-state acquisition.
In September 2020, a total hysterectomy, bilateral salpingo-oophorectomy, pelvic lymphadenectomy and para-aortic debulking, omentectomy, and appendectomy were performed. Surgical findings included a uterus with multiple intramural fibroids of approximately 14 cm in size, with the appendix adhered to the uterus.
Pelvic adenopathy suspicious for disease was observed in the bilateral external iliac and common iliac region. Also, a conglomerate of lymph nodes up to 6 cm in diameter were noted in the interaortocaval and para-aortic region up to the left renal region, and these were firmly adhered to the vessels. Monopolar energy and bipolar vessel sealing devices were used to remove the lymph nodes. Hemostasis was performed with metal clips in the nodal bed. The duration of surgery was 6 hours, and blood loss was 1000 mL. The patient did not require an intraoperative blood transfusion. Postoperative hemoglobin was 9.3 g/dL. No residual disease was noted at the completion of surgery. The patient had an uneventful postoperative course and was discharged on the fifth postoperative day. The final report of the surgical pathology confirmed International Federation of Gynecology and Obstetrics (FIGO) stage IIIC2 uterine serous adenocarcinoma, with uterine serosa involvement. The appendix and omentum were without tumor. Four of 20 pelvic and 13 of 17 para-aortic lymph nodes had metastases. Adjuvant treatment with carboplatin-paclitaxel and sequential external beam radiation therapy with para-aortic extended field plus brachytherapy were recommended.
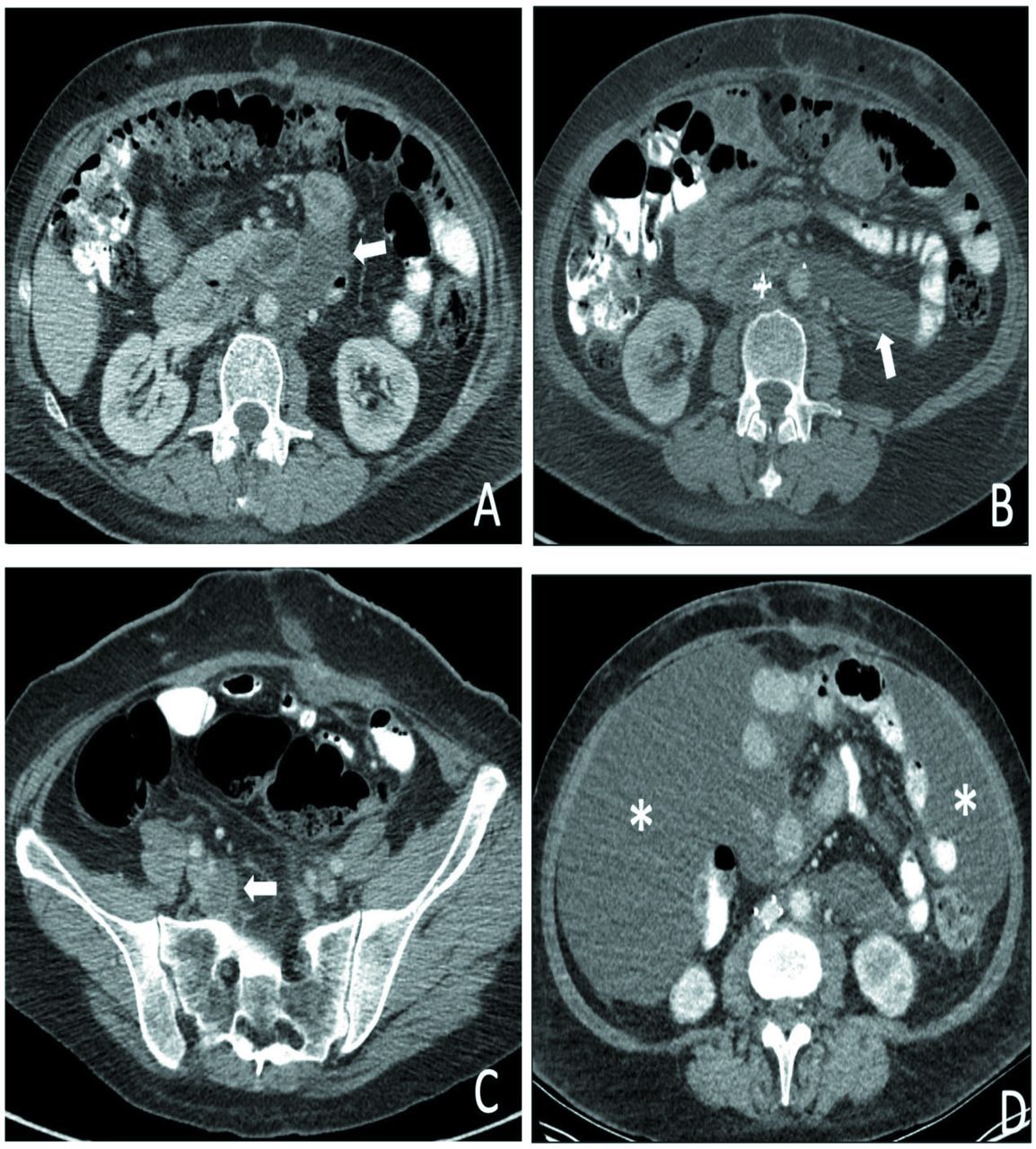
The patient returned 2 weeks after surgery reporting abdominal pain. On admission, she had normal vital signs. Physical examination revealed tenderness in the mesogastrium and right iliac fossa, without masses or signs of peritoneal irritation. The vaginal vault was without lesions. Bimanual examination was normal. No vaginal bleeding was noted. An abdominal CT revealed fluid collection below the ligament of Treitz measuring 6.5 cm at the largest diameter, and a second collection measuring 3.0 cm in the right internal iliac chain. Both of these were consistent with a lymphocyst (Figure 2A,C).

Initial postoperative CT scans shows a left retroperitoneal fluid collection consistent with a lymphocele that extends between the region below the ligament of Treitz and the anterior pararenal space (thick white arrow in A and B). There is another small lymphocele in the right internal iliac chain (thick white arrow in C) and ascites progression with an abundant amount of free intra-abdominal fluid indicated by asterisks in D.
Dr Munoz: What is the possible etiology of these collections and what management options would you recommend for this patient?
Taking into account the surgical history of para-aortic and pelvic lymphadenectomies, the location and the imaging characteristics of the collections, lymphocysts are considered the most probable diagnosis. The incidence has been reported between 1–58% in different series, with 80% of cases occurring within 2 weeks after surgery. 1 Between 3–6% are symptomatic. Treatment options described include: percutaneous catheter drainage, fine needle aspiration, sclerotherapy with an antibacterial or chemical sclerosing agent, embolization during lymphangiography, and surgical evacuation. Despite the extensive literature, there is no agreement regarding what is considered the best treatment strategy. 2 In this patient with symptomatic lymphoceles and related morbidity, a percutaneous interventional radiology procedure might have been considered.
The observation of lymphoceles was considered given that the pain was controlled in the emergency department with diclofenac. The patient was discharged home. One week later, she returned reporting pain and abdominal distension. CT scan of the abdomen showed persistence of previously documented collections and as an additional finding an abundant amount of free intra-abdominal fluid located in the perihepatic, perisplenic, paracolic gutters and pelvic cavity, not seen in the previous imaging study (Figure 2D).
At this time, it was decided to perform an abdominal drainage through percutaneous access in the right flank with an 8 French multipurpose catheter, done by the interventional radiology service. The initial drainage was 7000 mL of milky and cloudy fluid. Liquid cytochemistry was performed showing triglyceride levels of 250 mg/dL, confirming the diagnosis of chylous ascites. The patient received low osmolarity parenteral nutrition via a central line and octreotide 25 μg/hour, with a total volume of 1800 mL for 24 hours.
Dr Munoz: In the setting of chylous ascites, what are the routine recommendations and what are the anticipated success rates of these approaches?
Major surgery of the thorax and abdomen, mainly those that require extended lymph node dissection, are well known causes of chylous ascites due to direct lymphatic vessels injury. Ascites can build up as early as 1 week after the procedure or as late as several weeks to months because of adhesive syndrome or extrinsic compression of the lymphatic vessels. Its incidence after major oncological surgery is up to 7.4%. 3
The initial management for the patient with chylous ascites is to perform a paracentesis, which is not only therapeutic but is an important diagnostic tool.
The liquid is characterized by having a cloudy and turbid appearance. Triglyceride levels of the fluid are typically above 200 mg/dL, or chylomicrons above 4%, with high cell count of lymphocytic predominance and low glucose level. CT as performed on this patient determined the extent and location of the fluid, and helped guide the placement of the abdominal catheter. 4
Routine recommendations for the management of chylous ascites include the initiation of total parenteral nutrition to allow bowel rest. There is evidence that a high protein with low fat diet with medium chain triglycerides is a more reasonable approach, but no superiority is shown for one over the other. Diets with medium chain triglycerides are absorbed in the intestinal cells and are transported as free fatty acids and glycerol to the liver through the portal vein, contrary to long chain triglycerides, which transforms into monoglycerides and free fatty acids that are transported as chylomicrons to the intestinal lymph system and then to the systemic lymphatic ducts. 5
Pharmacological approaches have been reported with low evidence, suggesting the use of somatostatin and octreotide alone or in combination with total parenteral nutrition as an effective method of treatment, inhibiting lymph fluid excretion through specific receptors in the intestinal wall of lymphatic vessels. 3 4 6 Up to 71% of cases will resolve with medical and dietary recommendations between 1–6 weeks. 4
Paracentesis is performed to relieve symptoms and is usually repeated as needed. Therefore, there is no evidence of permanent drainage systems to prevent ascites and the use of these may lead to worsening of the loss of nutrients coming from the intestinal lymphatics though the leak. 3 Transjugular intrahepatic portosystemic shunts and peritoneovenous shunting are not used for this type of patient; the former is performed in patients with cirrhosis-related ascites and the latter is no longer being used because of its high association with sepsis, disseminated intravascular coagulation, and other major complications. 3 Lymphangiography with or without embolization is often used when medical treatment fails and can also give the exact location of the leak for surgical management. 3
Surgical treatment is described in the literature as being beneficial for patients with ascites due to surgical complications, and it is always performed after medical treatment has failed. Surgery has a success rate between 41–66%, when a fistula is identified and closed. However, surgical interventions for this disease are related to major complications with high morbidity and mortality rates and may also fail to identify the leak despite the use of the milk test or other methods. 3 4
The patient had evidence of improvement of her symptoms and was discharged 10 days after her admission with the recommendation of a low-lipid diet and enteric nutritional supplement with high protein content. For administrative reasons, she continued her follow-up in another institution until November 2020. The abdominal drain was removed and, after attending the emergency room twice for paracentesis obtaining up to 9000 mL at each visit, she received carboplatin 5 AUC and paclitaxel 175 mg/m2 for a total of two cycles. The last cycle was in December 2020. After the second cycle, the patient presented again with abdominal pain, distension with multiple episodes of emesis, and an inability to tolerate a diet. In addition, the patient had anemia (hemoglobin 7.8 g/dL) and thrombocytopenia (platelet count 26 000/mL blood). She required a transfusion of 2 units of red packed blood cells and apheresis of platelets.
On January 3, 2021, the patient presented to the emergency department with abdominal distension, ascites, exacerbation of pelvic pain, dyspnea, and tachycardia, and was admitted for comprehensive management. A diagnosis of severe protein-calorie malnutrition was established and it was decided to restart low-volume parenteral nutrition with the objective of volumetric and electrolyte repletion, in addition to continuous intravenous infusion of octreotide. During her hospitalization, the case was discussed in a multidisciplinary meeting with the participation of gynecological oncology, clinical oncology, interventional radiology, and surgeons of the metabolic support team. A lymphangiography with occlusion of lymphatic vessels was proposed.
Dr Munoz: At this point what were the considerations for management of this patient?
In the context of severe malnutrition, the main objective of treatment is to restore nutritional status and bring back homeostasis to prevent further complications. Determination of the presence and location of the leak allows its resolution through embolization in up to 65% of cases. 6
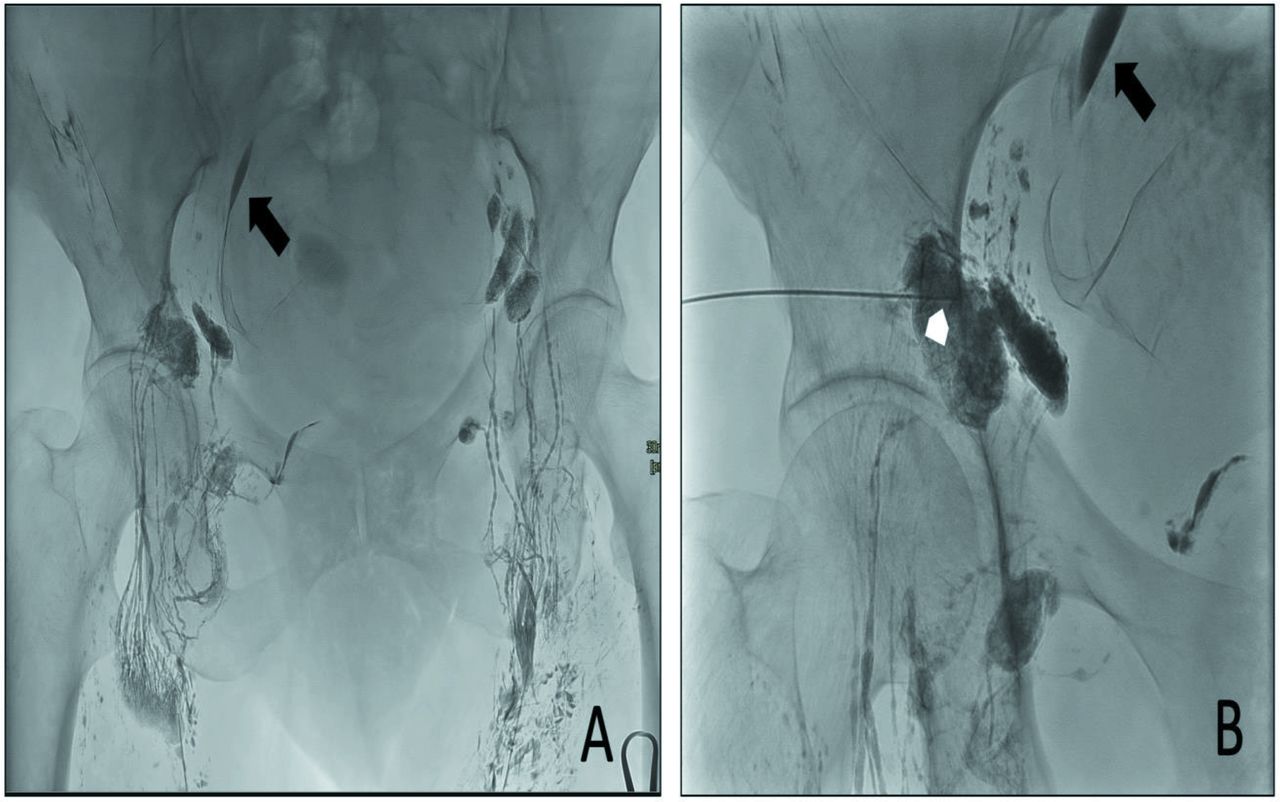
On January 27, 2021, lymphangiography and lymphatic embolization were performed under ultrasound and fluoroscopy guidance. Using a 22 g needle, percutaneous puncture of the bilateral inguinal lymph nodes was performed under ultrasound guidance and a total of 6 mL Lipiodol (ethiodized oil) was injected. Adequate opacification of lymphatic ducts was obtained in an ascending direction towards the pelvic nodal stations. At this level, contrast medium extravasation was documented due to a probable lymphatic leakage.
A direct percutaneous puncture–embolization of the pelvic lymph nodes at the level prior and closest to the extravasation level was performed. Lymph node embolization was performed with Onyx Liquid Embolic System (Onyx LES; Irvine, CA). No ascending opacification of lymphatic ducts towards the cisterna chyle was achieved. The procedure was performed without any complications (Figure 3).
{kind=link}
{kind=link}
{kind=link}
Lymphangiography and lymphatic embolization. Intranodal lymphangiography through bilateral inguinal lymph nodes demonstrates a contrast agent leakage in the right pelvic region (thick black arrow in A and B). A 22-gauge needle was inserted under fluoroscopy into the lymph node closest to the leak. Then, Onyx embolization of the lymph node was performed (white arrowhead in B).
Dr Rivero: What is the success rate of this approach and what are some of the potential adverse events with this procedure?
Cases that have failed conservative and medical therapy are considered refractory ascites. In this scenario, a feasible alternative is percutaneous interventional management. 7 Although the indications for this approach are varied, some authors have proposed its use with drainage of 1000 mL/day for 45 days or persistent drainage lasting more than 1–2 weeks despite conservative treatment. 8 Fewer than 100 cases have been described in the literature. 7
Different authors have reported success rates with lymphangiography and embolization between 35–86%, without significant minor or major complications. 7 9 Even performing repeat procedures, clinical success is achieved in up to 86% of cases, without adverse events. 9 Complications following lymphangiography are rare. The overall morbidity and mortality related to this procedure is less than 5%, the most important adverse event being pulmonary embolism associated with the volume of Lipiodol injected. 8 Infection, pain, and Lipiodol extravasation into the soft tissue have also been described. Regarding percutaneous embolization, abdominal swelling and lower extremity swelling, among others, have been mentioned. 8
Approximately 3 days after the procedure was performed, the patient presented with increased abdominal distension and abdominal pain. Abdominal ultrasound was performed, showing abundant free fluid in all abdominal quadrants, in relation to ascites.
A new paracentesis was performed, and about 9000 mL of fluid were removed. Radiation oncology proposed hypofractionated intensity modulated radiotherapy (IMRT) on the lymphatic fistula bed as complementary management.
Dr Munoz: What is the anticipated success rate of this approach and what is the mechanism of this intervention?
There is little evidence on the use of low-dose radiation therapy, which triggers an inflammatory cascade and the expression of cytokines from macrophages, leucocytes and endothelial cells, leading to scarring and fibrosis of the fistula. Hence, there are few case reports of successful leak resolution with this intervention. 10
The patient received a total of 10 Gy in five daily sessions. Given the persistence of chylous ascites 3 days later after treatment, the interventional radiology team decided to place a peritoneal catheter in the lower right quadrant of the abdomen on February 15, 2021. Since placement, the patient had persistent drainage of up to 9500 mL of fluid per day. A new multidisciplinary meeting was held and after extensive discussion, a surgical exploration was suggested. However, the patient deteriorated and had multiple comorbidities: mixed delirium, urinary tract infection complicated by Klebsiella pneumoniae, decompensation of diabetes mellitus, subacute venous thrombosis of the right subclavian vein, and deep thrombosis of the right axillary vein.
On March 1, 2021, the patient developed ventilatory failure associated with a probable episode of aspiration and septic shock, and an imaging documented cholecystitis, for which she was transferred to the intensive care unit and intubated, requiring vasopressor support. The patient then developed hemodynamic deterioration without response to multisupport measures, ventricular tachycardia, and she ultimately died from this complication.
Conclusion
There is no standard management of chylous ascites after lymphadenectomy, with little evidence from case series or expert opinion. It is initially suggested to provide medical and conservative treatment. In the face of a refractory condition, interventional management can be offered, with a low rate of complications, or surgical exploration with greater morbidity. An individualized approach with multidisciplinary participation should always be done.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the IRB Comité corporativo de ética en investigación Fundación Santa Fe de Bogotá, document number: CCEI- 14322- 2022.
Footnotes
Twitter @danielsanabrias
Contributors Study design: JR; data acquisition: JR, DS; image acquisition: OR; manuscript writing and review: JR, DS, OR, MM, RP.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.