Article Text

Abstract
Objectives We aimed to evaluate the utilization and impact of surgical para-aortic lymph node staging on the survival of patients with locally advanced stage cervical carcinoma receiving definitive chemoradiation.
Methods We identified patients in the National Cancer Database diagnosed between January 2010 and December 2015 with locally advanced (FIGO 2009 stage IB2-IVA) cervical carcinoma who did not undergo hysterectomy, received primary chemoradiation and had at least 1 month of follow-up. Two groups of patients were formed based on the assessment method of para-aortic lymph node status – radiologic assessment only versus surgical lymphadenectomy. Overall survival was compared with the log-rank test after Kaplan-Meier curves were generated. A Cox model was constructed to control for a priori selected confounders.
Results We identified a total of 3540 patients who met the inclusion criteria. Para-aortic staging was performed in 333 (9.4%) patients. These patients were younger (median age 46 vs 52 years, p<0.001), less likely to have co-morbidities (8.7% vs 15.6%, p<0.001), more likely to have private insurance (48.9% vs 37.8%, p<0.001) and receive brachytherapy (76.9% vs 70.9%, p=0.022). The rate of para-aortic lymphadenectomy was comparable between patients with stage IB2-II and III-IVA disease (9.4% for both groups, p=0.98). Patients who underwent para-aortic lymphadenectomy were also more likely to have lymph nodes categorized as positive compared with those who had imaging only (27.3% vs 13.2%, p<0.001). There was no difference in overall survival between patients who underwent radiologic only or surgical para-aortic lymph node assessment (p=0.80 from log-rank test); 4 year overall survival rates were 62.9% and 63%. After controlling for confounders, performance of para-aortic lymphadenectomy was not associated with a survival benefit (HR 1.07, 95% CIs: 0.88 to 1.31).
Conclusions In a large cohort of patients with locally advanced stage cervical carcinoma, para-aortic lymphadenectomy was rarely performed and not associated with a survival benefit.
- Cervical Cancer
- Lymph Nodes
- Radiation
- Lymphatic Metastasis
Data availability statement
Data may be obtained from a third party and are not publicly available. Data obtained from the American College of Surgeons.
Statistics from Altmetric.com
HIGHLIGHTS
Para-aortic lymphadenectomy was performed in approximately 10% patients with locally advanced cervical cancer in the United States.
Para-aortic lymphadenectomy identified a higher number of lymph node metastases.
Para-aortic lymphadenectomy was not associated with an overall survival benefit.
WHAT IS ALREADY KNOWN ON THIS TOPIC
Approximately, 10%–25% of patients with locally-advanced cervical cancer will harbor para-aortic lymph node metastases. The value of surgical staging for these patients is unclear.
WHAT THIS STUDY ADDS
Surgical staging may detect a higher number of lymph node metastases but is not associated with an overall survival benefit.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
This study’s results do not support the universal adoption of surgical staging for patients with locally-advanced cervical cancer. Further research should focus on optimal patient selection.
Introduction
Cervical cancer is the third most prevalent gynecologic malignancy in the United States; approximately 14 000 women will be newly diagnosed in 2022.1 Many patients present with locally advanced disease2 for which definitive chemoradiation is recommended.2 Presence of nodal metastases has been identified as an important prognostic factor, and approximately 10%–25% of patients with locally advanced cervical cancer will harbor metastases to the para-aortic lymph nodes.3–5 Identifying patients at high risk for para-aortic lymph node metastases can aid radiation field planning.
Positron emission tomography and computed tomography (PET-CT) is a commonly used imaging technique with sensitivity ranging from 82% to 95%.3–5 However, for patients with pelvic lymph node involvement, the false negative rate can be as high as 22%.4 5 As such several authors have advocated in favor of surgical staging that permits the pathologic examination of lymph nodes and accurate staging.4 5 Nevertheless, para-aortic lymphadenectomy may be associated with post-operative complications that could potentially delay definitive radiotherapy administration, and with an increased incidence of lower extremity lymphedema.4–6 Evidence to guide treatment recommendations mainly derives from retrospective studies, and there is significant practice variation.7–11 Moreover, a recent randomized trial (UTERUS-11), did not demonstrate any difference in disease-free survival between clinical and surgical staging.12 The present study aimed to evaluate national trends in the utilization of surgical staging for patients with locally advanced cervical cancer, using a large hospital-based database. In addition, we aimed to examine overall survival when compared with conventional radiologic staging.
Methods
The National Cancer Database was accessed to identify patients diagnosed between January 2010 and December 2015 with a pathologically confirmed locally advanced squamous cell, adenosquamous or adenocarcinoma of the cervix. Staging was based on the International Federation of Gynecology and Obstetrics (FIGO) 2009 stage (stage IB2-IVA) variable provided by the Collaborative Staging Schema, or the clinical stage variables. Patients who received external beam radiation therapy (with or without vaginal brachytherapy) of at least 45 Gy with radio-sensitizing chemotherapy, did not undergo hysterectomy, had known data on the mode of para-aortic lymph node assessment (surgical vs imaging only) and at least 1 month of follow-up were selected for further analysis. Data were derived from the Collaborative Staging Schema variables ‘assessment method of para-aortic nodal status’ and ‘para-aortic nodal status’. Potentially misclassified cases were excluded based on data from the pathology report. For patients undergoing lymphadenectomy, the status of resected lymph nodes was determined from the pathology report. (Online supplemental figure 1 depicts the patient selection flowchart).
Supplemental material
The National Cancer Data Base is a hospital-based database capturing approximately 70% of all malignancies diagnosed in the United States. The American College of Surgeons and the Commission on Cancer have not verified and are not responsible for the analytical or statistical methodology employed, or the conclusions drawn from these data. The present study was deemed exempt from Institutional Board Review from Penn Medicine (Protocol #829268).
Demographic, clinico-pathological, and treatment characteristics were extracted from the de-identified dataset. For analysis purposes, insurance status was recoded into Private, Government (including Medicaid and Medicare) and Uninsured/Unknown while patient age was dichotomized into <50,>50 years based on median age of menopause in the United States. The presence of co-morbidities was assessed from the Charlson-Deyo Comorbidity Index and classified as Absent (score 0) or Present (score >1). Lastly, the type of treatment facility was categorized into academic/research and non-academic that included community cancer program, comprehensive community cancer program, and integrated network cancer program. The type of treatment facility is not provided for patients aged <45 in line with the National Cancer Database’s mission to protect patient identity.
The frequency of distribution of categorical variables was compared with the Chi-Square test and continuous variables with the Kruskall-Wallis test. Overall survival was assessed following generation of Kaplan-Meier curves and compared with the log-rank test. A Cox model was constructed to control for a priori selected confounders known to be associated with overall survival. Statistical analyses were performed with the Statistical Package for the Social Sciences v.27 (International Business Machines Corporation, Armonk, New York) and the alpha level of statistical significance was set at 0.05.
Results
A total of 3540 patients with locally advanced cervical carcinoma who met the inclusion criteria were identified; para-aortic lymphadenectomy was performed in 333 (9.4%) patients. Utilization of para-aortic lymphadenectomy overall decreased from 15.7% in 2010 and 11.2% in 2011, to 8.6% in 2012, 6.5% in 2013, 8.3% in 2014 and 8.9% in 2015. Data on the type of treatment facility were available for 2865 patients; 46.4% were managed at academic centers. The rate of para-aortic lymphadenectomy was 11.3% for patients diagnosed between 2010–2012 compared with 7.9% for those diagnosed between 2013–2015, p<0.001. Patients who underwent para-aortic lymphadenectomy were younger (median age 46 vs 52 years, p<0.001), less likely to have comorbidities (8.7% vs 15.6%, p<0.001), more likely to have private insurance (48.9% vs 37.8%, p<0.001) and receive brachytherapy (76.9% vs 70.9%, p=0.022).
For patients undergoing para-aortic lymphadenectomy, based on pathology reports 14.2% had 1–4 lymph nodes removed, 20.1% had 5–9, 36.5% had 10–20 and 29.2% had >20 lymph nodes removed. Among patients with positive lymph nodes, 52.2% had 1–2 positive lymph nodes, while 27.4% and 20.4% had 3–5 or >5 positive lymph nodes; respectively. Table 1 summarizes the clinico-pathological characteristics of the patient population stratified by the mode of para-aortic lymph node assessment. Patients who underwent para-aortic lymphadenectomy were also more likely to have lymph nodes categorized as positive compared with those who had imaging only (27.3% vs 13.2%, p<0.001) and a longer interval between cancer diagnosis and radiation therapy initiation (median 55 vs 38 days, p<0.001). The type of external beam radiation therapy was reported for 1625 patients, 62.2% received intensity-modulated radiation therapy (65.1% in the lymphadenectomy and 62% in the clinical imaging group respectively, p=0.48). The majority of patients completed radiation treatment within 62 days from initiation (70.4%) with comparable rates between the surgical and imaging only groups (73.6% vs 70.1%, p=0.40). The overall rate of brachytherapy use in the present cohort was 73.4%, and it was higher among patients managed in academic facilities (77.6% vs 68.6%, p<0.001).
Clinico-pathological and demographic patient characteristics
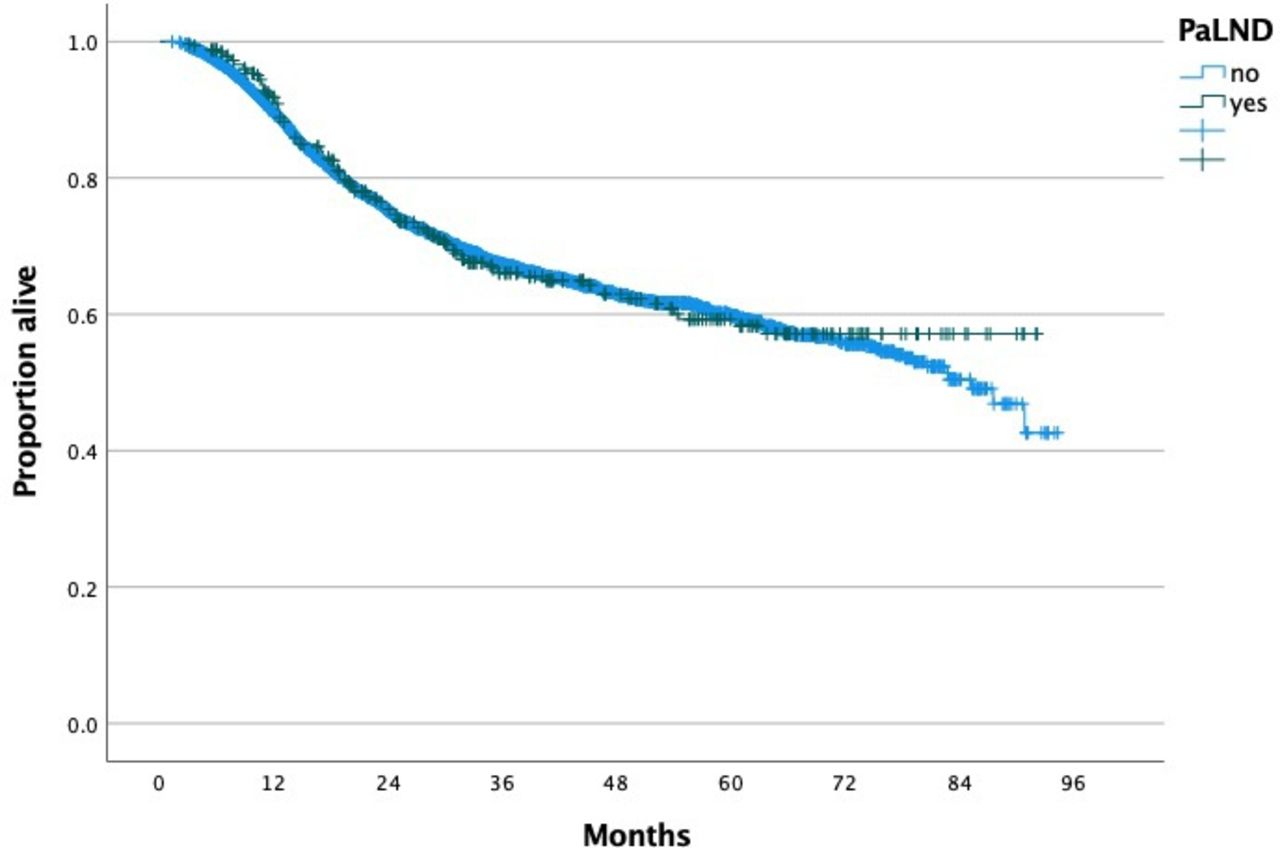
Based on the reverse Kaplan-Meier estimator method, median follow-up in the radiologic and surgical para-aortic staging groups was 40.25 and 41.1 months respectively. There was no difference in overall survival between patients who underwent radiologic (1000 deaths) or surgical (108 deaths) para-aortic lymph node assessment, p=0.80 from log-rank test; 4 year overall survival rates were 62.9% and 63% respectively (Figure 1). After controlling for patient age, race, insurance status, tumor stage, histology, presence of comorbidities, history of another tumor, and receipt of vaginal brachytherapy, performance of para-aortic lymphadenectomy was not associated with a survival benefit (HR 1.07, 95% CI: 0.88 to 1.31). Following stratification by disease stage there was no difference in overall survival between the radiologic and surgical para-aortic staging groups for patients with stage IB2 (p=0.29; 4 year overall survival rates 77.6% vs 72.7%), stage II (p=0.13; 4 year overall survival rates 72.4% vs 66.4%), stage III (p=0.08; 4 year overall survival rates 51% vs 57.6%), and stage IVA disease (p=0.63; 4 year overall survival rates 44.5% vs 40%).

{kind=link}
Overall survival of patients with locally-advanced cervical cancer stratified by mode of para-aortic staging.
Similarly, following stratification by type of treatment facility, there was no overall survival difference between the radiologic and surgical para-aortic staging groups for patients treated in academic (p=0.14; 4 year overall survival rates 63.7% vs 57%) or non-academic (p=0.15; 4 year overall survival rates 65.1% vs 62.4%). In a sensitivity analysis, when excluding patients who did not receive brachytherapy, after controlling for confounders performance of surgical staging was not associated with an overall survival benefit (HR 1.04, 95% CI 0.82 to 1.33). In addition, when selecting patients who had at least 10 lymph nodes removed (n=209), surgical staging was not associated with an overall survival benefit (HR 1.01, 95% CI 0.78 to 1.30) compared with radiologic staging. Lastly, for patients undergoing surgical staging, presence of para-aortic metastases was associated with worse overall survival after controlling for comorbidities, stage, patient age and receipt of brachytherapy (HR 2.09, 95% CI 1.41 to 3.12).
Discussion
Summary of main results
In a contemporary large cohort of patients with locally advanced cervical carcinoma, surgical para-aortic staging was rarely utilized (9.4%) in the United States. A higher rate of para-aortic lymph node metastases was observed among patients who underwent lymphadenectomy. However, overall survival was comparable between the radiologically and surgically staged patients after controlling for confounders.
Results in the context of published literature
Data comparing surgical to clinical staging in the cervical cancer population has been mixed with respect to feasibility, safety, and overall survival outcomes.7–11 For example, a retrospective study by Pomel et al evaluated 187 patients with locally advanced cervical cancer. The authors demonstrated that patients undergoing para-aortic lymph node dissection had lower disease-free survival compared with clinical staging.10 On the other hand, Ramirez et al prospectively compared the sensitivity of PET-CT to surgical staging.13 A total of 60 patients were enrolled and underwent both PET-CT and extraperitoneal para-aortic lymphadenectomy. Among patients who had negative pelvic and para-aortic lymph nodes on PET-CT (n=26), para-aortic metastases were found in 12%, while for patients who had positive pelvic but negative para-aortic lymph node on PET-CT (n=27) the incidence of para-aortic metastases was 22%. Overall, treatment modification following surgical staging occurred in 11 patients (18.3%). In a recent meta-analysis, Delara et al reported comparable oncologic outcomes between surgical and clinical staging.11 Authors included data from five studies, with a total of 1112 patients with FIGO 2009 stage IB2-IVA cervical cancer; 754 of them had surgical staging.11 Based on 132 patients who underwent para-aortic lymphadenectomy, the rate of lymph node metastases was 33% and comparable to the rate of metastases observed in our study.11 Based on data from four studies, there were no differences in progression-free survival (HR 1.13, 95% CI 0.73 to 1.74) or overall survival (HR 1.06, 95% CI 0.66 to 1.69) between surgical and imaging staging groups, although significant heterogeneity was found (I square 75%).11 Finally, two studies evaluated the concordance between imaging and surgical staging for the detection of para-aortic lymph node metastases and reported a relative low sensitivity (33.3%–62.5%) but a high specificity (92%–95.5%).11 In a pooled analysis of 685 patients with locally advanced cervical cancer who participated in three large phase III Gynecologic Oncology Group (GOG) trials, 555 patients underwent surgical para-aortic lymph node sampling.14 By multivariable analysis, radiologic staging was associated with worse progression-free survival (HR 1.35, 95% CI 1.01 to 1.81) and overall survival (HR 1.46, 95% CI 1.08 to 1.99) while a higher rate of para-aortic relapse was observed (31.9% vs 15.1%, p=0.006).14
Given the potential bias of retrospective studies, three randomized controlled trials have so far attempted to address the role of surgical staging in managing patients with locally advanced cervical cancer.12 15 16 A two-step randomized trial from Taiwan was terminated following recruitment of 61 patients after an interim analysis demonstrated significantly worse progression-free survival (HR 3.13, p=0.005) in the surgical staging arm.15 In that study the rate of para-aortic lymph node metastasis in the surgical arm was again comparable to our study (25%).14
A recently published, multi-institutional international randomized controlled trial (UTERUS-11) recruited 255 patients with stage IIB-IVA cervical cancer between 2009 and 2013. The patients had received pelvic external beam radiation therapy, weekly cisplatin and brachytherapy, and were randomized to radiologic staging (with biopsy if suspicious findings) or laparoscopic surgical staging.12 16 For the 121 patients who underwent surgical staging (transperitoneal approach for 93.4%), no intra-operative death occurred, while only 1 (0.8%) patient had conversion to laparotomy, and excessive blood loss (>500 mL) was observed in two patients.17 The post-operative complication rate was also low (7.3%) demonstrating that laparoscopic surgical staging is safe in this patient population with minimal peri-operative morbidity.16 Among patients undergoing surgical staging, 51% had positive pelvic lymph nodes and 24% had positive para-aortic lymph nodes, resulting in the upstaging of 33% of patients compared with 8% in the clinical arm (by CT-guided lymph node biopsy).12 Importantly, there was no difference in the time to primary chemoradiation between the two groups (median of 13 vs 13.5 days in the surgical and clinical group, respectively).12 15 Despite the significant difference in upstaging, and the resulting change in radiation therapy treatment planning, there was no difference in disease-free survival between the two groups (adjusted HR 0.73, 95% CI 0.49 to 1.08, p=0.12).12 However, surgical staging was associated with better cancer-specific survival (HR 0.61, 95% CI 0.40 to 0.93) and in an ad-hoc analyses, with better progression-free survival for patients with stage IIB disease (HR 0.51, 95% CI 0.30 to 0.86).12 It should be mentioned that cancer-specific survival was not one of the trial endpoints while stratification by disease stage was not pre-planned. In our study, we found a longer interval between diagnosis and initiation of radiation therapy for patients who underwent surgical para-aortic staging (median 55 vs 38 days, p<0.001). Whether this difference is related to barriers to health care access, delay in final stage assignment or increased rate of complications remains unclear.
Strengths and weaknesses
A major strength of our study is the inclusion of a large cohort of patients derived from a hospital-based database reflecting current real-world practice in the United States. Several limitations should be mentioned. First, given the absence of a central pathology report, possible histology and stage misclassifications cannot be ruled out. While all patients who underwent surgical staging had pathologic examination of the resected lymph nodes, information on the presence of micro or macrometastases was not provided, and we could not verify whether lymph node counts included exclusively para-aortic lymph nodes. Interestingly, a large percentage of patients in both surgical and radiologic staging groups did not receive brachytherapy contrary to national guidelines. Moreover, the National Cancer Database does not collect data on tumor recurrence precluding us from analyzing differences in progression-free survival and the pattern of relapse. In addition, no data on the imaging modality employed (PET-CT, magnetic resonance imaging (MRI) or CT) to evaluate para-aortic lymph node metastases in the clinical or surgical staging group were available. While all patients underwent definitive chemoradiotherapy, information on the extent of radiation fields and whether para-aortic lymph node basins were included was not available. For patients undergoing surgical staging, we did not have data on the route of lymphadenectomy (intra-peritoneal or extra-peritoneal) that could theoretically impact peri-operative outcomes17 or data on the upper border of dissection. Also, data on patient reported quality of life or the incidence of treatment related toxicity were not available. For patients who had only radiologic staging, we could not assess whether biopsy of any suspicious lymph nodes was performed. Lastly, unmeasured factors such as patient functional status and the individual surgeon’s preferences may have influenced the decision to perform surgical staging.
Implications for practice and further research
Surgical staging for locally advanced cervical carcinoma identifies a higher percentage of para-aortic lymph node metastases and is not associated with a significant delay in definitive treatment initiation. However, there was no clear benefit in overall survival compared with clinical staging. Further data from prospective studies are required to elaborate the role of surgical staging in locally advanced cervical carcinoma and identify patients who would benefit the most.
Conclusions
Surgical staging is rarely employed in managing locally advanced cervical cancer in the United States. There was no difference in overall survival between clinically and surgically staged patients.
Data availability statement
Data may be obtained from a third party and are not publicly available. Data obtained from the American College of Surgeons.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors All authors contributed to the manuscript. DN was responsible for the conception, data acquisition, data management, statistical analysis, critical analysis, drafting/final editing and serves as guarantor. MR, NT, AH, SK, EK, LC, RG were responsible for critical analysis, drafting/final editing. NL was responsible for supervision, critical analysis, drafting/final editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None related to this study RL: medical monitor for CAPRI trial by Astra ZenecaAH: GSK research fund, GSK advisory board, Honoraria: Axess ovarian cancer lecture.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Linked Articles
- Editorial
- Letter
- Letter
- Letter