Article Text

Statistics from Altmetric.com
Case Presentation
In 2017, a 35-year-old G1P0 presented with unexplained infertility. A cervical smear, performed as part of routine evaluation, showed a high grade intraepithelial lesion with features of adenocarcinoma in situ. She proceeded to colposcopy assessment and in November 2017, had a large loop excision of the transformation zone with a specimen size of 1.7×1.7 x 1.7 mm. Pathologic examination of this large loop excision of the transformation zone showed adenocarcinoma in situ which extended to the endocervical excision margin. A repeat (top hat) large loop excision of the transformation zone was performed in January 2018 and despite this attempt at re-excision, adenocarcinoma in situ was present and again the endocervical margins were positive. In view of the persistent positive margins and her wish to maintain fertility, she was referred to the tertiary gynecology oncology department for additional assessment. Physical examination revealed a post large loop excision of the transformation zone cervix, flush with the vagina. Magnetic resonance imaging (MRI) demonstrated approximately 1 cm of residual cervix remaining. No additional imaging abnormality and no lymphadenopathy was identified.
With these results, potential management options were discussed in detail with the patient and her partner. The innate difficulties of monitoring and diagnosing adenocarcinoma in situ in the endocervical canal were highlighted. In view of her previous positive margins on large loop excision of the transformation zone, a hysterectomy was advised. As the patient was keen to retain fertility, she declined this option and options for surveillance and monitoring to support a successful pregnancy were discussed. In May 2018, a plan was agreed that clinical surveillance would be undertaken and that a Pap smear with human papillomavirus (HPV) testing would be performed 6 months after the consultation and that if the cytology and HPV were negative, a laparoscopic cervical cerclage would be performed.
In November 2018, the patient had a HPV negative Pap smear with normal cytology and underwent an uncomplicated laparoscopic cerclage insertion and subsequent cervical dilation to assist embryo implantation. She became pregnant in 2019. At 38 weeks, an elective lower segment cesarean section of a healthy baby boy was performed in a standalone maternity hospital. At the time of the cesarean section, a right sided 10 cm ovarian cyst was identified and a cystectomy was performed. Histology demonstrated a borderline mucinous ovarian tumor. A 6 month follow-up pelvic ultrasound, performed in the maternity hospital, was normal.
One year after the birth of her baby, she re-attended the gynecology oncology department for follow-up. The gynecological oncologist was made aware of her borderline mucinous tumor diagnosed at cesarean section when the patient presented for review to consider a cervical dilatation to enable another cycle of in vitro fertilization. A hysteroscopy with endometrial and endocervical curettage was performed. Histology from curettings demonstrated recurrent (endocervical) adenocarcinoma in situ of the endometrial cavity. Immunohistochemistry was positive for p16, in keeping with a HPV induced process (Figure 1). Simultaneously, the previously resected borderline mucinous ovarian cyst was re-evaluated. Immunohistochemistry demonstrated p16 expression in mucinous epithelium of the ovary, and in situ hybridisation for HPV demonstrated HPV in mucinous epithelium of the ovary (Figure 2A,B). This demonstrated that the ovarian mucinous lesion arose as a result of a HPV driven process, suggesting that the ovarian process was secondary spread from a mucinous lesion of the endocervix. Radiological staging was undertaken as outlined below.

Endometrial curettings (hematoxylin–eosin) demonstrating endocervix adenocarcinoma in situ. The complex architecture is evident, with cribiform glands and abundant mitosis and apoptosis.
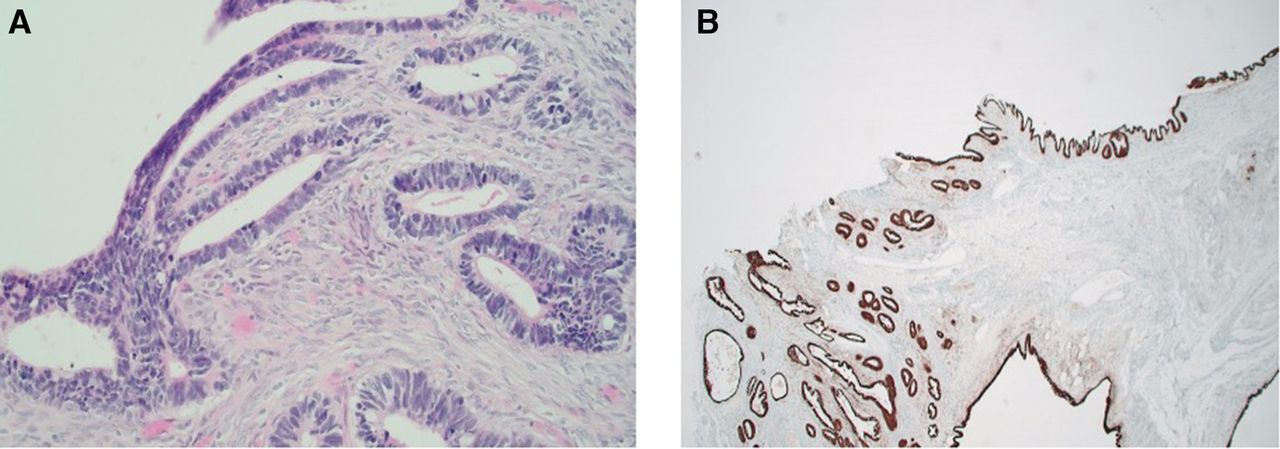
Immunohistochemistry (hematoxylin–eosin and p16) of ovarian cyst. (A) High power of ovarian cyst removed at cesarean section. The cyst was multi-loculated and lined by mucinous epithelium and hyperchromatic nuclei. At high power, clearly demonstrated is complex architecture with cribiform glands and mitotic activity. Its histological appearance is similar to adenocarcinoma in situ proliferation in the endocervix and endometrium. (B) p16 immunohistochemistry of the endometrium. Diffuse strong positivity for p16 was demonstrated on the sample. This was later confirmed with human papillomavirus in situ hybridization.
Radiology: Dr Geoghegan
A computed tomography (CT) scan of the thorax, abdomen, and pelvis was performed as a staging procedure which demonstrated a 4.6×3.2 cm right adnexal cyst with some internal septations ( Figure 3A ). Appearances suggestive of benign intrapulmonary lymph nodes were also identified abutting the left and right major lung fissures. Overall, there was no evidence of metastatic disease on imaging. An MRI, to further characterize the right adnexal cyst, demonstrated a 5.5×3 x 4 cm cyst with numerous septations. Some of these were nodular in appearance with restriction on diffusion weighted imaging. This was a new appearance in comparison with previous imaging. On the T1 fat saturated image, there were some bright signals which raised the possibility of some hemorrhage within the cyst. There was also a complex 2.1 cm left ovarian cyst containing some thickened internal septations and peripheral enhancement, suggestive of a corpus luteal cyst. Some soft tissue thickening was noted in the endocervical canal. Although the cervix was outside the field of view, the endocervical junction appeared normal.

Preoperative imaging. (A) Sagittal computed tomography demonstrating a 4.2×3.6 cm right adnexal cyst. (B) Positron emission tomography scan shows a complex right adnexal cyst with a small focus of fluorodeoxyglucose accumulation (standardized uptake value max 2.4). (C) There is a small focus of fluorodeoxyglucose accumulation to an standardized uptake value max of 4.5 within the cervix/proximal uterus concerning for a small focus of malignancy.
This patient proceeded to have a positron emission tomography scan ( Figure 3B,C ). This demonstrated a small focus of fluorodeoxyglucose (FDG) accumulation to a standardized uptake value max of 4.5 within the cervix/proximal uterus. This raised concerns for a focus of malignancy. A complex right adnexal cyst, with a small focus of FDG accumulation (standardized uptake value (SUV) max 2.4) and a left adnexal cyst with a standardized uptake value max of 5.6 were also noted.
Surgical Procedure: Professor Brennan
Following extensive consultations with the patient and detailed multidisciplinary team discussion, it was felt that there was a significant risk that this patient may have an invasive adenocarcinoma of the cervix. Based on her history of a mucinous borderline ovarian tumor and radiology findings outlined above, there was a significant concern that she may have ovarian involvement. Although this would not change her International Federation of Gynecology and Obstetrics (FIGO) stage, based on FIGO 2018 staging, it would impact on her prognosis. Clinically and radiologically, the cervical remnant was <1 cm, and therefore we did not feel there was scope for a fertility preserving option in this case and thus proceeded to perform a radical hysterectomy, bilateral salpingo-oophorectomy, and laparoscopic sentinel lymph node biopsy. As this patient already had disease in her ovary, it was felt that the risk associated with laparoscopy were low. Although the Laparoscopic Approach to Cervical Cancer (LACC) trial demonstrated worse survival with the minimally invasive approach in early stage cervical cancer, 1 laparoscopy is still used in certain settings to resect metastatic lymph nodes and stage advanced cervical cancer.
At the time of surgery, a small cyst was noted on the right ovary. Thorough examination of the rest of the abdomen demonstrated no evidence of peritoneal disease. Laparoscopic sentinel lymph nodes were identified and resected in the right external iliac region, obturator fossa on the left, and paracaval lymph node. At laparotomy, a type C1 radical hysterectomy and bilateral salpingo-oophorectomy, appendectomy, and omental biopsy was performed. The appendix was removed due to the history of a previous borderline mucinous ovarian tumor.
Histology: Dr Ann Treacy
The hysterectomy and salpingo-oophorectomy specimen weighed 74 g. The uterus measured 40×40×45 mm. The cervix measured 15×15×10 mm and appeared disrupted with no gross tumor identified. The vaginal cuff measured 20 mm. The right ovary was submitted separately, measuring 60×30×20 mm, with a smooth external surface and a multicystic cut surface; the left ovary was 20×20×20 mm.
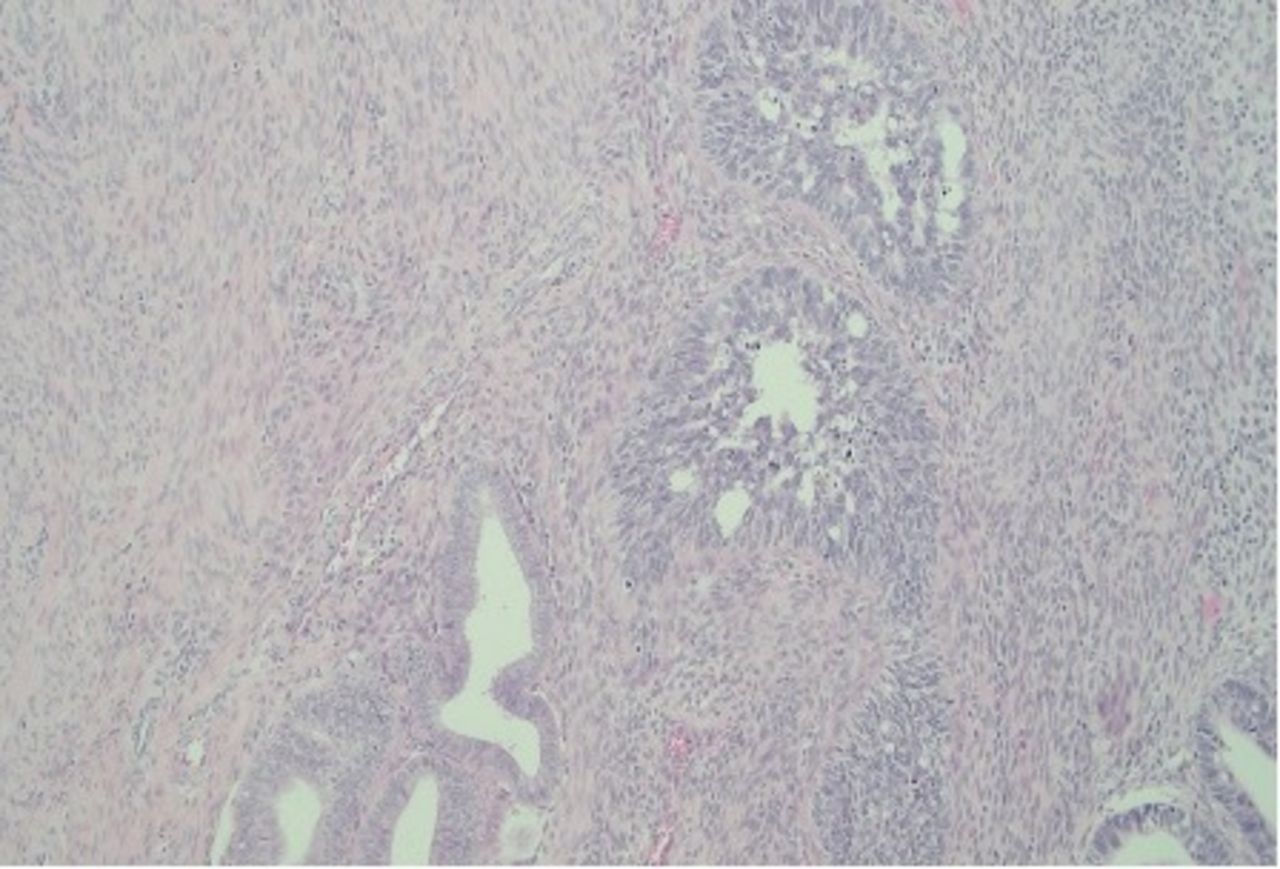
The entire cervix was embedded sequentially and demonstrated extensive adenocarcinoma in situ with no invasive adenocarcinoma. Adenocarcinoma in situ extended to involve the lower uterine segment and endometrium ( Figure 4A,B ). The ectocervical margin was >10 mm from in situ adenocarcinoma. Within the parametrium, a focus of endometriosis was noted. The right ovary was distended with a mucinous tumor measuring 60 mm, showing stratification, abundant mitoses, and apoptotic bodies, in keeping with morphological appearances of endocervical adenocarcinoma in situ. Immunohistochemical studies showed positive staining with p16. The right and left fallopian tubes, left ovary, omental biopsy, and appendix were normal. All sentinel lymph nodes (pelvic ×2, paracaval ×1) were negative for malignancy, which was confirmed on levels and immunohistochemistry. In conclusion, cervical adenocarcinoma in situ was present in the endocervix, endometrium, and right ovary ( Figure 4C ). Comparison with hematoxylin–eosin slides from the previous ovarian cyst showed similar appearances.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Histology from resected specimen, endometrium. (A) Endometrium from resected uterus. Normal appearing endometrium on the right and adenocarcinoma in situ to the left, extending from the endocervix to the lower uterine segment (B) Schematic representation of the pathology showing the extent of adenocarcinoma in situ (AIS), involving the endometrium and right ovary. The omentum, appendix, and left ovary were not involved.
Professor Brennan: Based on the Clinical and Histological Findings, What Would be the Recommended Follow-up for this Patient?
This is an unusual case of metastatic cervical adenocarcinoma in situ, and emphasizes the importance of thoroughly investigating mucinous borderline tumors of the ovary, with particular emphasis on screening history of any cervical dysplasia. Surveillance of metastatic spread is also challenged in view of the rare nature of this presentation and lack of supporting data. While metastatic adenocarcinoma in situ of the cervix to the ovary is rare, additional sites of metastasis, such as pulmonary lesions, have been reported. 2 Prognostic data from metastatic adenocarcinoma in situ is limited; however, overall prognosis is favorable with no evidence of disease after a median of 63.4 months. 3–5 While some reports describe patients who required adjuvant treatment in the form of radiotherapy or chemotherapy, they also appear to perform well, remaining disease free as far as 5 years after diagnosis. 5
Our recommendations on follow-up reflect the international evidence to date. Our patient was recommended close monitoring with regular clinical examination on a 3 monthly basis. In order to detect metastatic spread, such as pulmonary deposits, 2 imaging in the form of CT thorax/abdomen/pelvis on an annual basis for 3 years was recommended. In addition, she was advised to have the HPV vaccination and will attend for annual vault smears.
Closing Summary and Discussion: Dr Paul Downey
This unusual case of metastatic carcinoma to the ovary from cervical adenocarcinoma in situ highlights some of the challenges in the diagnosis and monitoring of women with high grade, non-invasive glandular abnormalities of the cervix. In general, the majority of cervical adenocarcinomas (>90%) are associated with high risk HPV, and pathologic demonstration of p16 immunohistochemical expression is a good surrogate marker for this. 2 Adenocarcinoma in situ has the potential to progress to invasive adenocarcinoma and can metastasize in a conventional manner through lymphatic and vascular spaces. 6 While spread of non-invasive tumors of the ovary and fallopian tube is well recognized (so-called drop down metastasis to the endometrium/cervix), spread of cervical adenocarcinoma in situ in a similar fashion (although in the opposite direction) is less well recognized and the mechanism of dissemination is unknown. 6
The diagnosis of a metastatic tumor to the ovary can be difficult, especially where there is no history of an invasive lesion. Although metastatic tumors to the ovary often result in bilateral ovarian enlargement in older women, spread to the ovary from a cervical adenocarcinoma in situ can present with both clinical and histological features consistent with an ovarian primary tumor (with mucinous or endometrioid morphology) and can pose significant challenges to the diagnosis. 2–4 Furthermore, spread to the ovary from in situ disease may have radiological features consistent with a primary tumor, such as a solid cystic appearance and unilateral presentation, and thus may not raise suspicion of metastatic disease. 2 The challenge is compounded in the case of a synchronous cervical and ovarian tumor, lacking the typical histological features associated with metastatic invasion.
Primary ovarian tumors are independent of HPV infection 7 and thus testing for the presence of HPV (directly or indirectly through the use of p16 immunohistochemistry) will help correctly identify metastatic spread to the ovary in most cases, especially where there is a known history of cervical glandular neoplasia. 7–10 In a case series of 29 synchronous endocervical and ovarian tumors, occurring as a result of metastatic spread from the cervix to the ovary, 26 of 29 specimens exhibited histological appearances mimicking primary ovarian borderline (atypical proliferative) mucinous tumors with ‘borderline like’ glandular cribiform and/or villoglandular patterns. 3 As only three ovarian tumors had conventional features typically associated with metastatic spread (bilateral presentation, infiltration), paired testing of the endocervical and ovarian tumors for identical HPV types was required to confirm the ovarian tumors as being metastases from a cervical primary.
In the context of a mucinous ovarian lesion, judicious use of p16 immunohistochemistry may be helpful in identifying metastatic mucinous tumors of cervical origin. Although there are potential pitfalls, diffuse expression of p16 can serve as a sensitive and specific marker for the identification of HPV related endocervical adenocarcinomas 2 and could serve as a useful adjunct (in addition to the differential cytokeratins CK7 and CK20 and other immunohistochemical markers) when assessing the possibility of metastatic spread to the ovary.
The mechanism by which ovaries become involved by cervical adenocarcinoma in situ is poorly understood and it is recognized that transtubal spread from the cervix to the ovary can occur with or without involvement of the endometrium and without evidence of invasion. This has been likened to 'seed and soil' spread of disease. 2 While this pattern of spread is thought to have a relatively good prognosis, 2 4 it is debatable about how this pattern of spread is best staged.
Conclusion
A thorough history of any cervical glandular abnormality should be available for all patients with a diagnosis of a mucinous ovarian cyst/tumor. Where this history is not forthcoming, p16 immunohistochemistry may be used to identify spread to the ovary from a cervical primary, especially where a diagnosis of a mucinous borderline (atypical proliferating) tumor is being considered.
Ethics statements
Patient consent for publication
Footnotes
Contributors All authors contributed to the planning, writing, and editing of this case report.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.