Article Text

Abstract
Objectives To assess the effect of complete surgical staging and adjuvant chemotherapy on survival in stage I, low grade endometrioid ovarian cancer.
Methods This retrospective study was conducted at two cancer centers from July 2001 to December 2019. Inclusion criteria were all stage I, grade 1 and 2 endometrioid ovarian cancer patients. Patients with mixed histology, concurrent endometrial cancer, neoadjuvant chemotherapy, and patients who did not undergo follow-up at our centers were excluded. Clinical, pathologic, recurrence, and follow-up data were collected. Cox proportional hazard model evaluated predictive factors. Recurrence-free survival and overall survival were calculated using the Kaplan-Meier method.
Results There were 131 eligible stage I patients: 83 patients (63.4%) were stage IA, 5 (3.8%) were stage IB, and 43 (32.8%) were stage IC, with 80 patients (61.1%) having grade 1 and 51 (38.9%) patients having grade 2 disease. Complete lymphadenectomy was performed in 34 patients (26.0%), whereas 97 patients (74.0%) had either partial (n=22, 16.8%) or no (n=75, 57.2%) lymphadenectomy. Thirty patients (22.9%) received adjuvant chemotherapy. Median follow-up was 51.5 (95% CI 44.3 to 57.2) months. Five-year recurrence-free survival was 88.0% (95% CI 81.6% to 94.9%) and 5 year overall survival was 95.1% (95% CI 90.5% to 99.9%). In a multivariable analysis, only grade 2 histology had a significantly higher recurrence rate (HR 3.42, 95% CI 1.03 to 11.38; p=0.04). There was no difference in recurrence-free survival (p=0.57) and overall survival (p=0.30) in patients with complete lymphadenectomy. In stage IA/IB, grade 2 there was no benefit of adjuvant chemotherapy (p=0.19), and in stage IA/IB, low grade without complete surgical staging there was no benefit of adjuvant chemotherapy (p=0.16). Twelve patients (9.2%) had recurrence; 3 (25%) were salvageable at recurrence and are alive with no disease.
Conclusions Patients with stage I, low grade endometrioid ovarian cancer have a favorable prognosis, and adjuvant chemotherapy and staging lymphadenectomy did not improve survival.
- ovarian cancer
- gynecologic surgical procedures
Data availability statement
Data are available upon reasonable request.
Statistics from Altmetric.com
HIGHLIGHTS
Stage I low grade endometrioid ovarian cancer has a favorable prognosis with surgery.
There is no survival benefit with adjuvant chemotherapy, regardless of staging lymphadenectomy.
The salvage rate was 25% with surgery, radiation, and/or chemotherapy at recurrence.
INTRODUCTION
Endometrioid is the second most common histologic subtype of epithelial ovarian carcinoma after high-grade serous, representing about 10% of epithelial ovarian cancers.1 Compared with high-grade serous carcinoma, endometrioid is often low grade, presents in younger women, at an earlier stage, and is associated with better overall and disease-free survival.2–4 Current guidelines from the National Comprehensive Cancer Network for endometrioid ovarian cancer recommend: observation for surgically staged, stage IA or IB, grade 1; either observation or chemotherapy for stage IA or IB, grade 2 and stage IC, grade 1; and adjuvant chemotherapy for all grade 3 histology.5
Recommendations for adjuvant chemotherapy are primarily based on two randomized controlled trials in stage I epithelial ovarian cancer.6–8 Complete staging lymphadenectomy of apparent early stage epithelial ovarian cancer has been associated with better prognosis, and the benefit of chemotherapy is highest in early stage patients who did not undergo complete lymphadenectomy.7 8 However, the majority of patients in these larger trials represent high-grade serous histology. Retrospective studies have shown the rate of lymph node metastasis in stage I, grade 1 and 2 endometrioid ovarian cancer was much lower at 0–1.7%.9–12
There is limited evidence regarding the role of complete surgical staging with lymphadenectomy and adjuvant chemotherapy in early stage, especially grade 2, endometrioid ovarian cancer. The objective of this study is to evaluate the effect of surgical staging and adjuvant chemotherapy on survival and patterns of recurrence in stage I, grade 1 and 2 endometrioid ovarian cancer.
METHODS
Patient Selection
This retrospective cohort study included patients with grade 1 and 2 (low grade) endometrioid ovarian cancer treated at two cancer centers from July 2001 to December 2019. All cases included before 2010 had undergone pathology review of hematoxylin-and-eosin stained slides by gynecologic pathologists, and required at least one confirmatory endometrioid feature, including background of endometriosis and/or endometrioid adenofibroma or metaplasia (squamous, mucinous, and/or secretory) in addition to negative WT-1 by immunohistochemistry.13–15 Cases after 2010 were evaluated at initial presentation based on the new 2010 criteria. The Institutional Research Ethics Board at each center approved the study. Our initial study cohort included all endometrioid ovarian cancer cases at the two centers. Exclusion criteria were mixed histology, concurrent endometrial cancer, neoadjuvant chemotherapy, and patients who did not undergo follow-up at our centers.
Data Collection
Clinical and pathologic characteristics including age, stage, grade, p53 and WT-1 immunohistochemistry, surgical staging, adjuvant treatment, history of endometriosis, menopausal status and fertility sparing surgery, date of surgery, recurrence, death, and last follow-up were collected. Complete staging lymphadenectomy was defined as ipsilateral or bilateral pelvic and para-aortic lymph node dissection. Complete surgical staging was defined as complete staging lymphadenectomy and cytology. Location of recurrence, treatment for recurrence and post-treatment follow-up information were collected. The decision for surgical staging and adjuvant treatment was based on the treating physician’s preference in concordance with the institutional protocol. Recurrence was defined based on imaging and/or biopsy. Recurrence-free survival was defined as date of surgery to date of recurrence or censored at last follow-up if no recurrence. Overall survival was defined as date of surgery to date of death (if a patient died) or censored at last follow-up date.
Statistical Analysis
Univariate Cox proportional hazard model of recurrence-free survival and a backward stepwise selection procedure of the multivariable analysis was performed to assess for significant associations with predictive factors for disease recurrence. Hazard ratio (HR) and 95% confidence interval (95% CI) was estimated for each predictive factor in the model, with p<0.05 considered statistically significant. Recurrence-free survival and overall survival were compared by the Kaplan-Meier method and groups were compared with the log rank test. Statistical analysis was computed using (SAS version 9.4, Cary, NC) and R package (v4.0.3). In accordance with the journal’s guidelines, we will provide our data for the reproducibility of this study in other centers if such is requested.
RESULTS
Patient Selection
There were 192 grade 1 and 2 (low grade) endometrioid ovarian cancer cases. At the time of surgical staging, 61 patients (31.8%) were upstaged for pelvic organ involvement (n=47 (24.5%), stage II) or positive omentum/bowel (n=14 (7.3%), stage III). Of those with presumed stage I disease, 79 patients (41.1%) underwent complete or partial lymph node dissection. There were no positive lymph nodes identified, therefore, none of the patients were upstaged due to positive lymph nodes.
Stage IA-C, Low-Grade Patients
There were 131 patients (68.2%) with stage I disease after surgery as shown in Figure 1A. The median follow-up was 51.5 (95% CI 44.3 to 57.2) months. The 5 year recurrence-free survival was 88.0% (95% CI 81.6% to 94.9%) as shown in Figure 2A and the 5 year overall survival was 95.1% (95% CI 90.5% to 99.9%) as shown in Figure 2B.
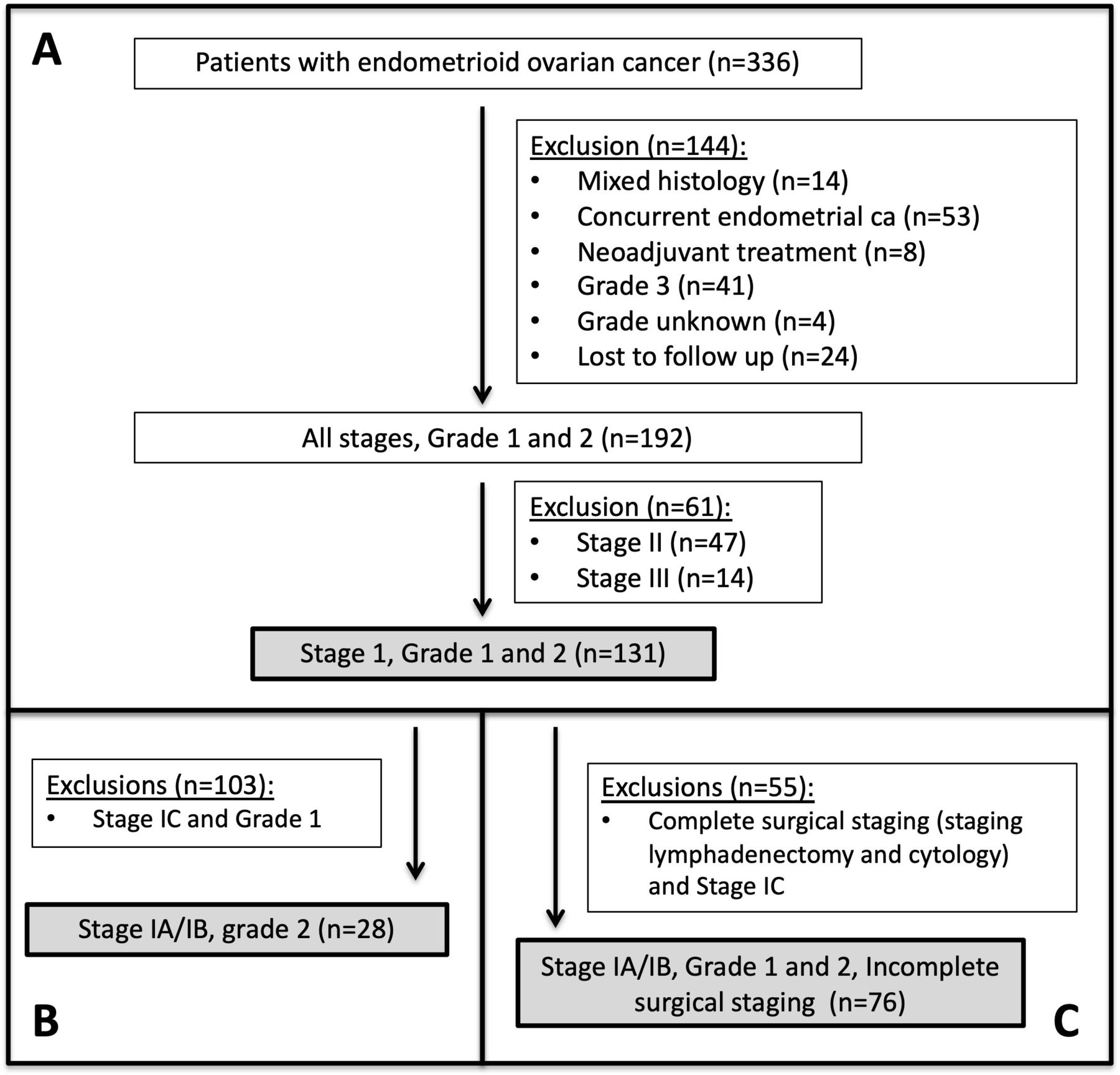
: (A) Flow diagram for cohort selection of stage 1, grades 1 and 2 endometrioid ovarian cancer (n=131). (B) Flow diagram for subgroup analysis of stage IA/IB, grade 2 endometrioid ovarian cancer (n=28). (C) Flow diagram for subgroup analysis of stage IA/IB, grades 1 and 2 patients with incomplete surgical staging of endometrioid ovarian cancer (n=76).

(A) Kaplan-Meier recurrence-free survival (RFS) curve in all patients with stage I disease after surgery (n=131). (B) Kaplan-Meier overall survival (OS) curve in all patients with stage I disease after surgery (n=131).
Table 1 summarizes the clinical and pathological characteristics of patients in the stage I cohort (n=131) with 84 patients (64.1%) stage IA, five patients (3.8%) stage IB, and 42 patients (32.1%) stage IC, with 80 patients (61.1%) having grade 1 and 51 patients (38.9%) having grade 2 histology. Complete staging lymphadenectomy was performed in 34 of 131 patients (26.0%), whereas 97 (74.0%) had either partial (n=22, 16.8%) or no (n=75, 57.2%) lymphadenectomy at surgical staging. Adjuvant chemotherapy was administered to 30 patients (22.9%), 27 patients (20.6%) were treated with carboplatin and paclitaxel, and three patients (2.3%) received single agent carboplatin. Twenty-two patients (16.8%) received six cycles, five patients (3.8%) received three cycles, and three patients (2.3%) received four cycles of chemotherapy. In the univariate analysis shown in Table 1, including age (p=0.15), complete staging lymphadenectomy (p=0.58), and adjuvant chemotherapy (p=0.07), only grade 2 (p=0.04) was a significant risk factor for recurrence with an HR of 3.4 (95% CI 1.03 to 11.4). Although adjuvant chemotherapy approached statistical significance on univariate analysis, the trend was that patients given chemotherapy had a higher risk of recurrence (HR 3.0, 95% CI 0.93 to 2.3). In a multivariable analysis, only grade 2 histology had an increased risk of recurrence (HR 3.42, 95% CI 1.03 to 11.38; p=0.04).
Clinical and pathological characteristics of stage I patients and univariate analysis for risk of recurrence
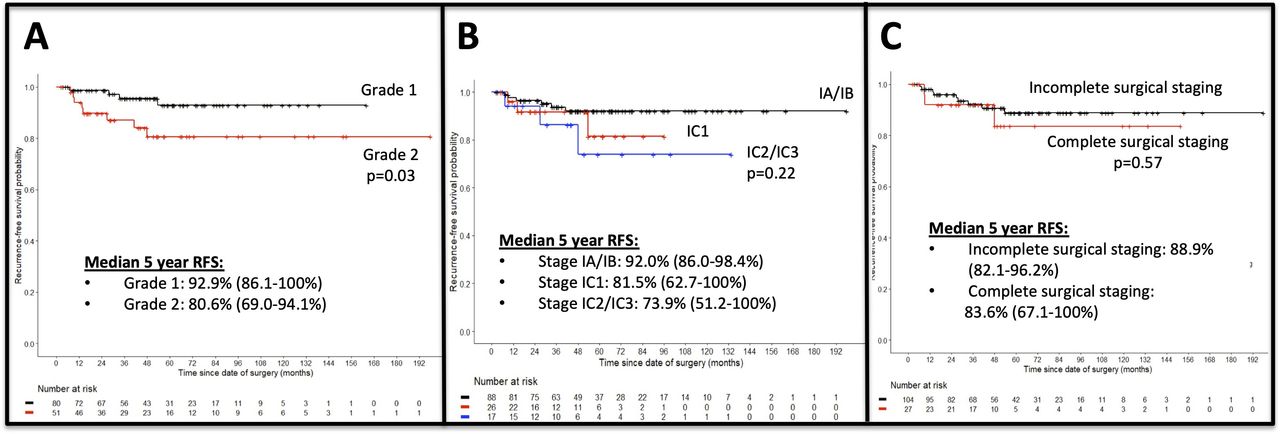
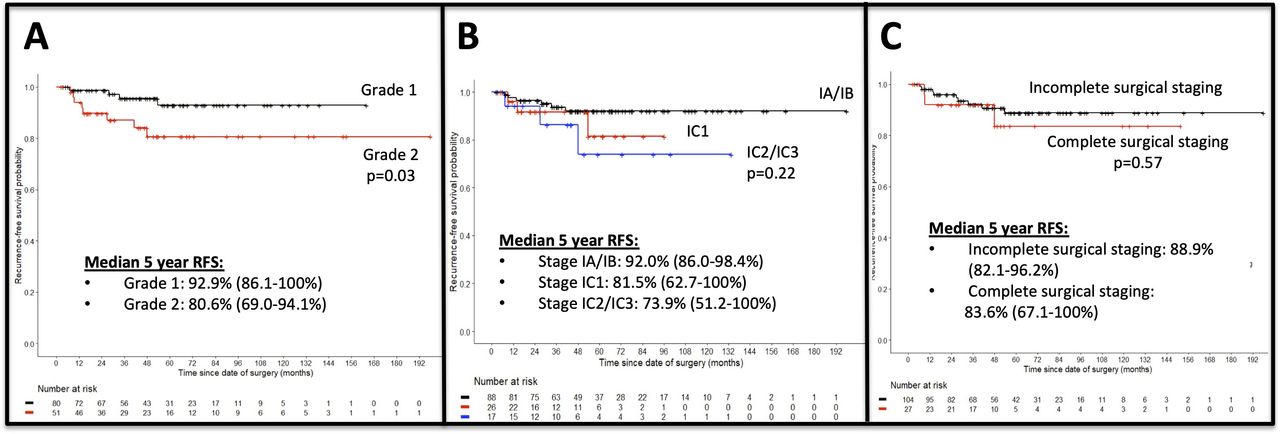
The Kaplan-Meier curve in Figure 3A shows that patients with grade 2 histology are more likely to recur compared with grade 1 patients (p=0.03). For grade 1 patients, the 5 year recurrence-free survival was 92.9% (95% CI 86.1% to 100%) compared with grade 2 at 80.6% (95% CI 69.0% to 94.1%). There was a trend towards improved 5 year recurrence-free survival in patients with stage IA/IB (92.0%, 95% CI 86.0% to 98.4%), compared with stage IC1 (81.5%, 95% CI 62.7% to 100%), and stage IC2/IC3 (73.9%, 95% CI 51.2% to 100%), but this was not statistically significant (p=0.22), as shown in Figure 3B. There was a similar trend in 5 year overall survival in patients with stage IA/IB (96.3%, 95% CI 91.3% to 100%), compared with stage IC1 (92.9%, 95% CI 80.3% to 100%), and stage IC2/IC3 (88.9%, 95% CI 70.6% to 100%), but this was not statistically significant (p=0.7), as shown in online supplemental figure 1. There was no difference in recurrence-free survival (p=0.57) (as shown in Figure 3C) and overall survival (p=0.30) (as shown in online supplemental figure 2) for patients who underwent complete staging lymphadenectomy compared with those who did not.
Supplemental material
Supplemental material
{kind=link}
{kind=link}
{kind=link}
(A) Kaplan-Meier recurrence-free survival (RFS) curve in patients with grade 1 compared with grade 2 histology (n=131). (B) Kaplan-Meier recurrence-free survival curve in patients with stage IA/IB, compared with stage IC1 and stage IC2/IC3 disease. (C) Kaplan-Meier recurrence-free survival curve in patients with complete or incomplete staging lymphadenectomy.
Recurrence
Twelve patients (9.2%) had disease recurrence (Table 2). Eight patients (6.1%) had grade 2 and four patients (3.1%) had grade 1 histology. Four patients (3.1%) with stage 1A recurred, two patients (1.5%) with stage IB, and six patients (4.6%) with stage IC disease recurred. Three patients (25% of patients with recurrence) are alive with no disease after treatment for their recurrence. Of these, one patient had fertility sparing surgery initially, then recurred in the other ovary and is alive with no disease after repeat surgery. The other two patients had a pelvic recurrence, and were treated with surgery, chemotherapy, and one also had radiation treatment. Five patients (41.7% of patients with recurrence) are alive with disease who had pelvic recurrences, with one lymph node recurrence. Four patients (33.3% of patients with recurrence) died of disease, one with stage IA disease initially who was p53 null type. Two of these four recurrences were peritoneal.
Characteristics of patients with recurrence
Stage IA/IB, Grade 2 Patients
A subgroup of 28 patients with stage IA/IB and grade 2 histology were analyzed, as identified in Figure 1B. Ten patients (35.7%) had complete staging lymphadenectomy, three patients (10.7%) had partial lymphadenectomy, and 15 patients (53.6%) did not have a lymph node assessment. Twenty-five patients (89.3%) had stage IA and three patients (10.7%) had stage IB disease, 13 patients (46.4%) had negative cytology, and 15 patients (53.6%) did not have cytology performed at the time of surgery. Seven patients (25.0%) were treated with adjuvant chemotherapy and 21 patients (75.0%) were not. Three patients (10.7%) in this cohort had a disease recurrence. In the univariate analysis shown in online supplemental table 1, there were no significant predictors of recurrence. Specifically, there was no benefit to adjuvant chemotherapy in these grade 2 patients (p=0.19).
Supplemental material
Stage IA/IB, Low Grade Patients with Incomplete Surgical Staging
A subgroup of 76 patients with stage IA/IB, low grade histology who did not have complete surgical staging were analyzed, as identified in Figure 1C. Within this cohort, 10 patients (13.1%) had complete lymphadenectomy without cytology, eight patients (10.5%) had partial lymphadenectomy without cytology, four patients (5.3%) had partial lymphadenectomy with cytology, 30 patients (39.5%) had no lymphadenectomy with cytology, and 24 patients (31.6%) had no lymphadenectomy and no cytology. The majority of patients (n=71, 93.4%) were stage IA and five patients (6.6%) were stage IB. Fifty patients (65.8%) had grade 1 and 26 patients (34.2%) had grade 2 histology. Adjuvant chemotherapy was given to 10 patients (13.1%) (six patients with grade 2 and four patients with grade 1) and 66 patients (86.9%) had no adjuvant treatment. In the univariate analysis shown in online supplemental table 2, stage IB versus stage IA was significantly associated with recurrence (HR 9.9, 95% CI 1.8 to 54.5). Specifically, there was no benefit to adjuvant chemotherapy in this incompletely staged population (p=0.16).
Supplemental material
DISCUSSION
Summary of Main Results
We found that patients with stage I, low-grade endometrioid ovarian cancer have a favorable prognosis with a 5 year recurrence-free survival of 88.0% (95% CI 81.6% to 94.9%) and a 5 year overall survival of 95.1% (95% CI 90.5% to 99.9%). In our cohort of stage I, low grade patients, the only significant predictor of recurrence was grade 2 histology (HR 3.42, 95% CI 1.03 to 11.38; p=0.04). Adjuvant chemotherapy and complete surgical staging with lymphadenectomy did not improve recurrence-free survival. Of the 12 patients with disease recurrence, all recurrences were in the pelvis. Three patients were salvageable at the time of recurrence and are alive with no disease. The one patient with stage IA disease initially who later died of disease was p53 null type, which may suggest a more aggressive subtype of endometrioid ovarian cancer.14
Results in the Context of Published Literature
There are no prospective trials specifically assessing adjuvant chemotherapy in early stage, low grade endometrioid ovarian cancer. Two recently published large retrospective database studies have conflicting results regarding lymphadenectomy and adjuvant chemotherapy for stage 1 endometrioid ovarian cancer. A Surveillance, Epidemiology, and End Results (SEER) study from 2000 to 2013 found no improvement in 5 year overall survival with adjuvant chemotherapy in stage IA/IB/IC, grade 1 and 2 endometrioid ovarian cancer16—findings similar to our study. Another small retrospective cohort study showed no benefit to adjuvant treatment in stage IA/IB, majority grade 1 and 2 endometrioid ovarian cancer.17 In contrast, a National Cancer Data Base study from 2004 to 2014 found a survival benefit with adjuvant chemotherapy for patients with stage IA/IB, grade 2 who did not undergo complete lymphadenectomy. Similar to our study and the SEER study, this study also showed no benefit to adjuvant chemotherapy or lymphadenectomy in stage IA/IB/IC, grade 1 tumors.18
The major limitation of these large database studies in endometrioid ovarian cancer over this time period is that the cases included did not undergo a centralized pathology review. In 2010, the pathologic classification for endometrioid ovarian cancer was revised15 and in subsequent studies several cases that were previously thought to be endometrioid were in fact reclassified to high-grade serous histology.13 It is possible that with pathology review some cases may have been reclassified to high-grade serous histology, as lymph node metastasis in stage I, grade 1 and 2 endometrioid ovarian cancer is 0–1.7%9–12 compared with 5.2–10.7% in serous.11 12 In studies of early stage ovarian cancer, the benefit of chemotherapy is highest in early stage patients with high-grade serous histology who did not undergo complete lymphadenectomy.7 8 19
Strengths and Weaknesses
Our study cohort is one of the largest retrospective studies for this uncommon histology. Given the rarity of this cancer, prospective studies are unlikely to be conducted in this subpopulation, and large retrospective series help guide treatment decisions. All our pathologic specimens prior to 2010 were reviewed with morphology and were WT-1 negative on immunohistochemistry and our study reports recurrent disease with sites of recurrence. Our study limitations include that this was a retrospective study over a long period, as endometrioid ovarian cancer is an uncommon histologic subtype. Surgical staging was not standardized, as some patients had initial surgery with general gynecology and then were referred to gynecologic oncology after pathologic diagnosis, and only a subset of these patients had a second procedure for complete staging. As 47.7% stage IA and IB patients had unknown cytology, this cohort could include a small number of patients with stage IC3. Overall, this cohort had a good prognosis, which may explain why substage was not significant in our analysis. Adjuvant treatment regimens were also not standardized and only a small number of patients received adjuvant chemotherapy; hence, subgroup analysis is limited.
Implications for Practice and Future Research
Our data support the National Comprehensive Cancer Network guidelines that patients with stage IA-C grade 1 endometrioid disease do not benefit from adjuvant chemotherapy. Molecular classification of endometrioid ovarian cancer has shown prognostic significance,14 similar to endometrioid endometrial cancer, and may provide a better risk stratification in the future for adjuvant chemotherapy decisions, particularly for stage I, grade 2 patients.
Conclusions
Patients with stage I, low grade endometrioid ovarian cancer have a favorable prognosis, and staging lymphadenectomy and adjuvant chemotherapy did not improve survival. Recurrences were confined to the pelvis and there was a 25% salvage rate at time of recurrence.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Presented at This work was presented as an Abstract at the Society of Gynecologic Oncology Annual Meeting 2021 and Oral Presentation at the Society of Gynecology Oncology of Canada Annual Meeting 2021.
Contributors BES: data curation, Investigation, methodology, visualization, writing – original draft. AC: conceptualization, visualization, writing – review and editing. VM: investigation, writing – review and editing. CP-H: investigation, writing – Review and editing. MQB: visualization, writing – review and editing. SN-M: investigation. LH: Guarantor, conceptualization, methodology, visualization, writing – review and editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.