Article Text

Abstract
Objective The International Federation of Gynecology and Obstetrics (FIGO) revised the vulvar cancer staging schema in 2021. Previous stage IIIA–B diseases were reclassified based on nodal size (≤5 mm for stage IIIA compared with >5 mm for stage IIIB), and previous stage IVA1 disease based on non-osseous organ extension was reclassified to stage IIIA whereas osseous extension remained as stage IVA. This study sought to validate the 2021 FIGO vulvar cancer staging schema.
Methods This retrospective cohort study examined 889 women with stage III–IV vulvar cancer from 2010 to 2015 in the National Cancer Institute’s Surveillance, Epidemiology, and End Results Program. Stage shift and overall survival were assessed by comparing the 2021 and 2009 FIGO staging schemas.
Results Stage shift occurred in 229 (25.8%) patients (upstaged 17.7% and downstaged 8.1%). When comparing the new and previous staging schemas, 5 year overall survival rates were 45.6% versus 48.9% for stage IIIA, 47.0% versus 44.2% for stage IIIB, and 13.9% versus 25.1% (interval change −11.2%) for stage IVA diseases. According to the revised staging schema, 5 year overall survival rates were similar for stage IVA and IVB diseases (13.9% vs 14.5%) and for stage IIIA and IIIB disease (45.6% vs 47.0%). For new stage IIIA disease, 5 year overall survival rates differed significantly based on the staging factors (nodal involvement vs non-nodal organ involvement, 48.9% vs 38.7%, difference 10.2%, p=0.038).
Conclusion The 2021 FIGO staging schema results in one in four cases of advanced vulvar cancer being reclassified. Survival rates of patients with new stage IVA disease worsened significantly whereas those of patients with new stage IIIA disease were heterogenous based on the staging factors. The discriminatory ability of the revised 2021 FIGO staging schema for 5 year overall survival rate between patients with stage IIIA and IIIB tumors and those with IVA and IVB tumors is limited in this study population.
- vulvar neoplasms
Data availability statement
Data are available in a public, open access repository. All the data that support the findings of this study are publicly available in The National Cancer Institute’s Surveillance, Epidemiology, and End Results Program at http://seer.cancer.gov/.
Statistics from Altmetric.com
HIGHLIGHTS
The stage of one in four advanced diseases was reclassified in the new revision.
Survival rates of patients with new stage IVA disease appear to be comparable to those with stage IVB disease.
Survival rates of patients with new stage IIIA disease are heterogenous based on tumor factors.
Introduction
Vulvar cancer is the fifth most common gynecological malignancy in the United States.1 The population incidence rate of vulvar cancer is approximately 2–2.5 per 100,000, and the incidence has been gradually increasing during the past few years.2 In 2021, 6120 women are expected to be diagnosed with vulvar cancer and 1550 women are estimated to die from the disease in the United States.1 Prognosis of women with vulvar cancer is largely dependent on the stage of the cancer. Women with early disease have a favorable survival outcome whereas those with advanced disease have poor prognosis.2
Historically, cancer staging schemas are predicated on prognostic tumor factors based on local, nodal, and distant tumor information, and the staging schema guides treatment practice and patient counseling.3 4 In October 2021, the International Federation of Gynecology and Obstetrics (FIGO) Committee for Gynecologic Oncology reviewed the recent literature and revised the cancer staging for vulvar cancer.5 The rationale of this revision was to address the inconsistent findings across the studies validating the prognostic performance of the 2009 FIGO staging schema.5 The revised staging guidelines were based on an analysis of data from the National Cancer Database (NCDB) from 2010 to 2017.5 6 According to the Committee, the analysis was used to examine the prognostic performance and simplify the cancer staging schema based on overall survival, which was a new strategy.5 The analysis relied on a number of tumor characteristics including tumor size, depth of invasion, local tumor extension, nodal status, and regional and distant spread and their association with overall survival.5 To date, external validation of these findings has not been performed.
Compared with the 2009 FIGO vulvar cancer staging schema, the 2021 revision has two changes for advanced disease: previous stage IIIA1−2/IIIB1-2 diseases were reclassified based on nodal size (≤5 mm for stage IIIA vs >5 mm for stage IIIB); and prvious stage IVA1 disease based on non-osseous organ extension was reclassified as IIIA disease (Table 1 and Online supplemental table S1).5 7 Given these reclassifications in the revised schema, this study sought to validate the 2021 FIGO vulvar cancer staging schema in a different patient population from the NCDB analysis.
Supplemental material
Reclassification of the staging schema in vulvar cancer
Materials and Methods
This study utilized the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) program for analysis.8 The SEER program is a population-based tumor registry in the United States that collects data on approximately 35% of the current US population and captures 97% of incident cancers within the registry areas.9 This study thus used the SEER program for the validation of 2021 FIGO staging schema due to the population-based data-capturing mechanism. Patient identification, data entry, and rigorous data quality control are managed by the registered trained personnel and the SEER program.10 The SEER program is externally linked to the National Death Index and vital status is updated every year.
In the current analysis of the SEER program, the selection criteria followed a similar fashion as the FIGO Committee on Gynecologic Oncology analysis that used the NCDB data.5 The study population included women aged ≥18 years with stage III–IV vulvar cancer diagnosed from 2010 to 2015. The starting point was chosen due to the 2009 revision in vulvar cancer staging schema.7 The endpoint was chosen to have adequate follow-up by excluding patients diagnosed more recently.
Primary tumor site codes included C51.0, C51.1, C51.2, C51.8, and C51.9. Histological types 8000–8246, 8248–8576, 8940–8950, and 8980–8981 according to the International Classification of Diseases for Oncology, third edition and WHO histological classification were included.11 Exclusion criteria were stage I–II or unknown stage, histology other than given above, lack of survival information, not first cancer diagnosis including secondary primary cancer, and no histopathological confirmation for diagnosis.
The SEER program captures the information for vulva cancer stage via the American Joint Commission on Cancer (AJCC) Tumor-Node-Metastases (TNM) category seventh edition during the study period, and local tumor factor (T), nodal metastasis (N), and distant metastasis (M) are recorded as discrete variables.8 12 According to the National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines, vulvar cancer is staged using the AJCC and FIGO staging systems,4 providing the comprehensive schema of conversion from AJCC TNM staging to FIGO staging (Online supplemental table S2).4 For T3 disease, the Collaborative Stage Extension schema was used to assess the tumor extension. Because the SEER program does not have information on actual size of lymph node metastasis, this study used the defaulted size of ≥5 mm or <5 mm cut-off for analysis (Online supplemental table S2).
The main outcome measures of this study were stage shift and prognostic performance. First, cases that had stage shift from the 2009 FIGO staging schema to the 2021 FIGO staging schema were assessed. Upstaging was defined as the reclassification of cancer stage to a higher group, and downstaging was defined as the cancer stage reclassification to a lower group (Table 1). Stage shift included substage levels (eg, IIIA to IIIB or IIIB to IIIA) in this study as the distinct survival difference was shown in the NCDB analysis.5 Descriptive statistics were performed according to the 2009 FIGO staging schema frequency.
Second, 5 year overall survival rate per cancer stage was assessed. This outcome measure was chosen for external validation because the FIGO Committee analysis of the NCDB database used overall survival as the study endpoint. A shift in the 5 year overall survival percentage rate points was examined. Specifically, 5 year overall survival rates per cancer stage were estimated based on the 2021 FIGO staging schema and compared with the performance in the 2009 FIGO staging schema. The 5 year overall survival percentage rate changes from the previous to the current staging schemas were calculated. Overall survival was defined as the time interval between the vulvar cancer diagnosis and death from any cause (all cause). The Kaplan-Meier method was used to construct the survival curves, and the differences between the curves were assessed with the log-rank test. In addition, vulvar cancer-specific mortality was assessed. This endpoint was chosen as vulvar cancer is a disease of older women (median age at diagnosis 69 years) and non-cancer conditions can be prevalent as the cause of death. Cumulative incidence functions were used to estimate the 5 year vulvar cancer specific mortality rate.
In an exploratory analysis, the discriminatory ability of cancer stage for overall survival was assessed in each schema. This was defined as the absolute difference between the highest and lowest 5 year overall survival percentage rates. In addition, survival rates of women with stage IIIA and IVA disease in the 2021 FIGO staging schema were examined based on the tumor factors within the substage. This analysis was undertaken because these two substages in the new staging schema comprised two distinct tumor sites: nodal involvement or non-nodal organ involvement. In stage IIIA disease, regional lymphatic involvement represented nodal involvement whereas tumor extension to the upper two-thirds of the urethra or vagina, bladder mucosa, or rectal mucosa represented non-nodal organ involvement. In stage IVA disease, fixed or ulcerative regional lymphatic metastasis represented the nodal involvement whereas a local tumor fixed to the pelvic bone represented non-nodal organ involvement. Log-rank tests were used to compare the statistical differences between the survival curves.
All the statistical analyses were based on two-tailed hypotheses and a p-value of less than 0.05 was considered statistically significant. IBM SPSS Statistics version 27.0 (Armonk, New York, USA) and R version 3.5.3 (R Foundation for Statistical Computing, Vienna, Austria) were used for statistical analyses. This study used deidentified, publicly available data and was deemed exempt by the University of Southern California Institutional Review Board.
Results
A total of 889 women with stage III–IV vulvar cancer were examined (Online supplemental figure S1). The median age at diagnosis was 68 years (IQR 57–79 years), and the majority were non-Hispanic White women (n=704, 79.2%).

Overall survival based on the staging schemas. Overall survival is shown for (A) 2009 FIGO staging schema and (B) 2021 FIGO staging schema. Among 294 women who were censored, 158 (53.7%) had ≥5 year follow-up. Metadata for survival statistics are shown in Table 3. FIGO, International Federation of Gynecology and Obstetrics.
The most frequent cancer stage in the 2009 FIGO staging schema was IIIA (n=290, 32.6%) followed by IVB (n=193, 21.7%), IIIC (n=147, 16.5%), IVA (n=139, 15.6%), and IIIB (n=120, 13.5%). In the 2021 FIGO staging schema, the most frequent cancer stage was IIIB (n=268, 30.1%) followed by IIIA (n=205, 23.1%), IVB (n=193, 21.7%), IIIC (n=147, 16.5%), and IVA (n=76, 8.5%).
Stage shift occurred for 229 (25.8%) women between the two cancer staging schemas (upstaged n=157, 170.7%; downstaged n=72, 8.1%; Table 2). For stage IIIA disease in the 2009 FIGO staging schema, 157 (54.1%) of 290 cases were upstaged to stage IIIB disease in the 2021 FIGO staging schema. For stage IIIB disease in the 2009 FIGO staging schema, 9 (7.5%) of 120 cases were downstaged to stage IIIA disease in the 2021 FIGO staging schema. For stage IVA1 disease in the 2009 FIGO staging schema, 63 (45.3%) of 139 cases were downstaged to stage IIIA disease in the 2021 FIGO schema.
Stage shift for the 2021 FIGO staging schema
The median follow-up of censored cases was 5.2 years (IQR 3.8–6.8 years), and 595 (66.9%) women died during the follow-up. The majority of deaths were due to vulvar cancer (71.0%). Among 294 women who were censored, more than half had 5 year or longer follow-up duration in this study (n=158, 53.8%).
Stage-specific survival was compared based on the 2021 and the 2009 FIGO staging schemas (Figure 1 and Table 3). For stage IIIA disease, the 5 year overall survival rate was 45.6% versus 48.9% for the 2021 and 2009 FIGO staging schemas, respectively (interval rate change −3.3 percentage points). For stage IIIB disease, the 5 year overall survival rate was 47.0% versus 44.2% for the 2021 and 2009 FIGO staging schemas, respectively (interval rate change+2.8 percentage points). For stage IVA disease, the 5 year overall survival rate was 13.9% versus 25.1% for the 2021 and 2009 FIGO staging schemas, respectively (interval rate change −11.2 percentage points). Similar trends were observed for vulvar cancer-specific mortality (5 year cumulative rate for stage IVA disease was 60.3% vs 52.4%, interval rate change −7.9 percentage points; Table 3).
Survival statistics according to the staging schemas
Inter-stage survival was then compared according to the 2021 FIGO staging schemas (Figure 1, Table 3, and Online supplemental tables S3 and S4). The 5 year overall survival rates were similar for stage IVA and IVB diseases (13.9% vs 14.5%, p=0.997). In the previous staging schema, stage IVA and IVB disease were distinctly different (5 year overall survival rates 25.1% vs 14.5%; p<0.001). Survival rates for women with stage IVA disease were similar to those with stage IIIC disease in the previous staging schema (25.1% vs 30.3%, p=0.377). In the revised staging schema, 5 year overall survival rates were similar between stage IIIA and IIIB disease (45.6% vs 47.0%, p=0.997). This association was also seen in the previous staging schema (48.9% vs 44.2%, p=0.347).
When the discriminatory ability of overall survival across three cancer stages (IIIA, IIIB, and IVA) was examined (Table 3), the inter-stage difference in the 5 year overall survival rate was 23.8 percentage points (from 25.1% to 48.9%) in the 2009 FIGO staging schema and the rate widened to 31.7 percentage points (from 13.9% to 45.6%) in the 2021 FIGO staging schema (interval rate change 7.9 percentage points).
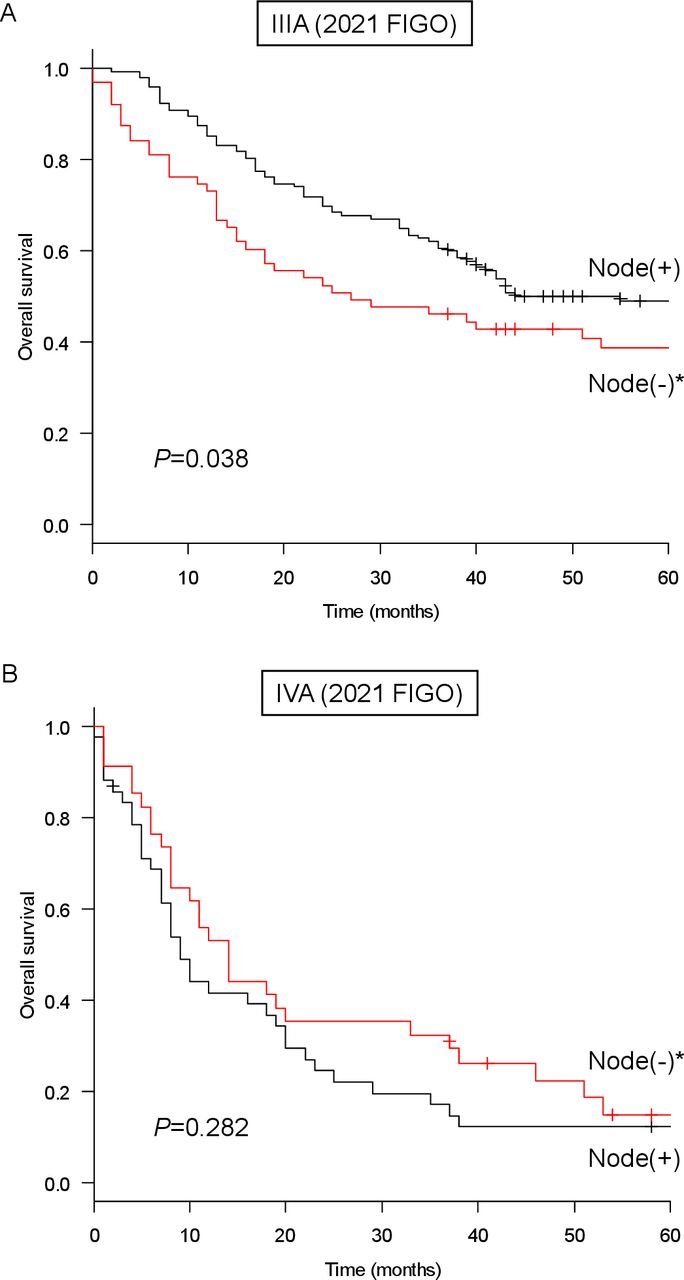
Lastly, by using the 2021 FIGO staging schema, survival outcomes of stage IIIA and IVA diseases were examined based on several pathological factors (nodal involvement vs non-nodal organ involvement; Figure 2). For new stage IIIA disease, the 5 year overall survival rate was 48.9% for women with nodal involvement and 38.7% for those with non-nodal organ involvement (inter-group rate difference 10.2%, p=0.038; Figure 2A). For new stage IVA disease, the 5 year overall survival rates were similar for those with nodal involvement and non-nodal organ involvement (12.2% vs 14.9%, inter-group rate difference 2.7%, p=0.282; Figure 2B).

{kind=link}
{kind=link}
Overall survival based on tumor factors (stage IIIA and IVA). Log-rank test for p value. Overall survival is shown based on the component of (A) stage IIIA disease and (B) stage IVA disease: nodal involvement (blue) or non-nodal organ involvement (red). *Tumor extension to upper-third vagina, bladder mucosa, or rectal mucosa. **Local tumor fixed to the pelvic bone. Node, nodal metastasis.
Discussion
Summary of Main Results
These data reveal several important findings. First, the disease stage of one in four patients with advanced disease was reclassified according to the new staging guidelines. Second, survival rates of women with stage IVA disease in the new staging schema were much poorer than using the 2009 staging schema. Third, survival rates of women with stage IIIA disease according to the new staging schema remain heterogenous with a diverse range of survival rates based on staging tumor factors. Lastly, the revised staging system results in overlapping survival for women with stage IIIA and IIIB tumors.
Results in the Context of Published Literature
In the current revision of the FIGO staging schema, a considerable number of stage III–IV vulvar cancers were reclassified. This included nearly half of the stage IVA cases in the previous staging schema being downstaged to stage IIIA disease in the new staging schema (46.1%). More than half of previous stage IIIA cases were also reclassified to stage IIIB (57.5%). Collectively, the extent of reclassification observed in the 2021 FIGO staging schema clearly implies that this is a major revision in vulvar cancer staging compared with the previous edition.
The cancer stage reclassification in the revised FIGO staging schema occurred in three substages of advanced vulvar cancer (stage IIIA, IIIB, and IVA diseases; Table 1). In the NCDB analysis, the discriminatory ability of 5 year overall survival rates across these three stages were 34.4 percentage points (25.9% to 60.3%).5 In this analysis of SEER program data, the discriminatory ability was similar to their analysis (31.7%, range 13.9% to 45.6%). This external validation is reassuring to confirm the prognostic performance of the newly introduced vulvar cancer staging schema. Moreover, the discriminatory ability of 5 year overall survival rates in these three groups in the current study increased from the previous staging to the new staging schema. This significant improvement in the discriminatory ability of the 2021 FIGO staging schema is clinically meaningful and is noteworthy.
This improved prognostic performance of the 2021 FIGO staging schema is in part due to the reclassification of stage IVA disease (Table 1). Tumor extension to the upper urethra or vaginal mucosa, bladder mucosa, or rectal mucosal invasion has been removed from stage IVA in this new revision, and survival outcomes of the new stage IVA disease worsened and were closer to stage IVB disease (Table 3). The new stage IVA disease has different staging components (nodal involvement and non-nodal organ involvement), but the survival effects appear to be similar for the two factors. However, survival rates of women with new stage IIIA disease are heterogenous and include women with either nodal or non-nodal organ involvement in this revision (Figure 2A). This results in a more than 10 percentage point difference between the two groups that clinicians should bear in mind when counseling patients. Whether this survival difference is also seen in the NCDB analysis merits further investigation.
While the 2021 FIGO staging schema is useful to distinguish survival among IIIA, IIIB, and IVA diseases that the within-staging definition altered from the 2009 FIGO staging schema, the discriminatory ability across advanced stages (IIIA–IVA) in the SEER population was less robust compared with the NCDB study population.5 Specifically, survival rates were similar between women with IIIA and IIIB disease and between those with IVA and IVB disease. In addition, the survival outcome of women in the SEER population was slightly worse compared with the NCDB population examined in the FIGO Committee on Gynecologic Oncology analysis.5 It may be possible that a different study time period resulted in varying 5 year overall survival rates between the two studies (SEER analysis 2010–2015 vs NCDB analysis 2010–2017).5
Strengths and Weaknesses
The strengths of this study included rigorous inclusion and exclusion criteria, use of population-based data, and a recent study period, all of which enhanced the robustness of the study results. Adequate follow-up for survival analysis (median, >5 years) is another strength when interpreting the 5 year overall survival rate. The NCDB analysis included more recent year cases.
Salient limitations of this study include a lack of information on preoperative information (grossly or radiographically abnormal lymph node), some pathological characteristics (eg, actual size and number of lymph node metastases), and information regarding recurrence including nodal recurrence. The accuracy of data in the SEER program is also unknown as an actual medical record review was not performed. The lymph node size cut-off in the 2021 FIGO staging schema is >5 versus ≤5 mm while the cut-off in the 2009 FIGO stating schema was ≥5 versus <5 mm.5 7 This slight difference could not be assessed in this study, and cases with 5 mm of nodal metastasis may have been misclassified in the current analysis. Details about reclassification of the lymph node metastasis size in the NCDB analysis were not provided and this warrants further validation. Information on depth of tumor invasion was not available in the SEER program, and early-stage disease was not assessed in this study. Lastly, the generalizability of the results in other populations is unknown because this study examined the limited geographical and socio-economic population in the United States only.
Implications for Practice and Future Research
In conclusion, the 2021 FIGO staging schema for vulvar cancer has major revisions compared with the previous schema, but overall it is useful to estimate survival of patients with advanced disease. Such information will be valuable in the practice and decision-making process. Simplifying and reducing the staging schema from 11 groups to eight groups in the new classification is also clinically meaningful. Because this SEER analysis did not completely validate the 2021 FIGO staging schema, further study is surely warranted to validate the results of their study. Additionally, distinguishing the nodal and non-nodal components in the staging schema of vulvar cancer could benefit from further discussion.
Data availability statement
Data are available in a public, open access repository. All the data that support the findings of this study are publicly available in The National Cancer Institute’s Surveillance, Epidemiology, and End Results Program at http://seer.cancer.gov/.
Ethics statements
Patient consent for publication
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Conceptualization: KM, MM. Data curation: KM. Formal analysis: KM. Funding acquisition: KM, LDR. Investigation: all authors. Methodology: KM, MK. Project administration: KM. Resources: KM. Software: KM. Supervision: MK, LDR, JDW. Validation: KM. Visualization: KM. Writing - original draft: KM. Writing - review and editing: all authors. Guarantor: KM.
Funding Ensign Endowment for Gynecologic Cancer Research (KM).
Disclaimer The funder had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Competing interests All were outside the work: honorarium, Chugai, textbook editorial expense, Springer, investigator meeting attendance expense, VBL Therapeutics (KM); consultant, Clovis Oncology, research grant, Merck, royalties, UpToDate (JDW); consultant, Quantgene (LDR).
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.