Article Text

Statistics from Altmetric.com
Recurrent ovarian cancer is usually associated with complex pelvic conditions. The variable location of metastatic tumors and intestinal adhesions make secondary cytoreductive surgery difficult. In order to provide appropriate surgery, gynecologic oncologists working in medical centers where many gynecological surgeries are performed are required to be accomplished in urological, vascular, and gastrointestinal surgery. The aim of Video 1 is to introduce minimally invasive surgical techniques used in secondary cytoreductive surgery of recurrent ovarian cancer for gynecologic oncologists. All the procedures demonstrated in this video were performed by gynecologic oncologists.
A 58-year-old woman was diagnosed with peritoneal carcinomatosis. In 2018, she received primary debulking surgery which included laparoscopic hysterectomy, bilateral adnexectomy, pelvic and para-aortic lymphadenectomy, and infragastric omentectomy. The post-operative pathology revealed a high-grade serous adenocarcinoma that was International Federation of Gynecology and Obstetrics (FIGO) stage IIB. She started adjuvant chemotherapy 3 weeks after the surgery for six cycles. A comprehensive evaluation suggested a complete response. However, in February 2020, a positron emission tomography/computed tomography (PET/CT) scan showed tumors on the ileum, sigmoid colon, left pelvic brim, and near the bladder. There were no other tumors in the upper abdomen or extra-abdominal region, so this patient was eligible for secondary cytoreductive surgery. We first placed a stent into the ureter on both sides.1 As the bottom of the tumor was initially hard to expose, we first separated the tumor from the left extreme which densely adhered to the left pelvic brim. Next, we distinguished and cut off the superior rectal arteries and veins and their branches. After that, the ureter and internal iliac vein were separated from the tumor. Finally, we performed the colorectal anastomosis using the double-stapled anastomosis technique.2 The operation lasted about 350 mins. The total intra-operative blood loss was 400 ml. The patient was discharged on the 13th day and did not experience any major post-operative complications. The post-operative pathology proved to be high-grade serous adenocarcinoma of the resected tumor. According to National Comprehensive Cancer Network (NCCN) guidelines, it is recommended that a gynecologic oncologist perform the appropriate surgery.3 In this video, the gynecological oncologists at our hospital demonstrated several common procedures of secondary cytoreductive surgery for recurrent ovarian cancer that usually require the assistance of the urological, vascular, and gastrointestinal departments. We left no residual disease in the abdomen. Follow-up has been for 28 months to date. In conclusion, our video shows that complex secondary cytoreductive surgery performed by gynecologic oncologists using minimally invasive technology is both feasible and safe.
{kind=link}
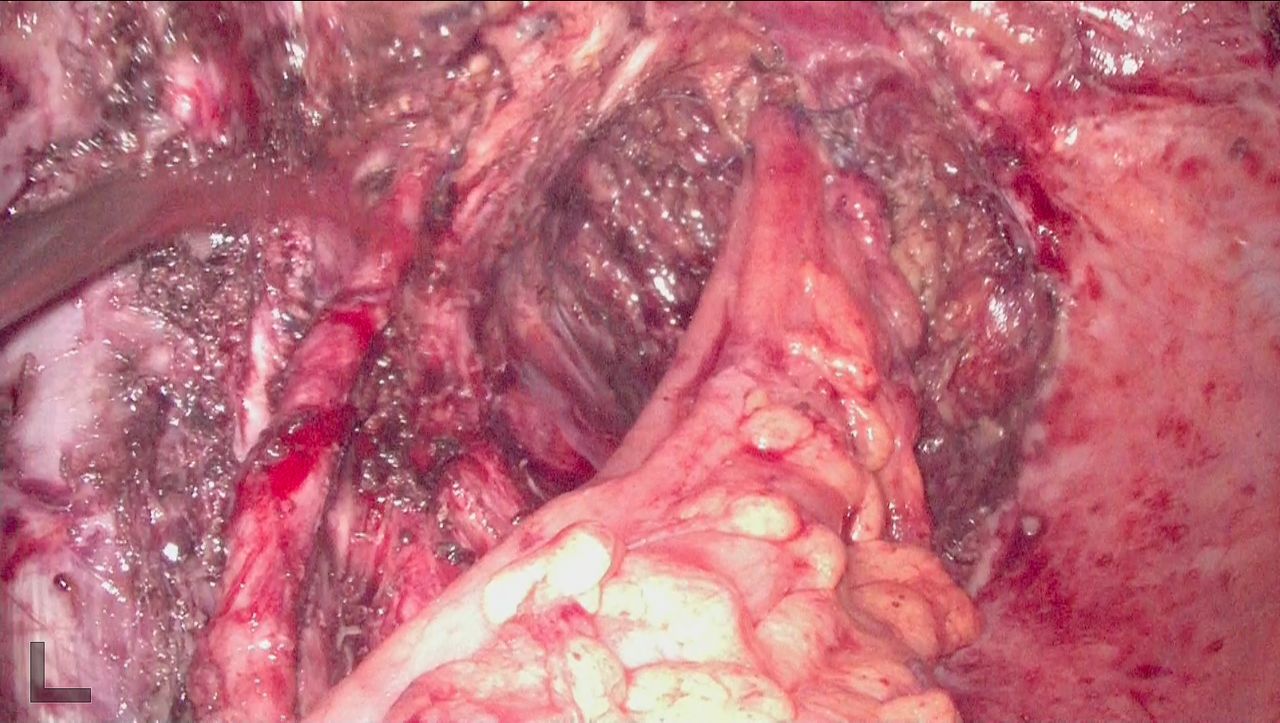
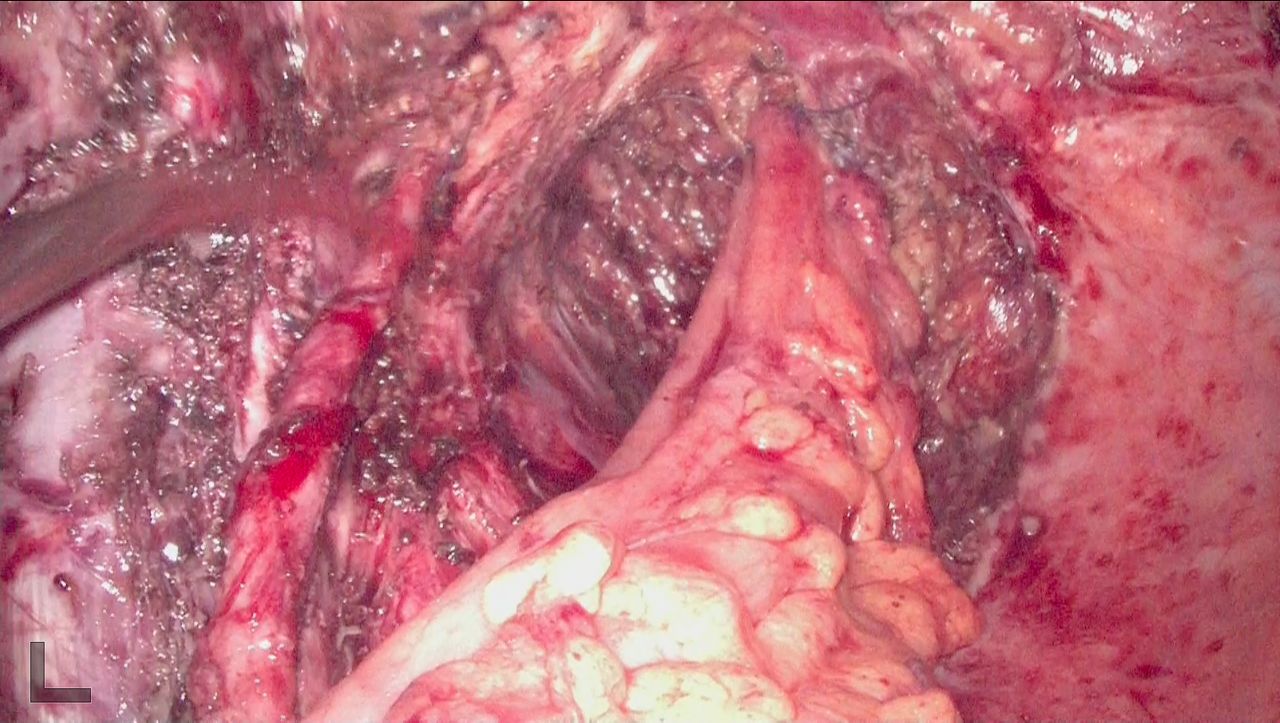
Image showing the overall perspective of the pelvis after removing all the disease within the pelvis. Part of the rectum and sigmoid colon which were infiltrated by metastatic tumor were removed. Colorectal anastomosis was performed using the double-stapled anastomosis technique. The lesion near the ureter, internal iliac vein, and bladder was separated and removed. After the surgery there was no residual disease left in the pelvis.
Data availability statement
All data relevant to the study are included in the article.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants; however, the Ethics Committee of Obstetrics & Gynecology Hospital of Fudan University exempted this study because the resultant article does not contain medical information about an identifiable individual. Participants gave informed consent to participate in the study before taking part.
Footnotes
Contributors QJ wrote and edited the video article. MC reviewed the article and narration. LYu and LYa performed the surgery. LYa is the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.