Article Text

Abstract
Primary mucinous ovarian cancer is a rare type of epithelial ovarian cancer. In this comprehensive review we discuss management recommendations for the treatment of mucinous ovarian cancer. Although most tumors are stage I at diagnosis, 15–20% are advanced stage at diagnosis. Traditionally, patients with primary mucinous ovarian cancer have been treated similarly to those with the more common serous ovarian cancer. However, recent studies have shown that mucinous ovarian cancer is very different from other types of epithelial ovarian cancer. Primary mucinous ovarian cancer is less likely to spread to lymph nodes or the upper abdomen and more likely to affect younger women, who may desire fertility-sparing therapies. Surgical management of mucinous ovarian cancer mirrors surgical management of other types of epithelial ovarian cancer and includes a bilateral salpingo-oophorectomy and total hysterectomy. When staging is indicated, it should include pelvic washing, omentectomy, and peritoneal biopsies; lymph node evaluation should be considered in patients with infiltrative tumors. The appendix should be routinely evaluated intra-operatively, but an appendectomy may be omitted if the appendix appears grossly normal. Fertility preservation can be considered in patients with gross disease confined to one ovary and a normal-appearing contralateral ovary. Patients with recurrent platinum-sensitive disease whose disease distribution suggests a high likelihood of complete gross resection may be candidates for secondary debulking. Primary mucinous ovarian cancer seems to be resistant to standard platinum-and-taxane regimens used frequently for other types of ovarian cancer. Gastrointestinal cancer regimens are another option; these include 5-fluorouracil and oxaliplatin, or capecitabine and oxaliplatin. Data on heated intra-peritoneal chemotherapy (HIPEC) for mucinous ovarian cancer are scarce, but HIPEC may be worth considering. For patients with recurrence or progression on first-line chemotherapy, we advocate enrollment in a clinical trial if one is available. For this reason, it may be beneficial to perform molecular testing in all patients with recurrent or progressive mucinous ovarian cancer.
- Surgery
- Cystadenocarcinoma, Mucinous
- Surgical Procedures, Operative
- Ovarian Neoplasms
Statistics from Altmetric.com
Background
Primary mucinous ovarian cancer is a rare malignancy accounting for <3% of all epithelial ovarian cancers.1 Because of its rarity, primary mucinous ovarian cancer has historically been under-represented in clinical trials for epithelial ovarian cancer, meaning that the evidence base for treatment for primary mucinous ovarian cancer is not strong. What has become clear is that mucinous ovarian cancer is distinct from the more common epithelial ovarian cancer types, such as serous ovarian cancer, in terms of clinical behavior and response to chemotherapy. For example, 83% of patients with primary mucinous ovarian cancer have ovary-confined disease at diagnosis compared with only 4% of patients with serous ovarian cancer.2 Patients with stage I primary mucinous ovarian cancer have a 5-year overall survival rate approaching 90%.3 In contrast, patients with stage II–IV disease have a much worse prognosis than women with metastatic serous ovarian cancer at similar stages treated with similar chemotherapy regimens.4 5
We review surgical and chemotherapy options for women with primary mucinous ovarian cancer and offer recommendations for treating women with this disease.
Evaluation at Diagnosis
Given the rarity of this tumor type, patients with a new diagnosis of mucinous ovarian cancer should have a thorough evaluation to rule out a gastrointestinal primary tumor. In two separate Gynecologic Oncology Group studies, the majority of cases that were initially thought to be mucinous ovarian carcinoma were reclassified as gastrointestinal primary tumors on re-review of the pathologic specimens (55% in Gore et al and 57–63% in Zaino et al).6 7 Although data regarding site of origin are not available from this study, another analysis of the published literature suggested that colorectal primaries are the most common gastrointestinal source, followed by gastric, appendiceal, and pancreatic.8 Thus, review of the specimens by a gynecologic pathologist is critical. Colonoscopy and upper gastrointestinal endoscopy should also be performed to rule out a gastrointestinal primary tumor.
Computed tomography (CT) of the chest, abdomen, and pelvis should be performed for baseline staging, as for other types of ovarian cancer. The tumor markers CA125, carcinoembryonic antigen (CEA), and CA19-9 may all be useful in the diagnosis and surveillance of mucinous ovarian tumors9–13 and should be evaluated at baseline. A ratio of CA125 level to CEA level of >25 to 1 may be indicative of a gynecologic primary tumor, although the positive predictive value is only 82%.14 Unfortunately, mucinous ovarian cancer often is not diagnosed until after surgery, at which time levels of tumor markers may be normal even if they were elevated at baseline.
Pathologic Features
The 2014 World Health Organization classification system separates primary mucinous ovarian cancer into two sub-types: expansile (confluent) and infiltrative. Although available data are limited, a recent review of the literature suggests that 50–60% of reported mucinous ovarian tumors may exhibit infiltrative histology.15 Expansile tumors exhibit confluent glandular growth with little or no intervening stroma and no stromal invasion. These tumors have low metastatic potential and are limited to the ovary in 95% of cases. Furthermore, among patients with the expansile sub-type, <5% of patients with stage I disease have recurrence. In contrast, infiltrative tumors have destructive stromal invasion with haphazard glands and associated desmoplastic stromal reaction. These tumors are more aggressive, and although 75% are stage I at diagnosis, in 15–30% of women with stage I disease they will recur.15 Both expansile and infiltrative mucinous ovarian cancers usually stain diffusely positive for CK7. They may also stain positive for CK20, PAX-8, and/or estrogen receptor, but when they stain positive, the pattern of staining is focal or patchy, not diffuse. This contrasts with the pattern observed in metastatic colorectal carcinoma, which typically stains diffusely positive for CK20 and negative for CK7.16
Tumor size and laterality may be helpful in differentiating primary mucinous ovarian cancer from metastatic disease from a gastrointestinal tumor. If the tumor is unilateral and >10 cm in diameter, the ovary is the primary tumor site in >80% of cases. If the tumor is bilateral and/or <10 cm in diameter, the primary tumor site is in the gastrointestinal tract in >90% of cases.2
Surgical Treatment
Primary Treatment
Surgical management of primary mucinous ovarian cancer largely mirrors surgical management of other types of epithelial ovarian cancer. This typically includes a total hysterectomy, bilateral salpingo-oophorectomy, omentectomy, and removal of any visible tumor metastases with the goal of complete gross resection of disease. When possible, surgery for mucinous ovarian cancer should be performed by gynecologic oncologists. Traditionally, staging and debulking procedures were done via laparotomy. More recently, use of minimally invasive approaches has increased, most commonly in patients with an isolated pelvic mass. When minimally invasive surgery is used, care should be taken to avoid intra-abdominal rupture and spillage, which increases the final disease stage.
Staging Procedures
Even in patients with disease apparently confined to the pelvis, occult peritoneal disease has been described in mucinous ovarian carcinomas.17 At a minimum, staging should include pelvic washings, omentectomy, and peritoneal biopsies. The role of lymphadenectomy is less certain in mucinous ovarian carcinoma than in high-grade serous ovarian carcinoma. Historically, complete pelvic and para-aortic lymphadenectomies were performed. In the 2010s, data were published suggesting that the frequency of lymph node metastasis in mucinous ovarian cancer is very low (0–2%),18–21 and thus lymphadenectomy in patients with grossly normal appearing lymph nodes was frequently omitted. However, new data emerged showing that, although lymph node metastases are rare in expansile mucinous ovarian cancer, lymph node metastases may be present in up to 30% of patients with the infiltrative sub-type.17 22 Thus, in general, lymph node evaluation should be considered in patients with infiltrative tumors. From a practical standpoint, however, it is difficult to determine the sub-type of mucinous ovarian cancer intra-operatively. Frozen section analysis of mucinous ovarian tumors is notoriously difficult, and one study indicated that the final diagnosis (benign vs borderline vs invasive mucinous carcinoma) might differ from the diagnosis rendered on the basis of frozen section evaluation in 10% of cases.23 More realistically, knowledge of the sub-type of mucinous ovarian cancer—infiltrative or expansile—may be more useful when the patient has already undergone unilateral oophorectomy and the decision is being made whether to re-operate for staging purposes.
Further research is needed into strategies for improving intra-operative diagnosis and decision-making, and a staged procedure may ultimately be required if a diagnosis cannot be confirmed intra-operatively during the initial surgical procedure.
Appendectomy
Another intra-operative consideration is whether or not appendectomy should be routinely performed. Previously, routine appendectomy was recommended for any patient with a borderline or invasive mucinous ovarian cancer to ensure that the appendix was not the true primary tumor site. Most recent data suggest, however, that the likelihood of an occult appendiceal primary tumor in a patient with a normal-appearing appendix is of the order of 1% or less.17 24–26 Thus, we recommend that the appendix be routinely evaluated intra-operatively, but an appendectomy may be omitted if the appendix appears grossly normal, particularly if no gross metastatic disease is identified.
Fertility Preservation
In primary mucinous ovarian cancer, as in other types of epithelial ovarian cancer, fertility preservation with unilateral salpingo-oophorectomy can be considered in patients with disease confined to one ovary, who have a normal-appearing contralateral ovary, and who desire future fertility. Given that the median age at diagnosis is lower for patients with mucinous ovarian cancer than for those with other types of epithelial ovarian cancer,27 28 and given the good prognosis for many patients with stage I mucinous ovarian cancer,3 desire for fertility preservation among these patients is not uncommon. Data regarding the safety of fertility preservation are limited, but overall small series have not shown a clear increased risk of recurrence or death with fertility-sparing approaches.28–31 In these small series, some but not all patients had surgical staging with biopsies, omentectomy, and/or lymphadenectomy, which also makes these data more difficult to interpret. Median age at diagnosis for patients included in these studies was largely in the late 20s. Given the limitations of available data, patients should be carefully counseled about the theoretical increased risk of recurrence,28 particularly in the case of infiltrative disease.31 However, overall for surgically staged patients desiring fertility preservation, fertility-sparing surgeries could be considered.
Treatment of Recurrent Disease
Data regarding surgical interventions for recurrent mucinous ovarian carcinoma are largely extrapolated from other types of epithelial ovarian cancer. Several recent trials suggested that secondary debulking may be beneficial for patients in whom the likelihood of achieving a complete gross resection is high,32 33 although notably one study that included bevacizumab did not show any survival benefit for secondary debulking.34 It is worth noting, however, that very few patients with mucinous ovarian cancer were included in these studies. In general, though, patients with platinum-sensitive disease whose disease distribution suggests a high likelihood of complete gross resection may be candidates for secondary debulking. Furthermore, given the poor rates of response to systemic treatment (discussed below), we believe secondary cytoreduction may prove to be more beneficial in patients with mucinous ovarian cancer than in patients with other types of epithelial ovarian cancer.
Systemic treatment
Primary Treatment
Historically, patients with mucinous ovarian cancer were included in large practice-changing trials of systemic treatment for other types of epithelial ovarian cancer. For this reason, until recently, standard first-line adjuvant systemic treatment for patients with mucinous ovarian cancer included the doublet of carboplatin and paclitaxel, with consideration of adding bevacizumab for patients with advanced disease. However, given the rarity of this histologic type, patients with mucinous ovarian cancer frequently accounted for only 7% or fewer of the patients in these large trials.12 35–39 Additionally, mucinous ovarian cancer behaves markedly differently from high-grade serous ovarian cancer,7 the type that is most widely represented in these studies. Thus, it is uncertain whether results from these landmark trials can truly be extrapolated to patients with mucinous ovarian cancer.
The poorer prognosis seen with mucinous ovarian cancer relative to high-grade serous ovarian cancer is thought to be due at least in part to the lower degree of platinum sensitivity of mucinous ovarian cancer. Platinum sensitivity data are largely based on retrospective studies. One such study, a case–control study that included 27 patients with advanced mucinous ovarian cancer, showed a response rate of 26% for these patients compared with 65% in patients with other types of epithelial ovarian cancer (the control group).4 A second retrospective study found that the response rate to first-line platinum-based chemotherapy was 39% for patients with advanced-stage mucinous ovarian cancer compared with 70% for patients with serous ovarian cancer.40 In a third small study of 21 patients with newly diagnosed mucinous ovarian cancer, only 32% of evaluable patients had a complete response to first-line platinum-based chemotherapy and an additional 11% had a partial response; 47% had disease progression.10
Given these poor response rates and the histologic similarity between primary mucinous ovarian tumors and mucinous tumors of the gastrointestinal tract, the hypothesis arose that mucinous ovarian tumors may respond better to gastrointestinal chemotherapy regimens. On the basis of pre-clinical data supporting this hypothesis,41 a phase II trial comparing a gastrointestinal cancer regimen with a traditional gynecologic cancer regimen in patients with mucinous ovarian cancer was implemented. Gynecologic Oncology Group trial 241/mEOC randomized patients to one of four arms: capecitabine and oxaliplatin; capecitabine, oxaliplatin, and bevacizumab; carboplatin and paclitaxel; or carboplatin, paclitaxel, and bevacizumab.6 The planned accrual was 330 patients, and enrollment occurred in both the USA and the UK. Unfortunately, the study closed early, in large part because of poor accrual. This highlights one of the major barriers to clinical trials of rare tumor types: accrual is very difficult and frequently requires many years of enrollment even when the trial is open nationwide or internationally. On analyses of the enrolled patients, the investigators also identified a second significant issue: 55% of the patients were found to have a non-gynecologic primary mucinous tumor on central pathology review.6 This finding limited the conclusions that could be drawn. However, the data that were available suggested that gastrointestinal cancer regimens were not worse than gynecologic cancer regimens, even when the analysis was limited to the sub-set of patients in whom an ovarian primary tumor was confirmed.
Following these results, the results from two other retrospective studies were published. The first was a descriptive study of 21 patients who received adjuvant chemotherapy with either a gastrointestinal cancer regimen (n=9) or a gynecologic cancer regimen (n=12).42 No difference was seen between the two regimens but, of note, the stage distributions for the two regimens were unbalanced with those receiving the gastrointestinal cancer regimen having more advanced disease. The second study, a retrospective cohort study from two tertiary referral centers, evaluated the use of gynecologic cancer (n=26) and gastrointestinal cancer regimens (n=26) as first-line treatment for patients with mucinous ovarian cancer. The results of this second study demonstrated a significant improvement in overall survival for patients who received gastrointestinal cancer regimens, primarily 5-fluorouracil and oxaliplatin or capecitabine and oxaliplatin, with or without bevacizumab.43 On the basis of these limited data, as well as the overall biological rationale and the poor outcomes seen for patients with advanced mucinous ovarian cancer, the National Comprehensive Cancer Network (NCCN) has updated their recommendations for first-line treatment for mucinous ovarian cancer to include 5-fluorouracil and oxaliplatin, capecitabine and oxaliplatin, and carboplatin and paclitaxel.44
Recommendations for which patients with mucinous ovarian cancer would benefit most from adjuvant treatment are varied. Most organizations agree that patients with stage II, III, or IV disease should receive adjuvant treatment. In general, outcomes for this group of patients remain poor.28 The use of adjuvant treatment was supported by a recent database study of patients with stages II–IV mucinous ovarian cancer that showed an improvement in overall survival for those who received chemotherapy.45 However, recommendations for patients with stage I disease are mixed. NCCN recommends that patients with stage IC disease receive adjuvant chemotherapy and that those with stage IA or IB disease do not, regardless of other histologic findings.44 In contrast, the European Society for Medical Oncology (ESMO) guidelines recommend that treatment decisions for stage I disease be based at least in part on the histologic sub-type, as infiltrative tumors tend to behave more aggressively than expansile tumors.46 The ESMO guidelines recommend against adjuvant chemotherapy for patients with stage IA expansile, grade 1–2 tumors. For all other sub-groups of patients with stage I disease, the ESMO guidelines either state that chemotherapy should be considered (for patients with stage IA infiltrative tumors or stage IB or IC expansile tumors) or state that chemotherapy is recommended (for patients with stage IB or IC infiltrative tumors). A recent study from the National Cancer Database found no improvement in overall survival for patients with stage I disease who received adjuvant chemotherapy.3 However, in that report, the authors provided no information about histologic sub-groups. A different study from the National Cancer Database attempted to further characterize patients with stage I disease into higher- and lower-risk groups, but notably also did not include information about infiltrative or expansile histology.47 The differences in recommendations regarding adjuvant chemotherapy for primary mucinous ovarian cancer reflect the limited data that are available and highlight an area where further investigation would be beneficial. Incorporating these findings, we would recommend erring on the side of complete staging for patients with clinical stage I mucinous ovarian cancer with infiltrative histology. Our proposed approach is outlined in Figure 1.

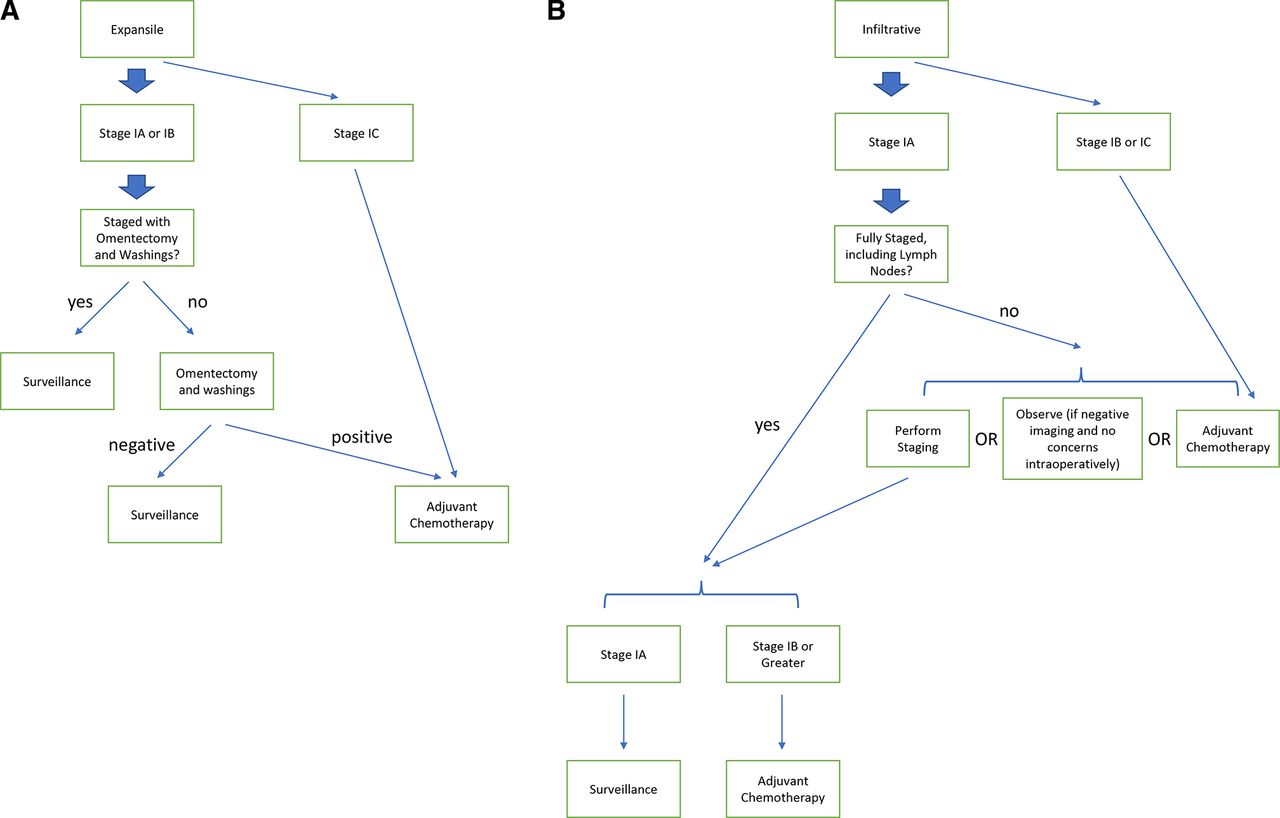{kind=link}
Treatment algorithm for stage I mucinous ovarian cancer tumors with (A) expansile or (B) infiltrative sub-types.
Neoadjuvant chemotherapy might be appropriate for certain patients with advanced stage mucinous ovarian cancer, with patient selection for treatment based on algorithms for other types of ovarian cancer44; however, neoadjuvant chemotherapy for mucinous ovarian cancer remains understudied. Within the three largest trials of neoadjuvant chemotherapy for ovarian cancer, no more than 3% of patients had a diagnosis of mucinous ovarian cancer.48–50 Therefore, the safety and efficacy of neoadjuvant chemotherapy with interval debulking surgeries in patients with mucinous ovarian cancer remain unknown. Furthermore, it is uncertain whether traditional gynecologic cancer regimens should be used, or whether these patients would benefit from gastrointestinal cancer regimens, as discussed above. A final consideration is that diagnosing the primary tumor site for mucinous tumors may be more difficult with a core biopsy and limited tissue than when the entire ovary can be examined. Thus, in cases of metastatic mucinous disease in which the primary tumor site of origin is not clear, we recommend review in collaboration with a gastrointestinal oncology team. However, outcomes for metastatic mucinous carcinoma, regardless of whether it arises from a gynecologic or gastrointestinal primary tumor, are overall poor.7
Heated Intraperitoneal Chemotherapy (HIPEC)
Whether or not heated intraperitoneal chemotherapy (HIPEC) may be beneficial for patients with epithelial ovarian cancer has been increasingly discussed. A study by van Driel et al in the Netherlands showed a recurrence-free and overall survival benefit from HIPEC at the time of interval debulking for patients with stage III epithelial ovarian cancer.51 In contrast, a phase II trial at the Memorial Sloan Kettering Cancer Center in the USA, which evaluated the use of HIPEC for recurrent platinum-sensitive high-grade serous ovarian cancer, did not find a benefit.52 The utility of HIPEC for recurrent high-grade serous ovarian cancer therefore remains uncertain.
Data on the use of HIPEC in patients with mucinous ovarian cancer are currently limited. Notably, the study by van Driel et al cited above included only three patients with mucinous ovarian cancer among a total of 245 patients enrolled.51 Despite these limited data, there remains substantial interest in the use of HIPEC in patients with mucinous ovarian cancer because of the disease’s similarity to gastrointestinal tumors, in which HIPEC is often used to treat carcinomatosis.53 The Peritoneal Surface Oncology Group International and BIG-RENAPE working groups in France published their experience with the use of HIPEC in rare ovarian tumors. They found a particular benefit in patients with mucinous ovarian cancer; in this group, neither the median progression-free survival nor the median overall survival had been reached by 5 years (n=77).54 Patients with mucinous ovarian cancer in this study had perfusion with either mitomycin C or oxaliplatin, which is the working groups’ standard treatment for appendiceal tumors.55 In contrast, all patients in the study by van Driel et al had perfusion with cisplatin.51
A group from China published their experience with patients diagnosed with pseudomyxoma peritonei secondary to mucinous ovarian cancer.56 Over a 10-year period they performed cytoreduction and HIPEC in 22 patients. Similar to van Driel et al, this group used cisplatin for perfusion. Patients with low-grade mucinous cancers and those with lower peritoneal cancer index scores had improved overall survival. Notably, median overall survival times were shorter than 40 months for the entire cohort of patients with pseudomyxoma peritonei due to mucinous ovarian cancer in this study.56
Much remains unanswered about the role of HIPEC in mucinous ovarian cancer. Additionally, recent data about the use of HIPEC in colorectal cancer did not show the benefits anticipated,57 implying that there is still much to be understood about HIPEC in general. However, given the rarity of mucinous ovarian cancer and the lack of effective systemic treatment options, HIPEC may be worth considering. Whether HIPEC is best given at the time of initial diagnosis, as a second staging surgery following the initial diagnosis in the up-front setting, or at the time of secondary debulking is not clear. Given that that vast majority of mucinous ovarian cancers are stage I at diagnosis and do not recur, it is likely that primary treatment with HIPEC for all patients with newly diagnosed mucinous ovarian cancer would result in overtreatment in a substantial proportion of patients. Thus, it may make most sense to preserve HIPEC for tumors associated with highest risk: those that are metastatic at diagnosis or those that have already recurred. We hope that future trials will better delineate the optimal use of HIPEC in patients with mucinous ovarian cancer.
Treatment of Recurrent and Progressive Disease
Data on second-line systemic treatment for mucinous ovarian cancer are even more limited than data on first-line systemic treatment. A retrospective study evaluated 20 patients with mucinous ovarian cancer who had a recurrence at least 6 months after their initial treatment.9 Although the number of patients in this study was small, several patients treated with platinum as second-line chemotherapy had a response. No patient treated with non-platinum agents as second-line chemotherapy had a response. Among patients treated with third- or fourth-line chemotherapy, one patient had a response to paclitaxel, topotecan, and cyclophosphamide as third-line treatment, and one patient had a response to this regimen as fourth-line treatment, but no responses were seen to gemcitabine or liposomal doxorubicin.9 Another small study found that none of the 12 patients treated in second line or beyond with cytotoxic chemotherapy had a complete response, and only one and two patients had partial and complete responses, respectively, to second-line treatment. The remaining eight patients in the second-line setting and six patients in the third-line setting all had progression of disease.10
Bevacizumab may also be beneficial for treatment of recurrent or progressive disease. One case report described a patient with recurrence after adjuvant carboplatin and paclitaxel followed by several standard single-agent regimens for platinum-resistant disease. She was treated with weekly paclitaxel with bevacizumab for six cycles, followed by maintenance bevacizumab for 32 cycles, and she had a durable response to treatment (stable disease).58 Another case report described durable disease stabilization of a borderline mucinous ovarian tumor with single-agent bevacizumab.59
In general, responses to standard-of-care chemotherapy at the time of recurrence or progression of mucinous ovarian cancer are relatively poor. Other regimens for platinum-resistant ovarian cancer listed in the NCCN guidelines should be considered. For patients who received combinations of platinum agents and taxanes for adjuvant treatment, there may be benefit to attempting a gastrointestinal cancer regimen such as capecitabine and oxaliplatin or 5-fluorouracil and oxaliplatin. However, given the poor outcomes described above, even for patients who previously received gastrointestinal cancer regimens, it may also be beneficial to extrapolate from data on mucinous gastrointestinal tumors and consider second-line gastrointestinal cancer regimens, particularly in patients whose functional status remains good after receipt of multiple other lines of treatment. Further data are needed to explore the question of whether the sequence of regimens matters and which second-line regimens are most likely to be successful.
Molecular Characterization and Novel Agents
Given the poor response of mucinous ovarian cancer to cytotoxic chemotherapy, there is much interest in further exploring novel agents for this rare tumor type. Large molecular studies have shown that mucinous ovarian cancers often have aberrations in TP53 (57–90%), KRAS (44–79%), and CDKN2A (11–19%).60–64 Her2 positivity or ERBB2 amplification has also been demonstrated in 18–27% of mucinous ovarian cancers.62 63 65 66
Mismatch repair deficiency has been reported in mucinous ovarian cancer, although it is a rare event.60 67 Thus, the tumor-type agnostic approval of pembrolizumab for patients with tumors demonstrating mismatch repair deficiency or high microsatellite instability68 69 provides another viable option for treatment of recurrent disease. Homologous recombination deficiency, which is present in up to 50% of high-grade serous ovarian cancers,70 is rare in mucinous ovarian tumors.67
Her2 positivity may be targetable given its prevalence described above, although data about treatment options for Her2-positive disease are limited. Extrapolating from other tumor types, it may be possible to combine Her2-targeting treatment with standard-of-care chemotherapy (trastuzumab plus carboplatin and paclitaxel71) or to give Her2-targeting treatment as a single agent. Additionally, the combination of trastuzumab and pertuzumab is currently being explored in other tumor types with Her2 positivity,72 73 and while this combination has not been evaluated in mucinous ovarian cancer, it may represent an avenue for future exploration.
Estrogen and progesterone receptor positivity has also been reported in a sub-set of patients with mucinous ovarian cancer in one study,67 74 and thus anti-hormonal agents could be considered for selected patients. Novel agents targeting the Ras pathway are currently in use for other tumor types and may be a promising avenue in the future. Epidermal growth factor receptor (EGFR) inhibitors have also been proposed,75 and other new treatments are being explored in pre-clinical studies.76–80 While data are lacking for many of these novel agents, we hope that patients with mucinous ovarian cancers will be enrolled in future basket trials of these targeted therapies as it is unlikely that a biomarker-driven, tumor type-specific trial of treatment for this rare histologic sub-type could achieve adequate accrual. If a patient has recurrence or progression on first-line chemotherapy, we would advocate enrollment in a clinical trial if one is available. For this reason, it may be beneficial to perform molecular testing, including next-generation sequencing, mismatch repair deficiency, and Her2 testing, in all patients with recurrent or progressive mucinous ovarian cancer.
Conclusions
Metastatic mucinous ovarian cancer is a rare but aggressive type of epithelial ovarian cancer. Given its rarity, large prospective studies of treatment for this disease have been difficult. This review summarizes the available data and highlights areas that warrant future investigation. Many patients are diagnosed at an early stage and outcomes in this setting are better; however, identifying the ideal algorithms for patients with early-stage infiltrative disease has been difficult. Similarly, surgical management may need to differ depending on histologic findings, so developing ways that details about the histologic sub-type can be available at the time of a surgical staging procedure could be important. Although systemic treatment is recommended for all patients with metastatic mucinous ovarian cancer, data are still limited on whether a traditional gynecologic regimen is sufficient or whether a gastrointestinal regimen may be beneficial. Fully defining the role of HIPEC and knowledge about which second-line regimens are most effective have also remained elusive. New therapies and updated treatment algorithms are sorely needed, and we may need to rely on novel clinical trial designs and basket trial approaches in order to obtain the data we need to move the field forward for this sub-set of patients.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Footnotes
Twitter @frumovitz
Contributors KK: concept development, literature search, writing, revisions, guarantor. MF: concept development, literature search, writing, revisions.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.