Article Text

Statistics from Altmetric.com
Case presentation
A 40-year-old woman with a history of uterine atypical hyperplasia in 2010 was treated with oral progestins for 6 months with complete response. She had no further follow-up until March 2018 when she was referred to the British Hospital of Buenos Aires because during in vitro fertility treatment she was found to have a relapse of atypical endometrial hyperplasia. In 2018 a new fertility preservation attempt was done and an intra-uterine device (Mirena) was used until June 2019. At that point the patient had a complete pathologic response and the intra-uterine device was removed in order to proceed with fertility treatment. An evaluation every 3 months was planned in case she did not get pregnant. In 2020, because of the COVID-19 pandemic, the patient did not have any fertility treatment or follow-up. She returned in January 2021, referred by the fertility clinic, requesting endometrial sampling before starting the in vitro fertilization treatment and hysteroscopic-guided biopsy was performed.
Dr Toscano
We received fragments of endometrial mucosa that focally exhibit an irregular proliferation of back-to-back glands, with epithelial pseudostratification with atypia, consistent with atypical hyperplasia ( Figure 1 ).
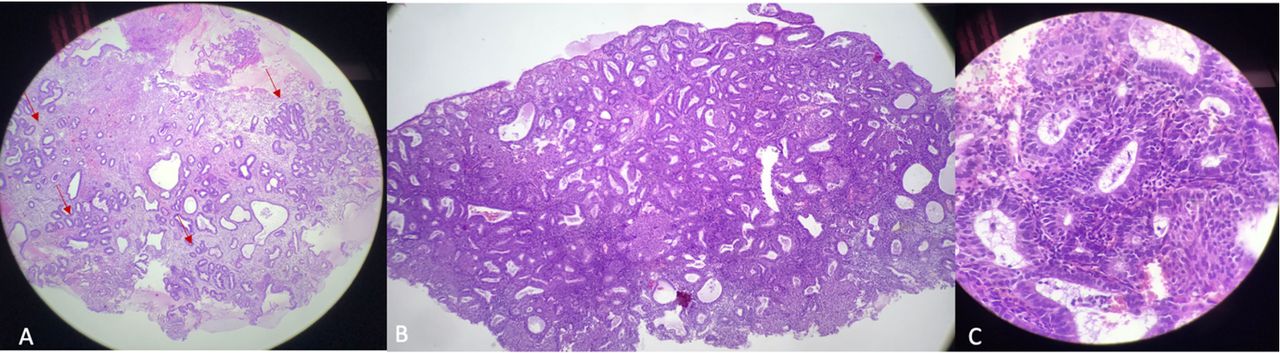
(A) Normal endometrial tissue focally bordering on irregular proliferation of glands (red arrows) (hematoxylin and eosin x10). (B) Closely packed irregular glands with minimal stroma, focally confluent (hematoxylin and eosin x10). (C) Irregular luminal contours with nuclear atypia (hematoxylin and eosin x40).
Dr Chae-Kim: What are the options for management for patients with atypical endometrial hyperplasia who desire fertility preservation?
For women with atypical endometrial hyperplasia or early-stage endometrial cancer, fertility-sparing treatment with oral progesterone or an intra-uterine device has been widely studied. These options are also recommended in the National Comprehensive Cancer Network (NCCN) guidelines for fertility-sparing management of endometrial cancer. Criteria for considering fertility-sparing therapy include: (1) well-differentiated or grade 1 endometrioid adenocarcinoma, (2) disease limited to the endometrium on imaging, (3) absence of suspicious or metastatic disease on imaging, and (4) no contra-indications to medical therapy or pregnancy. 1 For patients who meet these criteria, recommended treatment options include megestrol, medroxyprogesterone, or progestin intra-uterine device, in addition to lifestyle modifications and weight loss. Both routes of progesterone administration, either systemic or local, have been shown to be associated with good disease response outcomes, although some women are unable to tolerate the adverse effects of systemic therapy. Furthermore, recent research suggests that an intra-uterine device may be more effective when combined with metformin dual therapy. 2 A combined or multimodal approach to fertility-sparing therapy has been an evolving area of new research. Studies have reported favorable outcomes after combined therapy such as hysteroscopic resection, aromatase inhibitors such as letrozole, gonadotropin-releasing hormone analogs such as leuprolide, metformin, combined oral contraceptive pills, tamoxifen, and everolimus, among others. 3 4
Dr Chae-Kim: What option for management would you discuss with the patient at this point considering it is her second relapse?
Unfortunately, disease relapse as experienced by this patient can be seen in nearly 40% of cases. According to NCCN guidelines, if endometrial cancer is present at 6–12 months after therapy, total hysterectomy and bilateral salpingo-oophorectomy with staging is recommended. Some patients, however, may continue to desire fertility preservation. Research on outcomes after re-treatment is limited, although encouraging. In one early study which evaluated 33 patients who experienced disease recurrence after initial remission, re-treatment with progestin (medroxyprogesterone acetate or megestrol acetate) was associated with a complete response rate of 85%. 5 More recent studies have reported complete response rates of above 90%. A recent study examined outcomes for 25 patients who received re-treatment with medroxyprogesterone acetate, megestrol acetate, or combined oral progestin with levonorgestrel intra-uterine device or gonadotropin-releasing hormone agonist; 84% of patients achieved complete remission and nearly two-thirds of this group later had a successful pregnancy. Interestingly, 40% of patients who experienced complete remission after re-treatment later developed re-recurrence, and three patients received a third cycle of fertility-sparing treatment. Two of the three patients again experienced complete response. Of note, the time from the initial complete response to recurrence was shorter than the time from the second complete response to re-recurrence. 6
Dr Bambaci
The pelvic magnetic resonance showed a 75×37×54 mm anteverted uterus with heterogeneous endometrium with a thicker area of 10 mm at the uterine fundus. Nabothian cysts were noted in the cervix. The right ovary presents multiple follicular cysts that are hyperintense in T2. There was no evidence of peritoneal, distant disease or lymph node metastases ( Figure 2 ).

Pelvic magnetic resonance image T2 high resolution, sagittal anteverted uterus with homogeneous endometrium 9.9 mm thick. Nabothian cysts in cervix.
At this point the patient decided to proceed with fertility-sparing treatment. While she waited for her insurance to provide the intra-uterine device, she was started on norethisterone 10 mg/daily. Three months later, when she received the intra-uterine device, a hysteroscopy with endometrial biopsy was performed and the Mirena device was inserted during the procedure. At this time the biopsy showed endometrioid adenocarcinoma grade 1.
Dr Toscano
In only two of the endometrial fragments evaluated was a well-differentiated glandular neoplasm endometrioid variant found (endometrioid adenocarcinoma G1), with architectural complexity including glandular confluency and cribiforming, the presence of epithelial stratification and mild nuclear atypia. This finding was observed in focus of 2.2 and 2.4 mm. The remaining fragments corresponded to typical glandular hyperplasia (3 mm), atypical glandular hyperplasia (1 mm), and normal mucosa ( Figure 3 ).
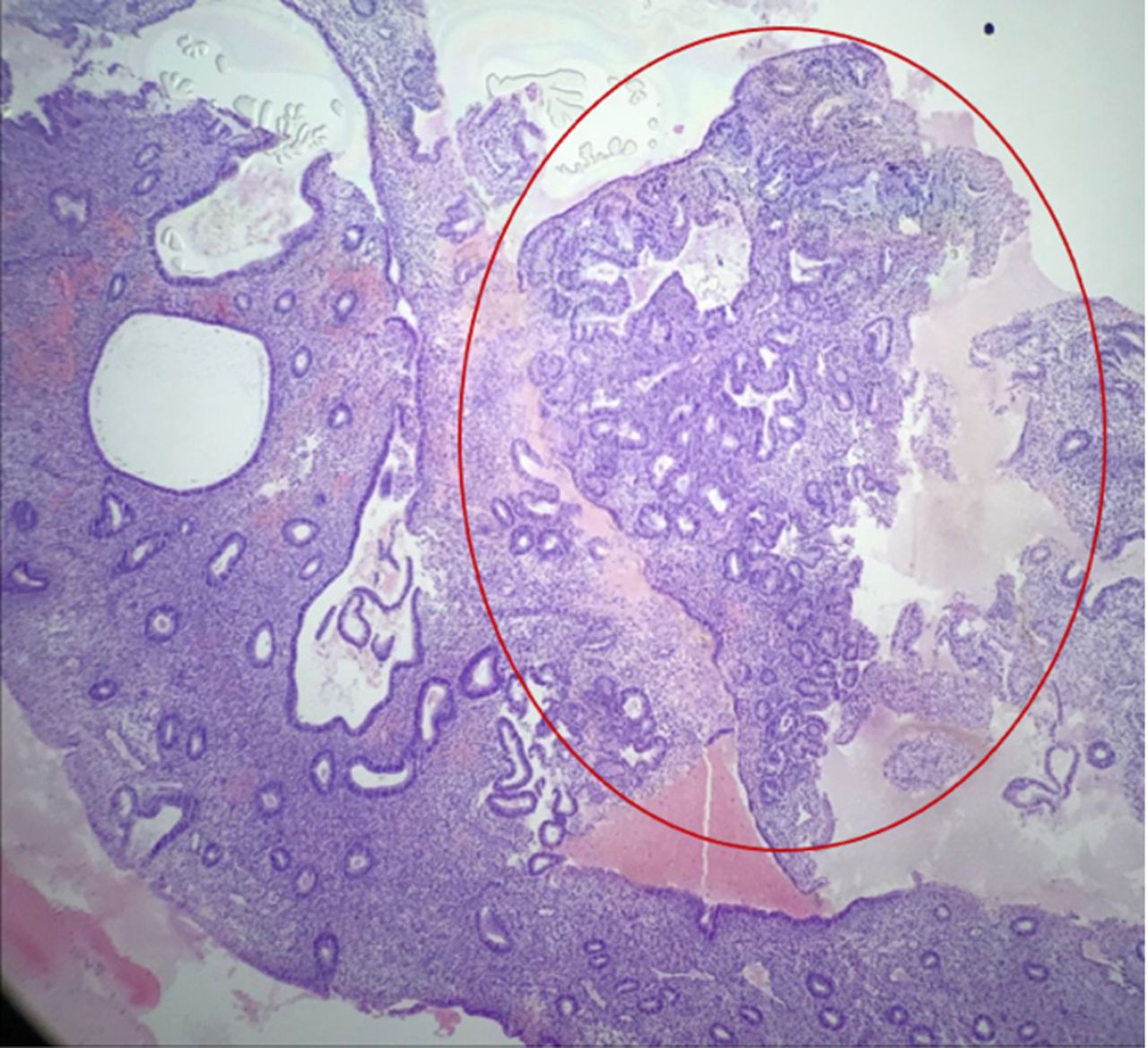
Well-differentiated glandular neoplasm endometrioid variant (endometrioid adenocarcinoma G1) (marked in red) in the context of glandular hyperplasia. Hematoxylin and eosin ×10.
Dr Chae-Kim
The patient’s clinical course spans several years and is characterized by relapse as well as disease progression. After being diagnosed with atypical hyperplasia in 2010, she experienced complete remission after 6 months of oral progestin. She was found to have atypical endometrial hyperplasia again in 2018 and she elected for a levonorgestrel intra-uterine device. The following year the intra-uterine device was removed. In 2021 she was diagnosed with persistent or recurrent atypical hyperplasia. Later that year she experienced disease progression, in the context of barriers to care during the COVID-19 pandemic, and was diagnosed with grade 1 endometrial carcinoma.
Although research on re-treatment outcomes is limited, complete response rates cited in the literature are encouraging, approaching 80–90% in recent studies. 5 6 In the case of this patient, she was counseled on re-treatment and she elected for an additional cycle of fertility-sparing therapy. Re-treatment options are similar to initial treatment options, although further consideration can be given to combined therapies based on the patient’s clinical course, adverse effects, or risk factors.
Dr Chae-Kim: What is the role of metformin in atypical endometrial hyperplasia?
Metformin is an oral anti-hyperglycemic agent widely used in the treatment of type 2 diabetes. Given the association between obesity, hyperinsulinemia, and endometrial cancer, metformin has recently been studied for its potentially therapeutic effects on atypical endometrial hyperplasia or endometrial carcinoma. Pre-clinical studies have shown that metformin has anti-proliferative effects on endometrial cancer cell lines. Metformin is thought to have indirect and direct effects on endometrial cancer cells, including indirectly slowing tumor proliferation by reducing insulin growth factor-1 and insulin, or direct activation of AMPK leading to decreased protein synthesis and tumor cell proliferation via various pathways. Metformin may also modulate expression of progesterone and estrogen steroid receptors to have a synergistic effect with progestin therapy. Several clinical studies have reported favorable outcomes after treatment with metformin as part of combined fertility-sparing therapy with progestin or even as monotherapy. A recent meta-analysis examined outcomes after progestin versus progestin with metformin therapy and found that combined therapy was associated with decreased relapse rates. 7 The data on outcomes after metformin fertility-sparing therapy are limited, however, and there is significant heterogeneity in the data regarding the dosing and duration of metformin therapy for those who pursue conservative treatment. Given that evidence is limited, the role of metformin in fertility-sparing treatment is not yet clear and there is uncertainty regarding the patient population for whom metformin is most beneficial, although initial review of the literature suggests promising outcomes. In practice, clinicians may reserve the use of metformin for women with known diabetes, evidence of hyperinsulinemia, hyperlipidemia or polycystic ovarian syndrome. Further research is needed to clarify the role of metformin in fertility-sparing therapy.
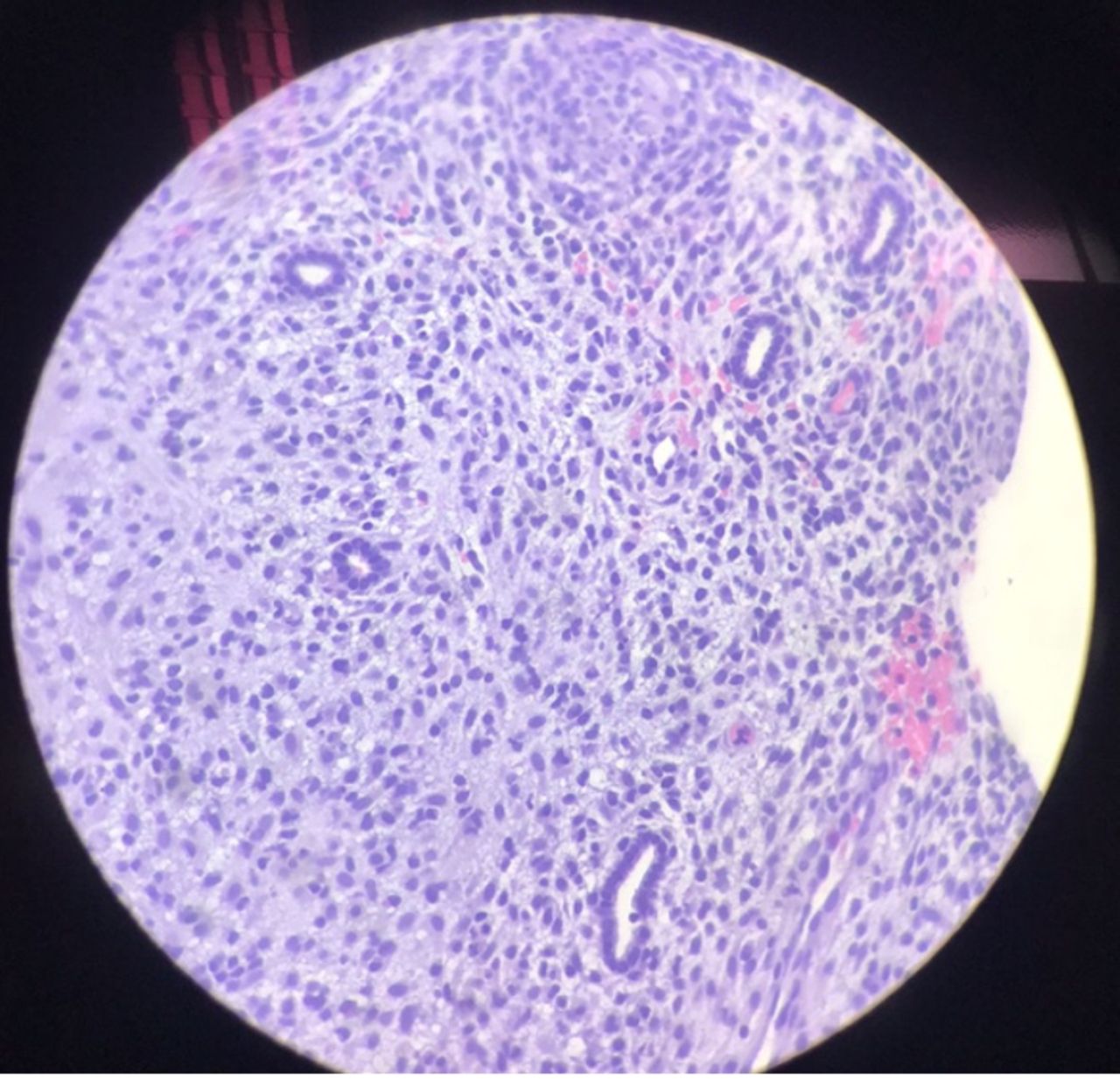
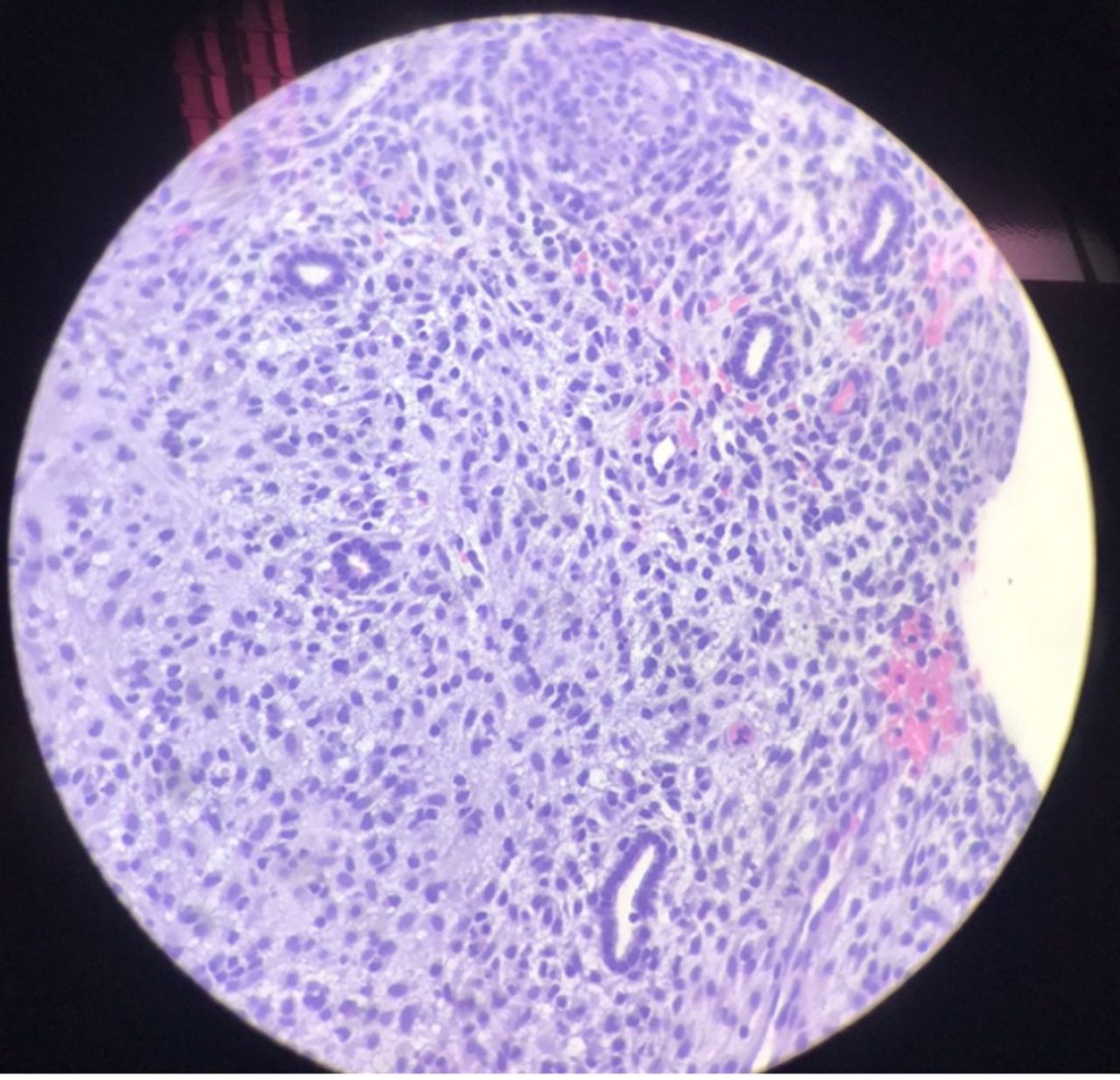
On further discussions with the patient, strict measures such as weight loss and exercise were discussed. When the adenocarcinoma was diagnosed, she decided she would continue with the fertility-sparing treatment and 1000 mg/day metformin was added to the treatment. Three months later a hysteroscopy was performed. The biopsy showed deciduoid reaction of the stroma ( Figure 4 ). As the hysteroscopic image showed a very proliferative endometrium with the intra-uterine device inside the uterine cavity and the existing risk of occult or synchronic carcinoma, a new magnetic resonance image was ordered which showed homogeneous and thin endometrium without signal restriction on diffusion-weighted imaging.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Endometrial mucosa with progestin treatment effect. Hematoxylin and eosin ×10.
Dr Chae-Kim: How often would you suggest endometrial biopsies?
Conservative treatment would be followed with endometrial sampling every 3–6 months. Endometrial sampling can be done with hysteroscopy, dilation and curettage, or endometrial biopsy. The latter approach may be preferred based on the patient’s risk factors for disease progression, anatomic considerations factoring into adequacy of endometrial biopsy sampling, convenience, as well as logistical barriers to surgery.
How long would you wait for a positive pathologic response?
For the initial fertility-sparing treatment, duration of treatment and assessment of positive pathological response may span 6–12 months. This is consistent with guidelines regarding evaluation of fertility-sparing therapy progress and consideration of staging hysterectomy if the patient has persistent or worsening disease. Studies in the literature have cited a wide range of duration of treatment.
After a 3-month period of treatment with the Mirena device and 1000 mg/day metformin, the patient had a complete pathological response. She lost 10 kg and did not have any complications or adverse events from the treatment.
Closing summary
Fertility-sparing treatment is an important and relevant issue for patients of reproductive age with atypical endometrial hyperplasia or endometrial cancer. There are recommended eligibility criteria for fertility-sparing treatment, and many clinical studies have demonstrated excellent response rates after treatment. Some patients do not respond to progestin treatment and a recent prospective study reported on biomarkers of proliferation, progesterone receptor and estrogen signaling that may characterize non-response.8 Specifically, this study found that non-responders had higher baseline expression of proliferation (Ki67) and lower Dickkopf homolog 3 (DKK3) gene expression compared with endometrial biopsies of patients who did respond to progestin therapy. Endometrial sampling after 3 months of treatment showed that the presence of exogenous progesterone effect was less common in patients who did not respond to therapy, suggesting a clinical milestone by which additional fertility-sparing therapies can be initiated.
Among those who pursue conservative management, selected patients may choose to pursue re-treatment in the context of disease persistence or even progression. Due to a limited number of studies, the optimal management for patients who undergo additional fertility-sparing treatments is unclear, although reported outcomes are encouraging. In this case of a young patient who experienced disease relapse and progression, due to pandemic-related barriers to infertility care, fertility-sparing re-treatment with levonorgestrel intra-uterine device and metformin led to a complete pathological response without complications. Close follow-up during re-treatment is recommended and referral to infertility care should be considered to expedite treatment with assisted reproduction.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Footnotes
Twitter @CeciliaDarin1
Contributors MCD contributed to the planning and presentation of the case study, working together with JDG, MT (pathologist), and FB (radiologist). JC-K planned and designed the discussion of the case report, according to the literature and current recommendations.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.