Article Text

Abstract
Cervical cancer is the fourth most common cancer in women worldwide. The preferred treatment for early stage cervical cancer is radical hysterectomy with pelvic lymph node assessment, and adjuvant therapy is suggested according to histopathological risk factors. A landmark study was published in 1999 that established 'intermediate risk' criteria for relapse, showing a benefit in recurrence free rate in patients that received pelvic radiotherapy. Furthermore, in the presence of parametrial, nodal, or vaginal margin involvement, another key study found that the addition of concurrent cisplatin based chemotherapy to radiation therapy improved progression free and overall survival for 'high risk' early cervical cancer. With the advancement in treatment modalities in surgery and radiotherapy, and the improved identification of prognostic histopathological factors, several authors have reconsidered the role of adjuvant therapy after radical hysterectomy in the presence of intermediate risk criteria. Here we review the literature on the evolution of adjuvant therapy for intermediate risk factors.
- Cervical Cancer
- Hysterectomy
- Radiotherapy
Statistics from Altmetric.com
Introduction
Cervical cancer is the fourth most common cancer in women worldwide. According to GLOBOCAN, in 2020 there were 604 127 new cases and 341 831 deaths.1 Treatment depends on the International Federation of Gynecology and Obstetrics (FIGO) stage. In patients diagnosed with early stages (FIGO 2018 IA1 with lymphovascular space invasion, IB1, IB2, and IIA1) not wishing to preserve fertility, the standard management is open radical hysterectomy with lymph node assessment. Radiation may be an option for medically inoperable patients or for those who refuse surgery.2 After surgery, taking into consideration the histopathological factors found in the specimen, the need for adjuvant treatment is determined.2 Radiation therapy after radical surgery reduces the risk of local recurrence,3 and chemotherapy, as a radiosensitizing agent, has been shown to improve overall survival for high-risk patients.4
The use of postoperative radiotherapy for patients with cervical cancer has been described for several decades in retrospective studies.5 6 However, in 1999 and 2000, two prospective trials were published, guiding adjuvant therapy recommendations.4 7 There is currently a debate regarding the role of adjuvant therapy in the presence of intermediate risk factors due to changes in surgical and radiotherapy techniques, better diagnostic images, and inclusion of pathologic and radiologic measurements of tumor size in the current FIGO staging classification.8 The objective of this study was to review the literature on the evolution of indications for adjuvant therapy and evaluate alternatives in patients with early cervical cancer with intermediate risk factors.
Adjuvant Therapy With Intermediate Risk Factors: an Historical Perspective
Survival in gynecological cancers is based on the stage at diagnosis and histopathological features. Specifically, in cervical cancer, factors associated with recurrence have been identified. Chung et al9 found that patients with a bulky primary tumor (≥4 cm), positive nodes, vascular invasion, and/or deep invasion of the cervix (>70%), had more local recurrences and distant metastases. In the Gynecologic Oncology Group study (GOG 49), Delgado et al analyzed 645 women with stage I squamous carcinoma of the cervix who had undergone a radical hysterectomy with pelvic lymphadenectomy and had no gross disease beyond the cervix/uterus and negative para-aortic lymph nodes. Three independent prognostic factors were identified: clinical tumor size, capillary lymphatic spaces involvement, and depth of tumor invasion. The presence of these three factors increased the probability of recurrence at 3 years from 2% to 31%.10
Considering these prognostic histopathological factors,9 10 Sedlis et al7 published a phase III multicenter, randomized clinical trial (GOG 92) to determine if postoperative pelvic radiotherapy following radical hysterectomy and pelvic node dissection would reduce the rate of recurrence and decrease mortality in stage IB cervical cancer patients compared with surgery alone. Eligible patients had one of four combinations of risk factors, including stromal invasion, capillary lymphatic space involvement, and tumor size. Of 277 patients, 137 were randomized to pelvic radiotherapy and 140 to no further treatment. Twenty-one (15%) in the radiotherapy group and 39 (28%) in the no further treatment group had cervical cancer recurrence, 18 of whom were vaginal/pelvic in the radiotherapy group, and 27 in the no further treatment group (p=0.008). The recurrence free rate at 2 years was 88% and 79%, respectively (p=0.008). No significant differences in overall survival were found.
Rotman et al11 published the post hoc follow-up of the GOG 92 study in 2006. In the radiotherapy group compared with observation, a significantly lower risk of recurrence was found (hazard ratio (HR)=0.54; 90% confidence interval (CI)=0.35 to 0.81; p=0.007). Both local (13.9% vs 20.7%) and distant (2.9% vs 8.6%) recurrence rates were lower in the radiotherapy versus the observation group. Regarding overall survival, there were no significant differences between the two groups (HR=0.70; 90% CI=0.46 to 1.05; p=0.074).
Current guidelines for the management of cervical cancer propose adjuvant treatment after radical surgery when one of the four combinations of the following three histopathological factors are present in the surgical specimen: lymphovascular space invasion, stromal invasion, and tumor size (cm) (determined by clinical palpation).2 The National Comprehensive Cancer Network (NCCN) guidelines also mentioned that additional risk factors, such as tumor histology (adenocarcinoma component) and close or positive surgical margins should be considered.2 The option of using concurrent platinum and radiotherapy (category 2B) is proposed for FIGO 2018 stages IA2, IB, or IIA1 with node negative but large primary tumors, deep stromal invasion, and/or lymphovascular space invasion.2 The European Society of Gynaecological Oncology/European Society for Radiotherapy and Oncology/European Society of Pathology guidelines recommend adjuvant radiotherapy in the presence of a combination of risk factors, such as tumor size, lymphovascular space invasion, and depth of stromal invasion (grade B) at final pathology. However, it also allows observation as an alternative in radical hysterectomy performed by 'experienced teams'. However, there is no strict definition on the meaning of experienced teams. Concomitant chemotherapy is not recommended.12
Despite the recommendations, currently the use, selection, and adjuvant treatment options are different among centers and regions. In a survey sent through the European Society of Gynaecological Oncology, it was reported that 81% of participants considered the combination of tumor size, lymphovascular space invasion, and stromal invasion as an indication for adjuvant radiotherapy.13 Eighty-eight per cent of Italian radiation oncologists believed other prognostic factors could be integrated in classic risk criteria (lymphovascular space invasion and suboptimal surgery, other histology than squamous cell carcinoma, high grade disease, age <50 years, close surgical margins, and different combinations of these factors). Furthermore, 66% considered chemoradiation in the case of lymphovascular invasion and suboptimal node dissection, high grade, size ≥4 cm, non-squamous histology, and risk factor combinations. The need to integrate the classic prognostic factors with other variables was unanimously mentioned.14
Evaluation and Criticism of the Sedlis Study
The role of adjuvant treatment in the presence of 'intermediate' risk factors has been the subject of frequent discussion. The previously mentioned trial by Sedlis et al7 has several limitations considering the evolution in the approach to cervical cancer regarding estimation of histopathologic prognostic factors, diagnosis, and treatment. The population treated in the trial is probably different from patients who undergo treatment today, including the factors outlined below.
Histopathologic Factors
In the study by Sedlis et al,7 78.7% of patients had squamous cell carcinoma and 23% had non-squamous subtypes (adenocarcinoma and adenosquamous). It has been shown that non-squamous subtypes are considered more aggressive with different risk factors and prognoses.15 16 Different classifications have been developed for endocervical adenocarcinoma, such as the Silva classification,17 and the International Endocervical Adenocarcinoma Criteria and Classification modified the classification of endocervical adenocarcinomas, separating these into human papillomavirus associated and human papillomavirus independent categories.18 These classifications demonstrate different prognostic features, even in the same histological type. It could be argued that the study of Sedlis et al generates conclusions that primarily apply to squamous cell carcinomas
It is also interesting to mention that although the intermediate risk established by the combination of the factors (tumor depth of invasion, lymphovascular space invasion, and tumor size) predicted a 3 year recurrence of ≥30%,7 it seems that this risk differs according to the histological subtype, and in the presence of one or more factors. Levinson et al16 developed an ancillary analysis of GOG 49, 92, and 141, and included stage I patients who underwent surgery and received no neoadjuvant/adjuvant therapy; among them, depth of invasion was associated with the most significant recurrence risk for squamous carcinoma (16% of risk), while for adenocarcinoma it was tumor size (15% of risk with negative lymphovascular space invasion vs a 25% risk with positive lymphovascular space invasion). This study guides the creation of a nomogram to assess the risk of recurrence based on histology. With these findings, the classic combinations could be reconsidered as a criterion to define adjuvant therapy.
Other prognostic factors have been evaluated in the setting of intermediate risk. Tumor budding is defined as the presence of clusters of tumorous cells detaching from the invasive margin of the primary tumor. Park et al19 evaluated its prognostic value. High tumor budding was defined as ≥5 per high power field for disease free survival. The authors found on multivariate analysis that high tumor budding was an independent prognostic factor for predicting overall survival (HR, 4.96; 95% CI 1.06 to 23.29; p=0.0423). Addition of this factor to the conventional intermediate risk models improved the accuracy of recurrence prediction.
Cibula et al20 retrospectively analyzed different prognostic models, including 15 factors: age along with 14 other factors obtained from the preoperative imaging and pathological assessment (11 tumor related, and three lymph node status related: lymph node positivity, number of positive lymph nodes, and type of metastasis in lymph node). Tumor free distance was defined by measuring the image on a transversal plane as a minimum distance of uninvolved stroma between the tumor and pericervical ring. Adenosquamous tumor type, lymph node involvement, and tumor free distance ≤3.5 mm were the most significant independent factors for the risk of recurrence in the entire cohort. In the cohort of lymph node negative patients, the combination of adenosquamous tumor type and tumor free distance ≤3.5 defined a group of 3% of cases with a recurrence rate (RR) of 33% in comparison with a 6% RR in the rest of the cohort. Tumor free distance was the best marker in both predictive models for the entire population and for the lymph node negative subgroup. This factor, when evaluated preoperatively, could represent an advantage for planning the surgical approach.
Although the proposal to apply normograms to determine adjuvant therapy through an individualized approach according to risk of recurrence, and the addition of preoperative and postoperative prognostic factors is promising,16 19 20 these should be validated before their use in clinical practice.
Lastly, it is important to highlight that in the study by Sedlis et al,7 institutional pathologists measured the depth of stromal tumor invasion and made a determination of the presence or absence of tumor in the capillary lymphatic spaces. Subsequently, and as quality control, all histology slides were reviewed by two pathologists of the GOG pathology committee but tumor size was only clinically determined.
Changes in FIGO Stage IB Classification
In 1958, the cervix was the first organ to be assigned to a clinical staging system for cancer by FIGO, and the pathologic (TNM) staging was used to report nodal and metastatic disease status. The classification has undergone modifications in recent decades.8 By 1994, 'bulky' stage IB was divided into IB1 (≤4 cm) and IB2 (>4 cm), to establish specific treatment strategies, according to their different prognostic impact.21
In the FIGO 2009 classification, staging was based mainly on physical examination; the use of diagnostic imaging techniques to assess the size of the primary tumor was encouraged but not mandatory, given the limited resources in some regions.22 In 2018, FIGO revised the staging classification to allow clinical, radiological, or pathological findings as valid tools to assign stage of disease.8 In addition, taking into account that recurrence rates are lower in stage I tumors <2 cm in size compared with tumors measuring 2–4 cm, stage IB was defined as an additional cut-off at 2 cm, establishing three stage categories (IB1, IB2 and IB3).23
The study by Sedlis et al7 included stage IB patients with tumors from <2 cm (28.1%) to >6 cm (10.4%). There were 74 (26.7%) patients with tumors >4 cm, a factor taken into account in two of the four combinations included in that trial. Based on this information, just over a quarter of the patients who participated in that study would not be candidates for surgery today, considering that they have stage IB3 by current guidelines and would, in turn, be treated with chemoradiation.
Tumor Size Measurement
Determining the actual size of the tumor has been the subject of debate in patients with cervical cancer. The evidence suggests that clinical examination, although a standard and necessary step in the initial evaluation of patients, is limited in its ability to reliably ascertain tumor size, with an accuracy of 47–70%.24 Among the limitations are that it is examiner dependent, has a high interobserver variability, its impacted by patient specific factors such as tolerance of examination or body mass index, and it becomes increasingly more challenging in patients with endocervical tumors.24 25
For measurement of tumor size by histopathology evaluation, it is important to highlight the discrepancy among institutions and even among pathologists on reporting.24 In the FIGO 2018 classification, the term 'diameter' is used interchangeably with 'dimension', when they represent two different definitions and measurements. In addition, inconsistencies have been found in the measurement according to the location of the tumor (eg, if it is in the anterior or posterior lip, or if the tumor is circumferential).26 Recent data have shown discrepancies in the estimation of preoperative tumor size compared with postoperative tumor size. Uppal et al27 analyzed preoperative tumor size during the clinic visit and tumor size as reported in the pathology report (final tumor size) in 744 patients with early cervical cancer undergoing radical hysterectomy. A total of 291 patients had no visible disease on preoperative assessment, but 58 (19.9%) patients had tumors >2 cm on final pathology, and of 257 patients with preoperative assessment of tumor size <2 cm, 89 (34.6%) had tumors >2 cm on final pathology.
In the study by Sedlis et al,7 it is mentioned that tumor diameter was estimated by palpation and there is no mention of who performed the physical examination or standardization of this measurement. In addition, there is no mention of tumor size by images. There was no documentation of evaluation of tumor size in the final surgical specimen. What the reproducibility of these selection criteria would be in current practice is difficult to determine when using magnetic resonance imaging, computed tomography scan, or ultrasound imaging, which allow a more precise estimation of tumor size.
Characteristics of Radical Surgery
Details regarding the radicality of surgery (type II or III radical hysterectomy) was not well established in the study by Sedlis et al. No details are provided on the surgical volume of radical surgeries performed by physician and/or center. In the study, all patients underwent bilateral pelvic lymphadenectomy but it is important to mention that the integration of sentinel lymph node biopsy and ultrastaging has been recently introduced into the routine management of cervical cancer,28 29 allowing detection of an additional 10–15% of cases with low volume disease.30 The technique also identifies sentinel lymph nodes in 'unexpected' nodal basins in up to 17% of patients.31 Detection of lymph node involvement using this technique identifies patients with high risk for recurrence who may benefit from adjuvant treatment with chemoradiation.30 With the evolution of radical surgery regarding the technique and indications in the last decade, the results of the Sedlis study could have less external validity in current clinical settings.
Advances in Radiotherapy Techniques
Treatment modalities with radiotherapy have been modified over time.32 Initially, teletherapy was administered using a two-dimensional technique. Subsequently, three-dimensional conformal radiation therapy was introduced and with the advancement of radiotherapy, the standard treatment modality is intensity modulated radiation therapy, which makes it possible to deliver doses to target volumes with less toxicity to nearby critical structures33 without differences in disease outcomes.34
The clinical practice guideline of the American Society for Radiation Oncology35 currently suggests that for patients meeting intermediate risk criteria, whole pelvic radiotherapy may be delivered to a total dose of 4500–5040 cGy, in 180 cGy per fraction, or 4000–4400 cGy in 200 cGy per fraction. In the Sedlis study,7 pelvic irradiation was given with a fourfield technique with a megavoltage beam, although cobalt-6 was allowed if the source–skin distance was >80 cm. The radiation dose was 46–50.4 Gy with daily fractions of 1.8–2 Gy over 4.5–6 weeks. Currently, radiation techniques such as three-dimensional conformal radiation therapy, intensity modulated radiation therapy, and volumetric modulated arc therapy are the standard of care, with potentially lower long term morbidity. For future studies, implementation of these techniques should be considered, seeking to improve pelvic control and thereby disease free survival, with a lower threshold (8–10% risk of pelvic relapse).36
Further Points of Consideration
The study of Sedlis et al demonstrated a reduction in risk of recurrence after radiotherapy, but not in overall survival. One potential reason is that the sample size might have been too small as this study was planned to have 80% power to detect risk reductions of 46% or greater in overall survival; however, patients with radiotherapy had only a 30% reduction in the risk of mortality and significance was not reached.37 Other aspects related to the design of the study include the evidence of a higher percentage of worse prognostic factors in the radiotherapy group, more adenocarcinomas, and tumors >3 cm.11 A potential risk of bias is to be highlighted because the method of randomization, allocation concealment, or blinding of the investigators was not reported.7 It has been described that inadequate concealment of allocation and lack of blinding are often associated with overestimation of the effects of treatment.38 All of these aspects should be considered in the design of a new study.
Considerations for Adjuvant Therapy in the Intermediate Risk Population
Impact of Observation Versus Adjuvant Therapy
When adjuvant therapy is administered in the presence of intermediate risk criteria, the oncological benefit must be balanced against morbidity. Regarding the oncological results, there are inconsistent results in the literature and this is likely because patient populations are heterogeneous, most studies are retrospective, and different treatment strategies have been used. Treatment recommendations for patients with intermediate risk disease include radiotherapy with or without brachytherapy, chemoradiotherapy, or observation.2 12
Rogers et al39 evaluated the effectiveness and safety of adjuvant therapies after radical hysterectomy for early stage cervical cancer. Two prospective randomized trials were included.11 40 No significant difference was found in risk of death within 5 years between women who received radiation and those who received no further treatment (RR 0.8; 95% CI 0.3 to 2.4). However, women who received radiation had a significantly lower risk of disease progression at 5 years (RR 0.6; 95% CI 0.4 to 0.9). The authors concluded that the available evidence is not of high quality.
Regarding the role of concomitant chemotherapy, Kim et al41 evaluated 316 patients with stage IB–IIA cervical cancer who underwent radical hysterectomy with pelvic lymphadenectomy and had one or more intermediate risk factors and no high risk factors. Based on adjuvant treatment (adjuvant radiotherapy alone vs adjuvant chemoradiotherapy), the 5 year recurrence free survival rates (90.8% vs 88.9%, p=0.63) and 5 year overall survival rates (95.9% vs 91.0%, p=0.29) were not different.
Guo et al42 performed a systematic review with meta-analysis that evaluated the effect of post-surgical adjuvant radiotherapy versus adjuvant chemoradiotherapy in patients with intermediate risk. Eleven retrospective cohort studies and two randomized clinical trials were included. Adjuvant chemoradiotherapy was found to have better recurrence free survival in patients with multiple intermediate risk factors (odds ratio (OR) 3.11; 95% CI 1.04 to 4.99; p<0.0001; i2=6%.) However, similar benefit was observed between both regimens in the presence of a single intermediate risk factor (OR 1.80; 95% CI 0.96 to 3.36; p=0.07; i2=0%). To confirm the effect of chemotherapy in the intermediate risk group, the results of a prospective study from the GOG 263 (NCT01101451) are awaited43
Brachytherapy has been included in some institutions as adjuvant therapy in the setting of intermediate risk. This treatment technique is recommended in the presence of positive surgical margins as a high risk factor.2 13 Rotman et al11 noted a high locoregional failure rate (14% in the radiation arm), suggesting the need to increase radiotherapy doses, either by external beam or in conjunction with brachytherapy. Further control in the pelvis, specifically in the vagina, may be achieved by using additional vaginal brachytherapy.36 Bronsart et al44 examined the role of adjuvant brachytherapy alone as an alternative to external beam radiation therapy in 40 patients. This treatment was indicated when tumor size was ≥2 cm and/or in the presence of lymphovascular space invasion. Ninety per cent of patients were in complete remission and four patients (10%) experienced tumor relapse, all in the peritoneal cavity. At 5 years, overall survival was 83.6% (95% CI 67.8% to 100%) and disease free survival was 85.1% (95% CI 72.6% to 99.9%). On the other hand, Yu et al45 evaluated the role of postoperative adjuvant chemotherapy combined with intracavitary brachytherapy. One hundred and two patients were subjected to chemotherapy combined with intracavitary brachytherapy (chemotherapy+intracavitary brachytherapy) and the remaining 70 patients were treated with concurrent chemoradiation. No significant difference was observed in 3 year disease free survival (93.2% vs 95%, p=0.862), and 3 year overall survival (96.0% vs 95.4%, p=0.599).
Observation in the presence of intermediate risk factors is becoming increasingly more common. Cibula et al46 published a retrospective study comparing outcomes in patients with intermediate risk factors that underwent observation or radiotherapy according to the protocol of three different centers. In all, 231 patients were evaluated in the study; 127 patients were treated with radical surgery without adjuvant treatment (surgery only group) and 104 patients with radical surgery, followed by adjuvant radiotherapy (control group). No differences were found for total recurrence rate between the groups (surgery only group 6.3% vs control groups 11.5%; p=0.168), 5 year overall survival (95% vs 91%; p=0.317), and disease specific survival (96% vs 95%; p=0.745). It is interesting to note that this study demonstrated improved oncologic outcomes in the group without adjuvant treatment, compared with the original GOG 92 (recurrence rate 6.3% and local recurrence rate 1.6% vs Sedlis study which were 27.9% and 19.3% respectively).
Van der Velden et al47 retrospectively analyzed 161 patients with intermediate risk factors who did not receive adjuvant treatment within a cohort of 937 patients with cervical cancer stage IB (FIGO 1995 classification) who underwent open radical surgery. Twenty-five (15.5%) patients had a recurrence, and nine (5.6%) patients had an isolated locoregional recurrence. The 5 year recurrence free survival was 86.6% and the 5 year overall survival was 90%.
Cao et al48 retrospectively compared observation with adjuvant radiotherapy or chemoradiation in 861 patients with stage IB and IIA disease (FIGO 2009 classification) and intermediate risk. In total, 75.2% (n=646) of patients had tumors >4 cm and 46.5% (n=400) of patients had lymphovascular space invasion. Eighty-five (9.9%) underwent no adjuvant treatment, 283 (32.9%) underwent adjuvant radiotherapy, and 493 (57.2%) underwent concurrent chemoradiation. The 5 year recurrence free survival was 87.1%, 84.2%, and 89.6% (p=0.27) for the no adjuvant treatment, radiotherapy alone, and concurrent chemoradiotherapy groups, respectively. Adjuvant treatment was not a significant independent prognostic factor for recurrence free survival. On multivariate analysis, lymphovascular space invasion was an independent negative prognostic factor for recurrence free survival (HR 2.26; 95% CI 1.44 to 3.55; p<0.001).
At the population level, Nasioudis et al49 reported a study using the National Cancer Database. The authors investigated the outcomes of observation alone versus adjuvant radiotherapy for 765 patients with squamous, adenosquamous carcinoma, or adenocarcinoma of the cervix, pathological stage IB disease (FIGO 2018 classification), who underwent radical hysterectomy with at least 10 lymph nodes removed (all negative), negative tumor margins, and presence of intermediate risk factors, defined as tumor size 2–4 cm with lymph-vascular invasion or tumor size >4 cm. As the National Cancer Database does not collect data on the depth of stromal invasion, the traditional criteria of Sedlis et al7 were not applied. The 4 year overall survival rates were 88.4% and 87.1% (p=0.44) among patients who received or did not receive adjuvant radiation therapy, respectively. When the prognostic variables age, histology, and surgical approach were controlled, there were also no significant differences in overall survival between the groups. The authors found no benefit of administering concurrent chemotherapy with 4 year overall survival rates of 89.8% and 86.3% (p=0.36). Of note, in this study, most patients (57.9%) received, in addition to radiotherapy, concomitant chemotherapy thus reflecting the heterogeneity in the treatment approach. On the other hand, it should be highlighted that the National Cancer Database does not collect data on tumor recurrence, an outcome that demonstrated a benefit from the addition of adjuvant radiotherapy in the Sedlis study.7
Similar results have been published in other retrospective studies comparing the use of adjuvant radiotherapy (with or without chemotherapy) versus observation for intermediate risk patients.50–53 Gómez-Hidalgo et al54 recently conducted a systematic review with meta-analysis including articles with ≥10 patients with two comparative arms. The relative risk of recurrence (RR 1.49; 95% CI 0.81,2.75) and the relative risk of mortality (RR 1.34; 95% CI 0.71,2.54) were similar in both groups independently whether they did or did not receive adjuvant therapy.
Treatment Related Morbidity
Another aspect to consider when deciding whether to provide adjuvant therapy in intermediate risk patients is treatment related morbidity. This is important because approximately 28% of patients undergoing radical surgery for early cervical cancer receive adjuvant therapy.55 The reported incidence of toxicity associated with adjuvant treatment varies in different studies due to the use of many classification systems or incomplete records, especially regarding mild toxicity. Late severe toxicity was observed in about 5% of patients treated with postoperative radiotherapy and in up to 15% of those treated with chemoradiation.56 Potential morbidity of pelvic irradiation includes diarrhea, urinary urgency or frequency, hematuria, as well as potential urinary or bowel incontinence57 The morbidity of radical surgery followed by radiation therapy is sufficiently great that clinicians should consider primary chemoradiation for patients with a need for subsequent radiation after surgery.58
Sedlis et al7 reported 6% grade 3–4 adverse events in the radiotherapy arm versus 2.1% in the no further therapy group. Kim et al41 reported that combined treatment with chemoradiotherapy was associated with a significantly higher risk of grade 3 toxicity compared with radiation therapy alone. Sandadi et al59 compared the morbidity of radical surgery with or without adjuvant radiation therapy in stages IB1–IB2 cervical carcinoma (FIGO 1995 classification). The rate of grade 3 or higher complications was similar (5% vs 4%, respectively; p=0.999). Although it is assumed that the addition of adjuvant therapy to surgical management increases severe morbidity, modern surgical and radiotherapy techniques could limit its impact. Lastly, several studies suggest that the quality of life and sexual functioning of cervical cancer survivors treated with radiotherapy are worse than surgery alone or surgery followed by chemotherapy without radiotherapy.60 61 This aspect is crucial when deciding to provide adjuvant therapy.
Considering the technological advances in radiotherapy described above, modifications in the surgical technique, and growing evidence of similar oncological outcomes in providing adjuvant versus no additional treatment, a reduction in treatment related morbidity is expected for this population of patients with early cervical cancer in future studies.
Perspectives
As the current clinical diagnosis and management of cervical cancer has evolved since the original Sedlis et al7 publication more than 20 years ago, new evidence has been proposed to establish what is the best treatment option for patients with intermediate risk factors, even including chemotherapy.
GOG 26343 is a randomized phase III clinical trial whose objective is to determine if postoperative adjuvant chemoradiation therapy can significantly improve recurrence free survival compared with radiation therapy alone in FIGO 2009 stage I–IIA cervical cancer patients with intermediate risk factors after treatment with radical hysterectomy. The trial has recruited 341 participants. In arm 1, patients receive pelvic external beam radiation therapy or intensity modulated radiation therapy once daily, 5 days a week, for 5.5 weeks. In arm 2, patients receive cisplatin intravenously over 1–2 hours on day 1, weekly for six cycles and undergo radiotherapy as in arm 1. According to the latest update on ClinicalTrials.gov, the estimated final data collection date for the primary outcome measure is April 11, 2024.
A phase III randomized prospective clinical trial has recently been registered (NCT04989647). The CERVANTES trial (Intermediate Risk Cervical Cancer: Radical Surgery±Adjuvant Radiotherapy),62 is expected to accrue a total of 514 patients. It will include patients with FIGO 2018 stages IB1–IIA, squamous cell, and HPV related adenocarcinoma types and four new different risk factor combinations as follows: (1) tumor ≥4 cm; (2) tumor >2 cm but <4 cm and lymphovascular space invasion; (3) tumor >2 cm but <4 cm and tumor free distance <3 mm; and (4) tumor >2 cm but <4 cm and deep stromal invasion (>2/3). Adenosquamous, non-associated HPV adenocarcinoma, lymph node compromise, R1 resection, and patients that received neoadjuvant chemotherapy will be excluded.
All patients will undergo a radical hysterectomy, sentinel lymph node biopsy, and systematic pelvic lymphadenectomy, and will be randomized to no further treatment or adjuvant treatment (radiotherapy±chemotherapy). The primary outcome will be disease free survival at 3 years and secondary outcomes will be overall survival, pelvic disease free survival, quality of life, and adverse events. One major potential confounder for this study is the fact that it allows for implementation of minimally invasive surgery, and given the results of the LACC trial55 demonstrating worse oncologic outcomes after minimally invasive radical hysterectomy, the results of the CERVANTES trial will need to be scrutinized for this element. It is expected to finish accrual in December 2029 with results available in December 2032. The results of this study will be highly anticipated to establish, in a modern era, adjuvant therapy in patients with cervical cancer with intermediate risk factors.
Conclusions
To date, recommendations for the management of early cervical cancer are that adjuvant radiotherapy should be considered in the presence of a combination of risk factors at final pathology, such as tumor size, lymphovascular space invasion, and depth of stromal invasion. However, the only evidence supporting adjuvant treatment in intermediate risk is the GOG92 study, with the potential limitations described given the evolution of cervical cancer diagnosis and management in recent decades. It is pertinent to establish new management alternatives, with adequately controlled clinical trials and standardization of imaging, histopathological factor evaluation, and radiotherapy techniques to assess the oncological benefit of different types of adjuvant treatment, including observation. The associated morbidity and quality of life should be considered as outcomes (Figure 1). Until new evidence is published, adjuvant therapy should continue to be individualized in the intermediate risk clinical setting.

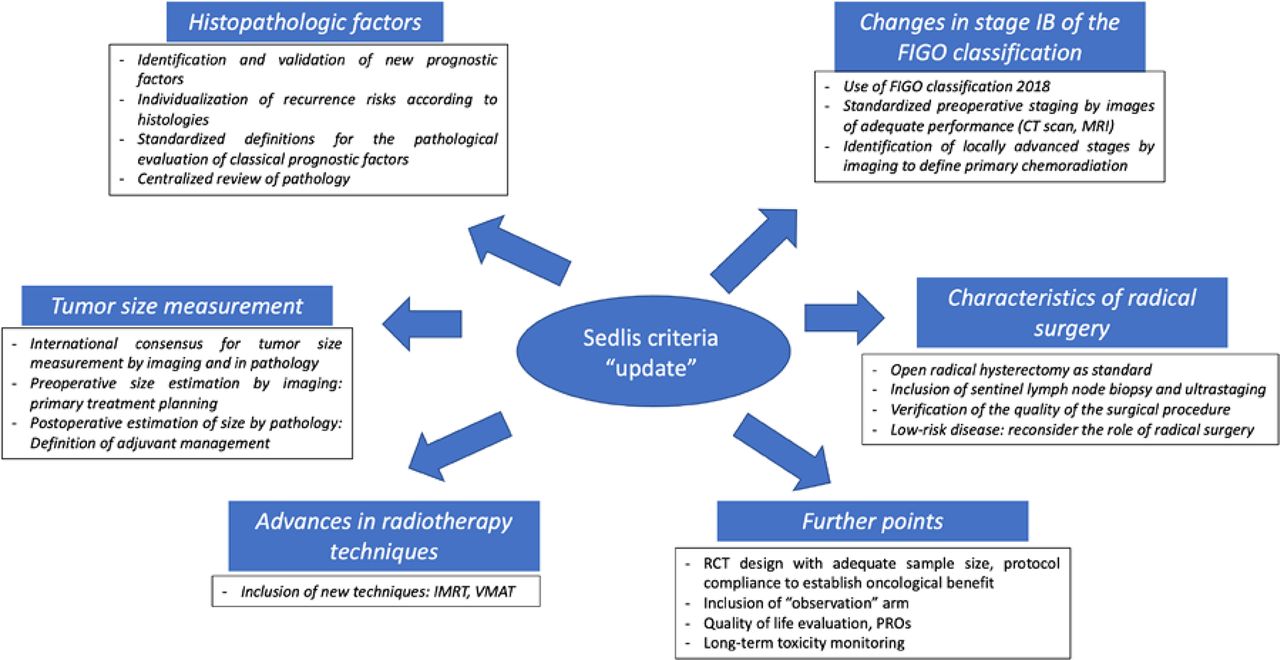{kind=link}
Key elements in Sedlis criteria 'update'. CT scan, computed tomography scan; FIGO, International Federation of Gynecology and Obstetrics; IMRT, intensity modulated radiation therapy; MRI, magnetic resonance imaging; PROs, patient reported outcomes; RCT, randomized controlled trial; VMAT, volumetric modulated arc therapy.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Footnotes
Contributors Study design, literature acquisition, manuscript writing, and manuscript review: JR, DV-C, and RP.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.