Article Text

Abstract
Objectives Schwannomas are uncommon, benign, indolent, nerve sheath tumours with low malignant potential; commonly affecting the nerves of the head, neck, mediastinum and extremities. Two pudendal cases have been reported. Their deep, complex location challenges resection - via the ischiorectal fossa in our case.
Methods A 24-year-old female reported an enlarging left perineal mass over eight years; associated with numbness and sexual dysfunction. This was 7x5cm on examination, distal to Alcock’s canal, with no vaginal, rectal or anal sphincter involvement. It was defined and mildly FDG-avid on imaging. Biopsies confirmed schwannoma. She reports no neurological deficit or evidence of recurrence following resection.
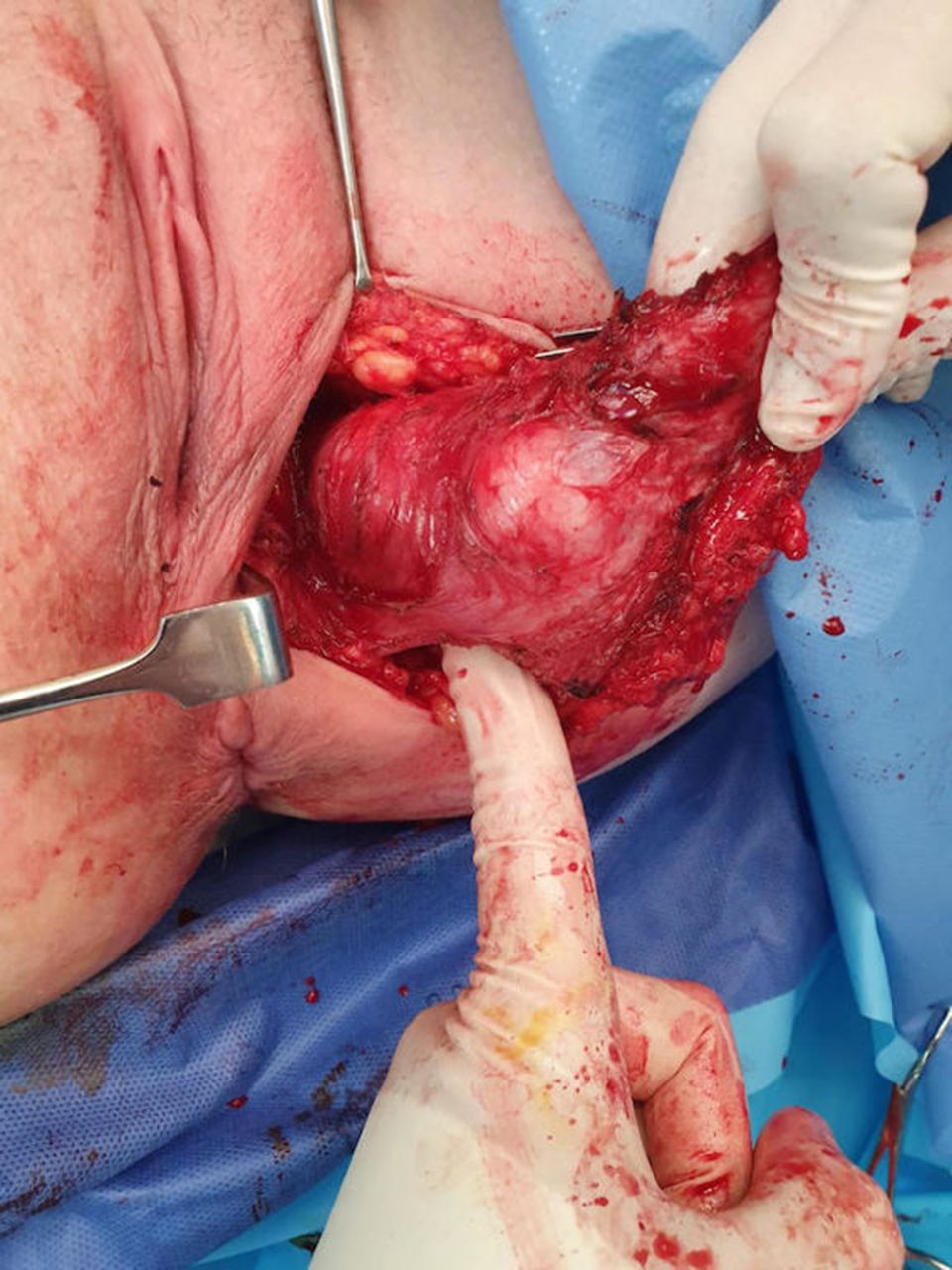
Results Alcock’s canal is directly accessed via the ischiorectal fossa with minimal pelvic muscle and ligament disruption. The pudendal nerve arises from the S2–4 sacral nerve and travels forward laterally in the pelvis within this obturator internus fascial sheath. It has both motor and sensory functions. The ischiorectal fossa is a pyramidal space lateral to the anal canal and below the pelvic diaphragm. It contains the internal pudendal and inferior rectal vessels and nerves.

{kind=link}
{kind=link}
Conclusions Pudendal nerve schwannomas are rare, arising from a single non-functioning sensory fascicle. Following preoperative imaging, this approach is safe and effective to achieve complete surgical resection, avoiding relapse. Other risk factors include incontinence and sensory defecit. The procedure requires an in depth knowledge of the pelvic anatomical spaces, their contents and boundaries.