Article Text

Abstract
Introduction/Background*There are around 3,200 new cases of cervical cancer(CC) each year in the UK and it accounts for at least 2% of all new cancer cases. Management can involve surgery for early-stage disease or chemoradiation(CRT). In our regional cancer network, we explored the disease course, changing management paradigm, complications and outcomes of patients with T4/stage IVA(FIGO 2009) CC over a 10-year period.
Methodology We carried out a retrospective, multicentre analysis between Jan 1 2010 and Dec 31 2020. The project included 4 NHS trusts in the region. Overall, 274 cervical cancer cases were reviewed, 35 cases were stage 4A and therefore suitable for analysis. In each case, treatment protocol(including radiotherapy dose/fraction), urinary diversion procedure, presence of fistula and survival outcomes were reviewed. Kaplan-Meier analysis and Logrank tests were used to compare survival distributions.
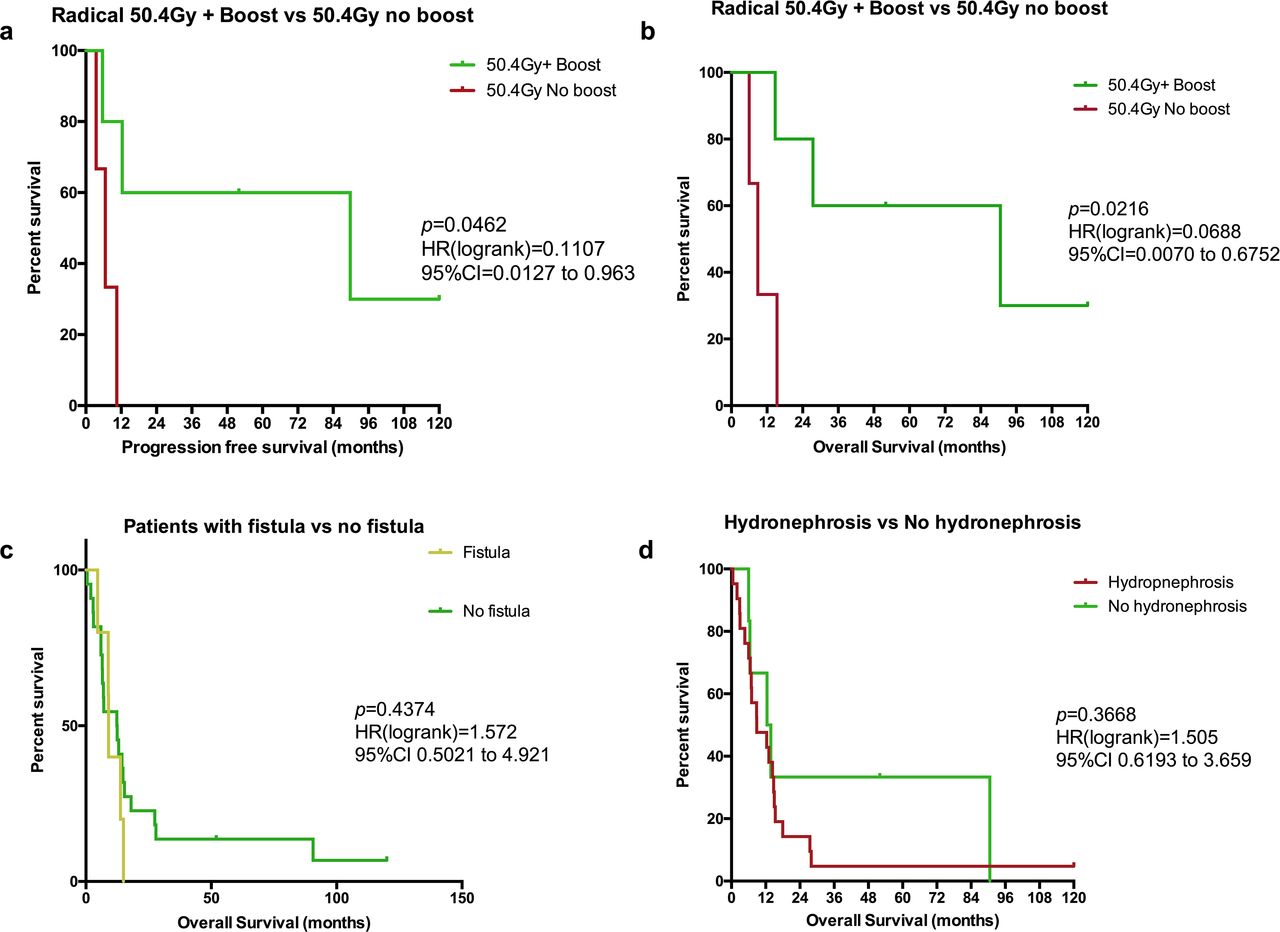
Result(s)*Median PFS of those who received 50.4Gy with a boost(external beam 14.4Gy in 8# to include compromised parametria or 19.5Gy in 3# HDR) vs no boost was 89.8 months vs 6 months, p=0.0462. Their median OS were 90.6 months vs 8.8months respectively p=0.0216. Those treated with palliative intent had a median OS of 8 months while those with a poor performance status(PS>2) and hence managed with best supportive care(BSC) died within 6.5months of presentation. 7/35(20%) patients had evidence of either vesico-vaginal(n=5) or recto-vesico-vaginal fistula(n=2). 2 patients developed fistula as a result of therapy. Presence of fistula (9 vs 12.42 months , p=0.4374) and hydronephrosis (8.8 vs 13.1 months, p=0.3668) did not lead to a significant difference in OS. Patient age (≥50yrs) and high PS were found to be associated with increased risk of death, p<0.0330)
{kind=link}
Progression free and overall survival Kaplan-Meier curves
Conclusion*Admittedly, there were fewer patients in some of the groups analysed however, the data has shown the impact of presence or absence of boost treatment on OS and PFS. Those treated with palliative intent and BSC unsurprisingly but predictably had poorer outcomes. Presence of fistula or hydronephrosis did not significantly impact patient OS. However, higher age at diagnosis and fitness was associated with increased risk of death.