Article Text

Abstract
Introduction/Background*Identifying risk factors for lymph node metastases in early-stage cervical cancer may aid in tailoring treatment. Unfortunately, early-stage cervical cancer research is often hampered by small sample sizes.
A natural solution to increase sample size is to incorporate data from multiple sources, traditionally done through centralization. Unfortunately, this approach presents disadvantages concerning privacy protection. Alternatively, models can be trained in one source and tested in another setting, sharing only the model coefficients (figure 1). This approach does not disclose any privacy-sensitive information. Additionally, external validation provides stronger evidence on the generalizability of the obtained statistical model.
In this study, we used the alternative approach to increase sample size and identify risk factors for postoperative lymph node metastases (pN1) in early-stage cervical cancer.
Methodology We conducted an international observational cohort study using data from the Danish Gynaecologic Cancer Database (DGCD) and the Netherlands Cancer Registry (NCR). We included women diagnosed with early-stage cervical squamous cell carcinoma, adenocarcinoma or adenosquamous carcinoma between 2005–2017, who were treated with radical surgery.
We generated two logistic regression models to identify risk factors for pN1. Model A was trained on NCR data and tested with DGCD data, while model B was obtained the other way around. The performance of each model was assessed using areas under the curve (AUCs).
Result(s)*A total of 2735 patients were included in the analyses.
In model A – trained on data from 1476 Dutch patients and tested with data from 1259 Danish patients – tumour size (odds ratio 1.62; 95% confidence interval [1.37–1.91]), depth of invasion (1.30 [1.12–1.53]) and LVSI (5.13 [3.50–7.52]) were identified as risk factors for pN1, and body mass index as protective factor (0.80 [0.67–0.95].
In model B, trained on Danish data (n=1259) and tested with Dutch data (n=1476), tumour size (1.48 [1.23–1.79]), depth of invasion (1.27 [1.04–1.54]) and LVSI (3.85 [2.53–5.86]) were associated with increased risk of pN1.
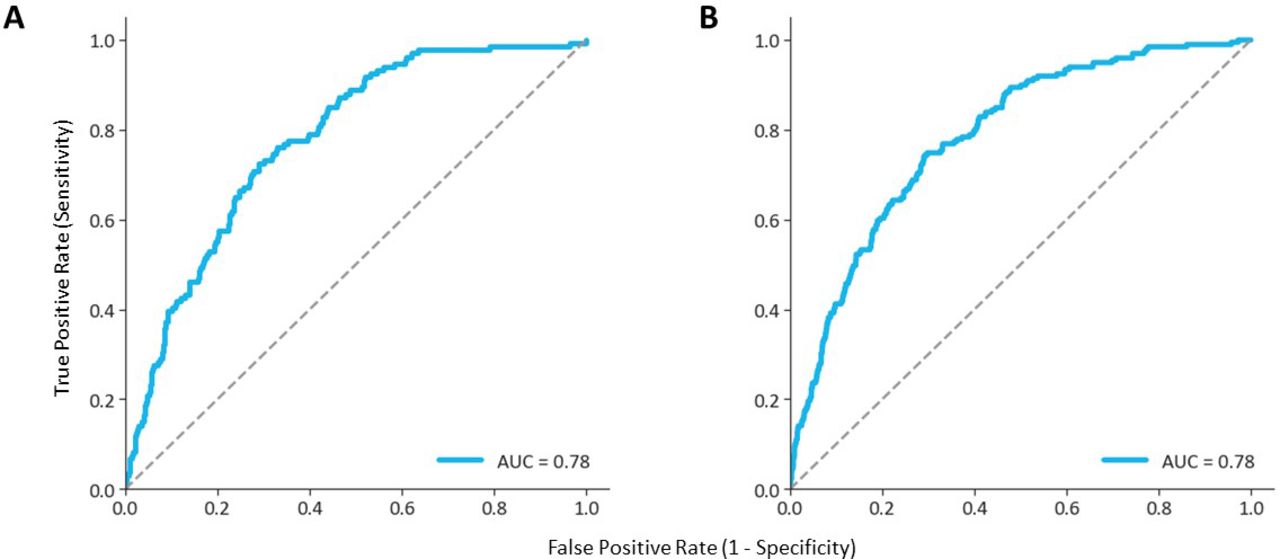
External validation of model A and B both showed AUCs of 0.78 (figure 2).

A privacy-preserving alternative to small sample analysis. Model A is trained on data from the NCR and tested on DGCD data. Model B was obtained the other way around. Only model coefficients need to be shared and, thereby, no privacy-sensitive information is disclosed
{kind=link}
{kind=link}
Areas under the curve for two models identififying risk factors for postoperative lymph node metastases in earl-stage cervical cancer. 2A: Model A trained with NCR data, tested on DGCD data; 2B: Model B trained with DGCD data, tested on NCR data.
Conclusion*Tumour size, depth of invasion and LVSI were identified as risk factors for pN1 in both models.
Separate models, containing either Danish or Dutch data have shown to be valid by privacy-preserving external validation.