Article Text

Abstract
Introduction/Background*Taxane-based chemotherapy used in treating gynecologic malignancies, results in one third of patients developing grade 2 or higher chemotherapy induced peripheral neuropathy (CIPN). Currently, there is no test which predicts who is at increased risk of CIPN. Pharmacogenomic testing may result in the ability to better predict risk of CIPN allowing personalized treatments to avoid this distressing side effect and improve quality of life.
Methodology Patients were enrolled from August 2020 to November 2020 in a prospective, case-control trial evaluating pharmacogenetic predictors of CIPN in women previously treated with at least 3 cycles of taxane-based chemotherapy for histologically confirmed gynecologic malignancies. Buccal saliva samples were used to test for 64 prespecified drug metabolism variations. All testing was performed by αLPHA-GENOMIX laboratories.
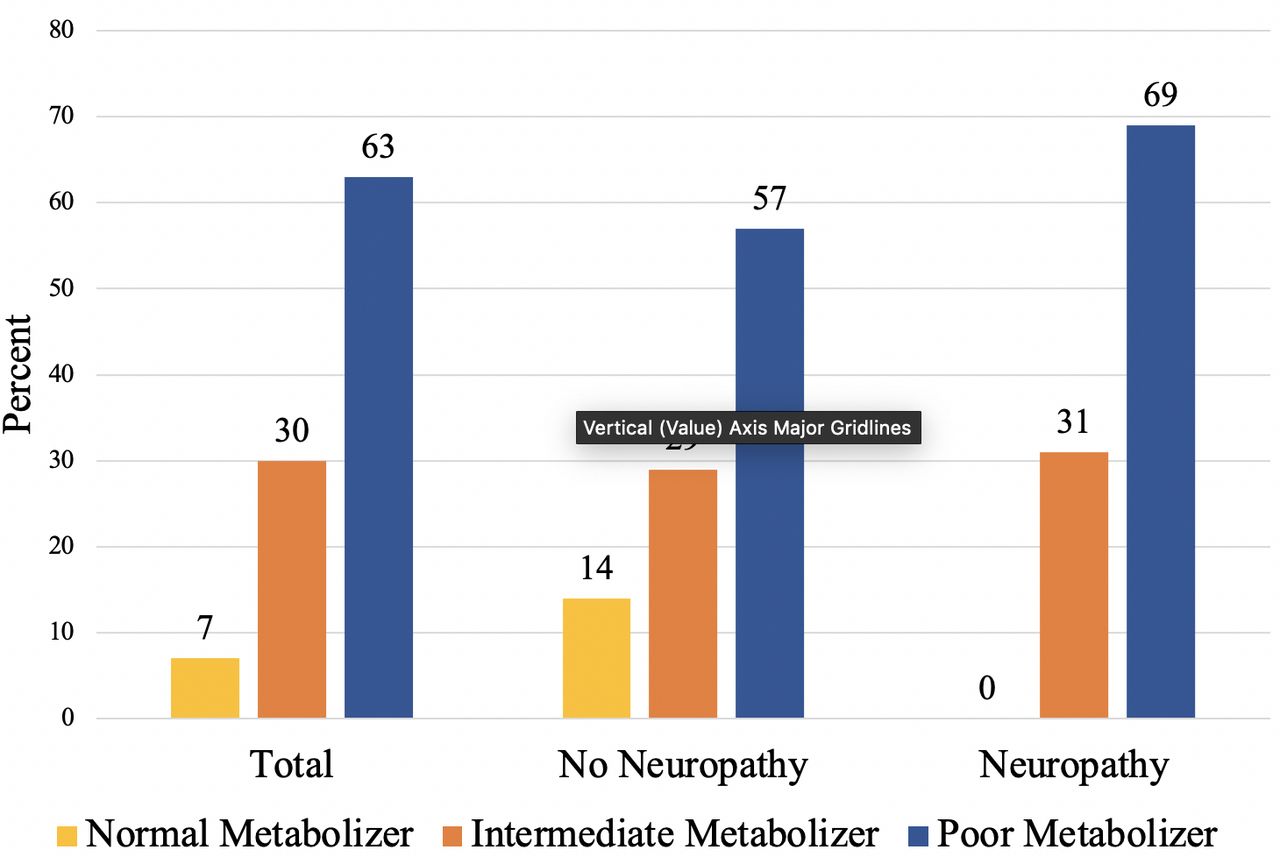
Result(s)*Of 102 enrolled patients, 58%, 28%, 14%, and 2% had ovarian, endometrial, or cervical cancers, respectively. The median age was 67, and 72% were white. A total of 16% of patients were treated with 3-4 cycles, 57% received 5-7 cycles, and 27% received 8 or more cycles of chemotherapy. Half of the patients had grade 2 CIPN. There was no difference in age, race, disease site, or number of chemotherapy cycles (p>0.05) when comparing between the two groups. Of the 64 tested pharmacogenomic alterations, CYP3A5 genotype (p=0.023), CYP3A5 phenotype (0.021), and CYP2D6 genotype (p=0.009) were associated with increased risk of CIPN. Patients who developed CIPN and had CYP3A5 genomic alterations most often were categorized as having the 3/3 allele (63%) and were also categorized as poor metabolizers (69%). Among the 38 genotypes of CYP2D6 there was no variation which contained the majority of patients.

{kind=link}
Differences in CYP3A5 phenotype compared between all patients, those without CIPN, and those with CIPN CYP3A5 Genotype
Conclusion*Pharmacogenomics appear associated with the development of CIPN and maybe able to help personalize treatment decision making. This data supports future large-scale trials to better determine and define molecular variants which lead to CIPN.