Article Text

Abstract
Introduction/Background*While being recognized as negative prognostic factors for other malignancies (e.g. endometrial and cervical cancer), preoperative anemia and preoperative leukocytosis have not been established as negative prognostic factors for EOC. Similarly, despite the accumulating evidence of preoperative thrombocytosis, it remains unclear whether it significantly adds to the prediction of survival of individual advanced stage EOC patients in relation to more established prognostic factors. The objective of this study was to assess the prognostic impact of the aforementioned preoperative hematologic parameters in relation to more established prognostic factors. Additionally, the aim was to develop nomograms based on established prognostic factors along with preoperative anemia, thrombocytosis and leukocytosis to predict the probability towards ≤3-, ≥5- and ≥8-year overall survival (OS) for individual advanced EOC patients.
Methodology Patients consecutively diagnosed with advanced EOC between 01-01-1996 and 01-01-2010 who underwent primary treatment in the eastern part of the Netherlands were identified from our database. Three nomograms were developed. Nomograms’ candidate predictors included nine established prognostic factors combined with preoperative anemia, thrombocytosis and leukocytosis. Candidate predictors were fitted into three multivariable logistic regression models (i.e. ≤3-year, ≥5-year and ≥8-year OS models). Multiple imputation by chained equations was conducted to account for missing data. Model performance was assessed with the AUC, Brier score and calibration curves. Bootstrap internal validation was conducted to correct for model-optimism.
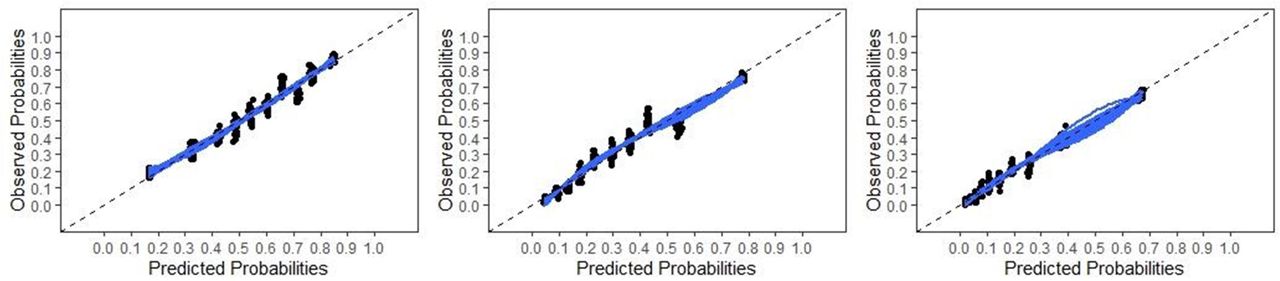
Result(s)*A total of 773 advanced stage EOC patients were identified. The most predictive ≤3-year OS model was constructed using FIGO stage, tumor grade, histologic subtype, Karnofsky score, treatment approach, and residual disease after debulking. The most predictive ≥5-year OS model was constructed using FIGO stage, histologic subtype, Karnofsky score, preoperative CA-125 level, preoperative thrombocytosis, ascites volume, treatment approach, and residual disease after debulking. The most predictive ≥8-year OS model was built using the same predictors as the ≥5-year model and tumor grade. All models demonstrated good calibration and predictive accuracy with optimism-corrected AUCs of 0.71, 0.76 and 0.78, respectively.
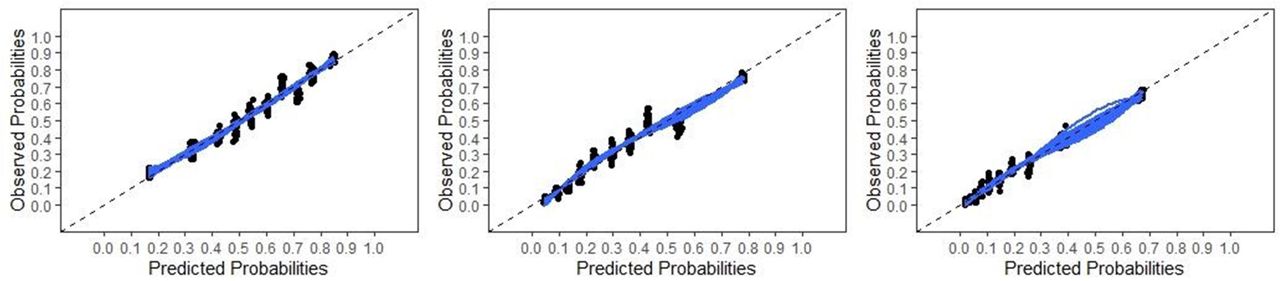
Calibration plot of the final ≤3-year (left), ≥5-year (middle) and ≥8-year (right) OS models

Online nomogram to calculate the probability towards a ≤3-year OS. Example: a FIGO stage IIIC patient who presented with high-grade serous EOC, a Karnofsky score of 80, and who underwent NACT-ICS with ≤1 cm residual disease. The nomogram predicts a probability of 70% towards a ≤3-year OS for this patient
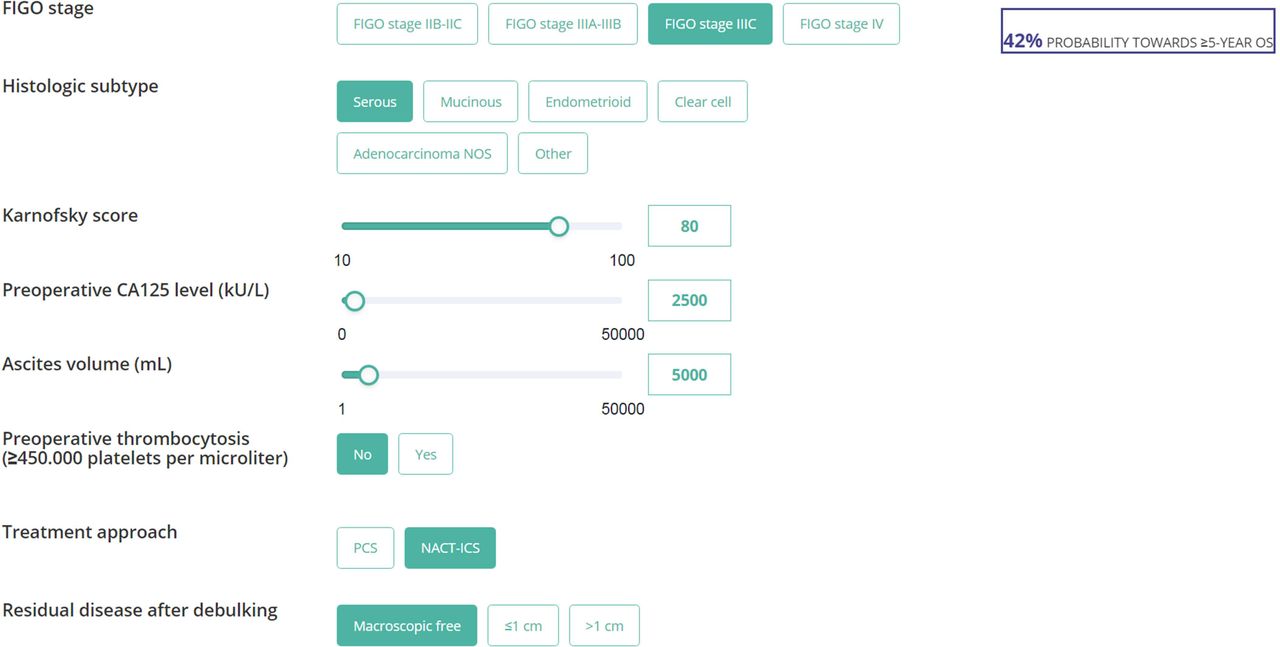
Online nomogram to calculate the probability towards a ≥5-year OS. Example: a FIGO stage IIIC patient who presented with serous EOC, a Karnofsky score of 80, preoperative CA-125 level of 2500 kU/L, ascites volume of 5L, no preoperative thrombocytosis, and who underwent NACT-ICS with no gross residual disease. The nomogram predicts a probability of 42% towards ≥5-year OS for this patient.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Online nomogram to calculate the probability towards a ≥8-year OS. Example: a FIGO stage IIIC patient who presented with high-grade serous EOC, a Karnofsky score of 80, preoperative CA-125 level of 4670 kU/L, ascites volume of 5L, preoperative thrombocytosis, who underwent NACT-ICS with no gross residual disease. The nomogram predicts a probability of 15% towards ≥8-year OS for this patient
Conclusion*Preoperative anemia and leukocytosis are not significantly independently associated with advanced EOC survival. Preoperative thrombocytosis adds to the prediction of ≥5- and ≥8-year OS of individual EOC patients. Nomograms with easily accessible factors should be useful for patient counselling, clinical trial eligibility, postoperative management, or follow up.