Article Text

Abstract
Introduction/Background*Whilst CT scanning is well established in the pre-operative staging of tubo-ovarian or primary peritoneal malignancy, studies suggest CT may be a poor predictor of diaphragmatic involvement.
Methodology All patients who underwent diaphragmatic surgery for stage III/V tubo-ovarian or primary peritoneal carcinoma in a cancer centre between 2008-2020 were identified. Pre-operative CT, operation notes and histopathology reports were reviewed retrospectively.
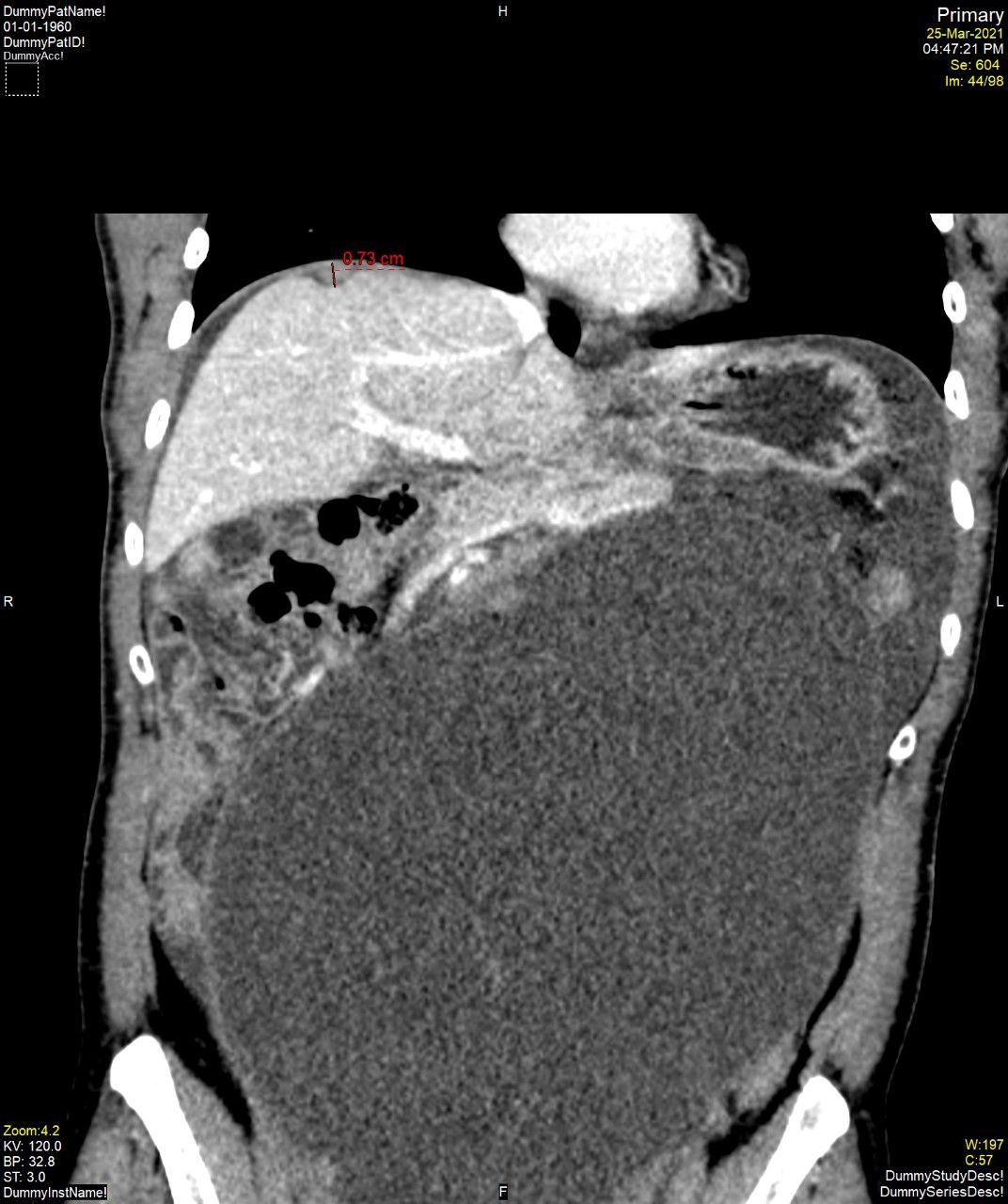
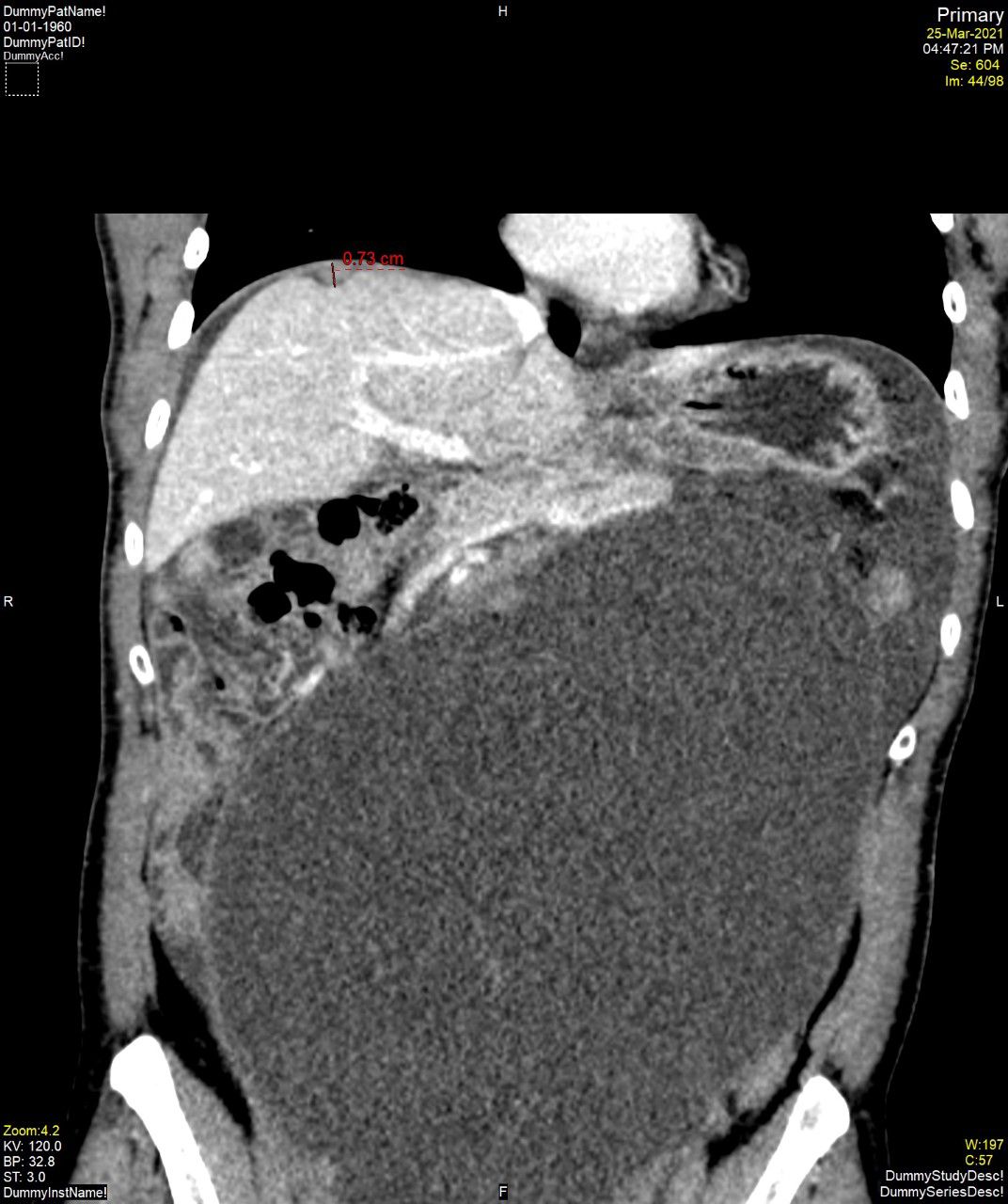
Result(s)*61 patients were identified. In 82.0% (n=50), no diaphragmatic disease was identified on pre-operative CT. This was corroborated by negative histopathology in 6 cases – equating to 9.8% true negatives, 72.1% false negatives and negative predictive value of 12%. Of those with diaphragmatic disease identified radiologically (n=11), this was confirmed on histopathology in 10 cases – equating to 16.3% true positives, 1.6% false positives and positive predictive value of 90.9%. Our data demonstrates a sensitivity of 18.5% and specificity of 85.7% for CT in diaphragmatic assessment.
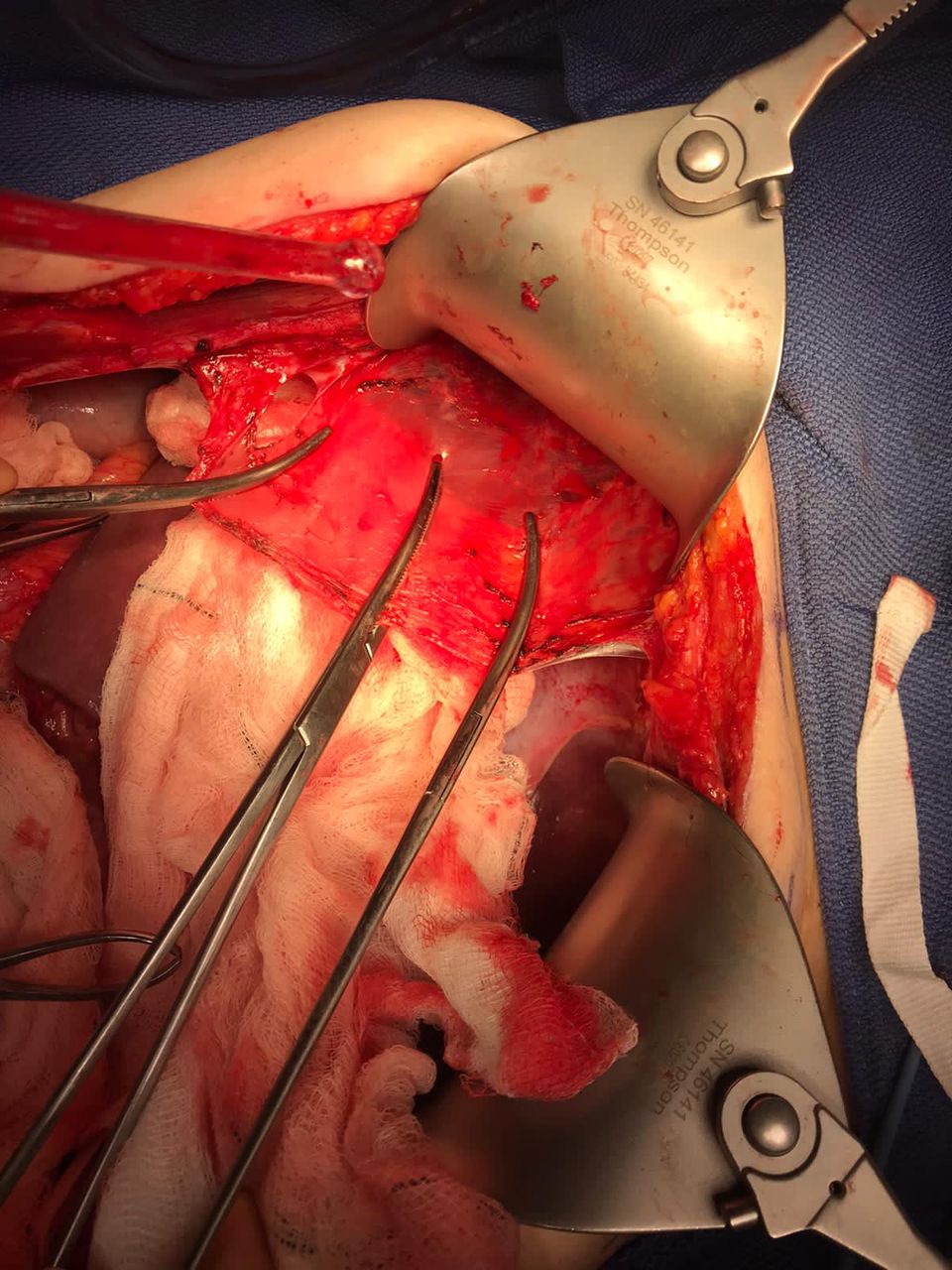
Intra-operative findings were suspicious for diaphragmatic involvement in all cases and confirmed on histopathology in 90.1% (n=55). In 6 (9.8%) patients, however, histopathology returned negative. Statistical analysis of this data was limited by the inclusion criteria – but can be interpreted as 90.2% true positives, 9.8% false positives and positive predictive value of 90.2% for intra-operative detection of diaphragmatic disease
{kind=link}
{kind=link}
Conclusion*Whilst it is accepted that CT is a poor predictor of diaphragmatic disease, we suggest our figures may be additionally compounded by a local radiological focus on identification of surgical stopping-points in the context of a unit with a well-established ultra-radical service and experience of diaphragmatic surgery. Gynaecological-oncologists should, however, remain mindful of the limitations of CT and hence approach all relevant cases with the anticipation of encountering diaphragmatic disease.