Article Text

Abstract
Introduction/Background*Malignant ovarian germ cell tumours (MOGCTs) are rare with a yearly-adjusted incidence of 3.7 per million [1] and account for 1-2% of all ovarian malignancies in Europe. There is a clinical imperative to clarify the optimal surgical approach and establish surgical radicality since this is a predominantly young population and minimising treatment morbidity and optimising future fertility is of real importance. Here we aim to describe the current surgical management of ovarian germ cell tumours and relate this to clinical outcome. Specifically, we aimed to compare outcomes of open versus laparoscopic surgery, the use of fertility-sparing approaches, surgical staging, and the potential utility of cystectomy alone in the management of patients with stage 1 immature teratoma.
Methodology A retrospective cohort study of all consecutive patients with primary ovarian germ cell tumours treated in four major UK gynaecology oncology centres over 12 years.
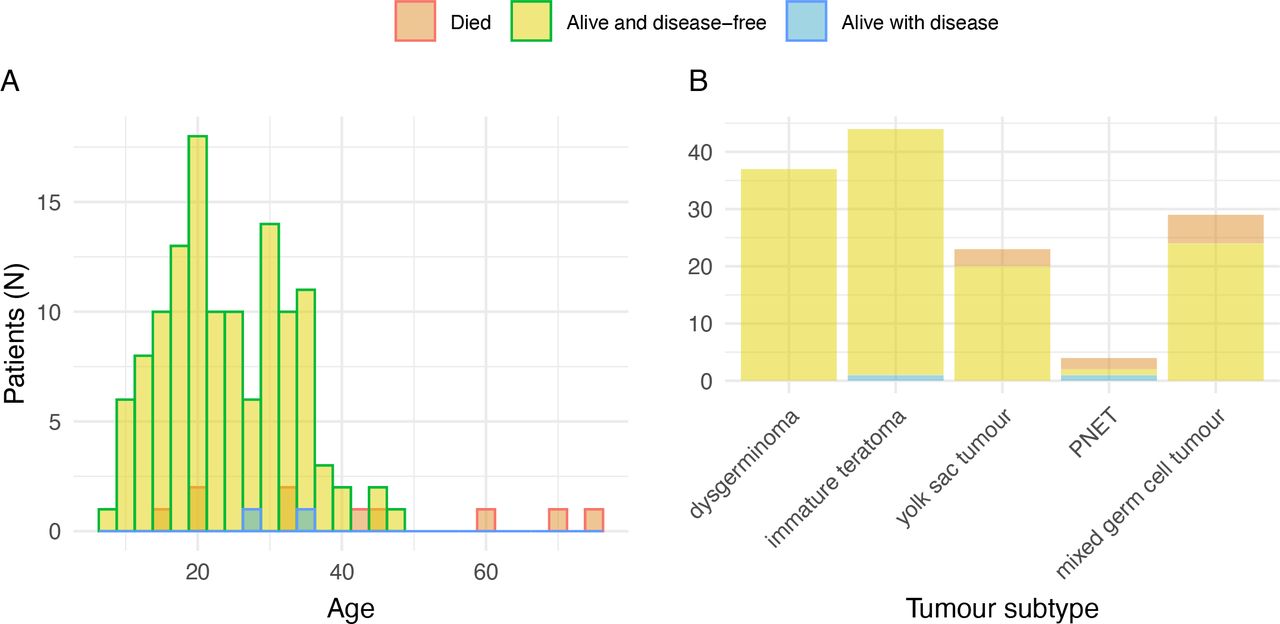
Result(s)*One hundred and thirty-seven patients were followed-up for a median of 4.6 years with a 5 year survival of 91% (95% CI 86-97%).
Open procedures were likely to be performed for larger (p<0.001) and higher stage tumours (p<0.049), but there was no significant difference in mortality between open (80% n=109) and laparoscopic approaches (16%,n=22).
Assessing the use of surgical staging in our cohort, peritoneal or omental biopsies were infrequently taken (29%, n=40) and were largely negative, returning positive results in 0% of peritoneal and 4% of omental biopsies.
In patients with stage one immature teratoma, outcomes of unilateral cystectomy only (n=9) and unilateral salpingo-oophorectomy (n=29) were compared, with no significant difference in death, recurrence rates or residual disease prevalence between the groups.
The majority (88%, n=120) of patients had fertility-sparing surgery. This was not associated with higher rates of recurrence or death than non fertility-sparing approaches.

{kind=link}
Conclusion*Laparoscopic surgery was safe and since routine staging biopsies did not alter outcome, we suggest that their use should be limited. Ovarian cystectomy may be acceptable for early-stage immature teratoma and warrants replication in other cohorts.