Article Text

Abstract
Introduction/Background*The standard treatment for advanced ovarian cancer (AOC) is cytoreduction surgery and adjuvant chemotherapy. Tumor volume after surgery is a major prognostic factor for these patients. The ability to perform complete cytoreduction depends on the extent of disease and the skills of the surgical team. Several predictive models have been proposed to evaluate the possibility of performing complete cytoreductive surgery (CCS).
Methodology External validation of the prognostic value of three predictive models (Fagotti index and the R3 and R4 models) for predicting suboptimal cytoreductive surgery (SCS) in AOC was performed in this study. The scores of the 3 models were evaluated in one hundred and three consecutive patients diagnosed with AOC treated in a tertiary hospital were evaluated. Clinicopathological features were collected prospectively and analyzed retrospectively. The performance of the three models was evaluated, and calibration and discrimination were analyzed.
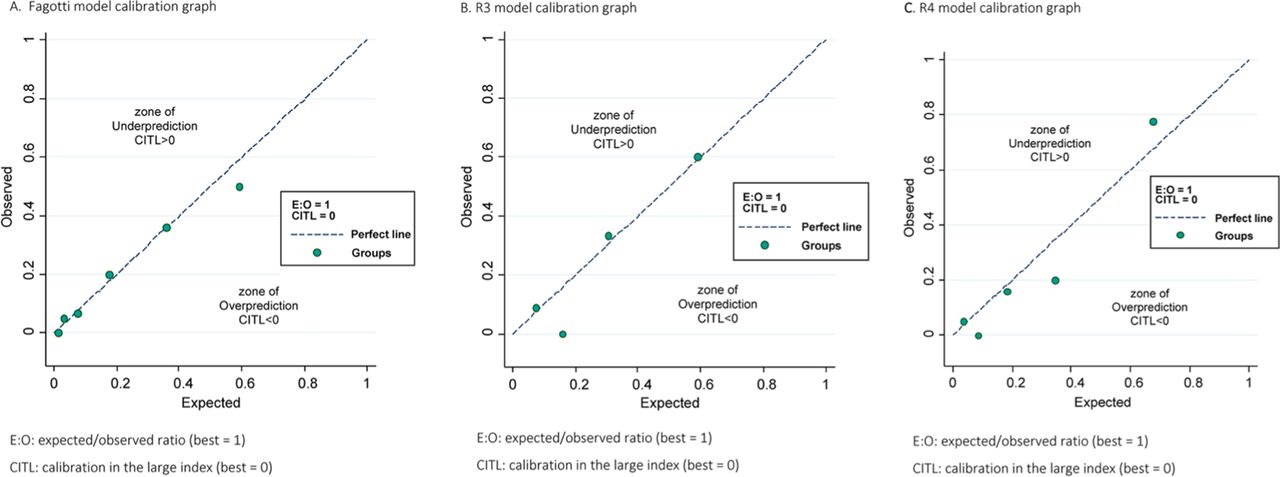
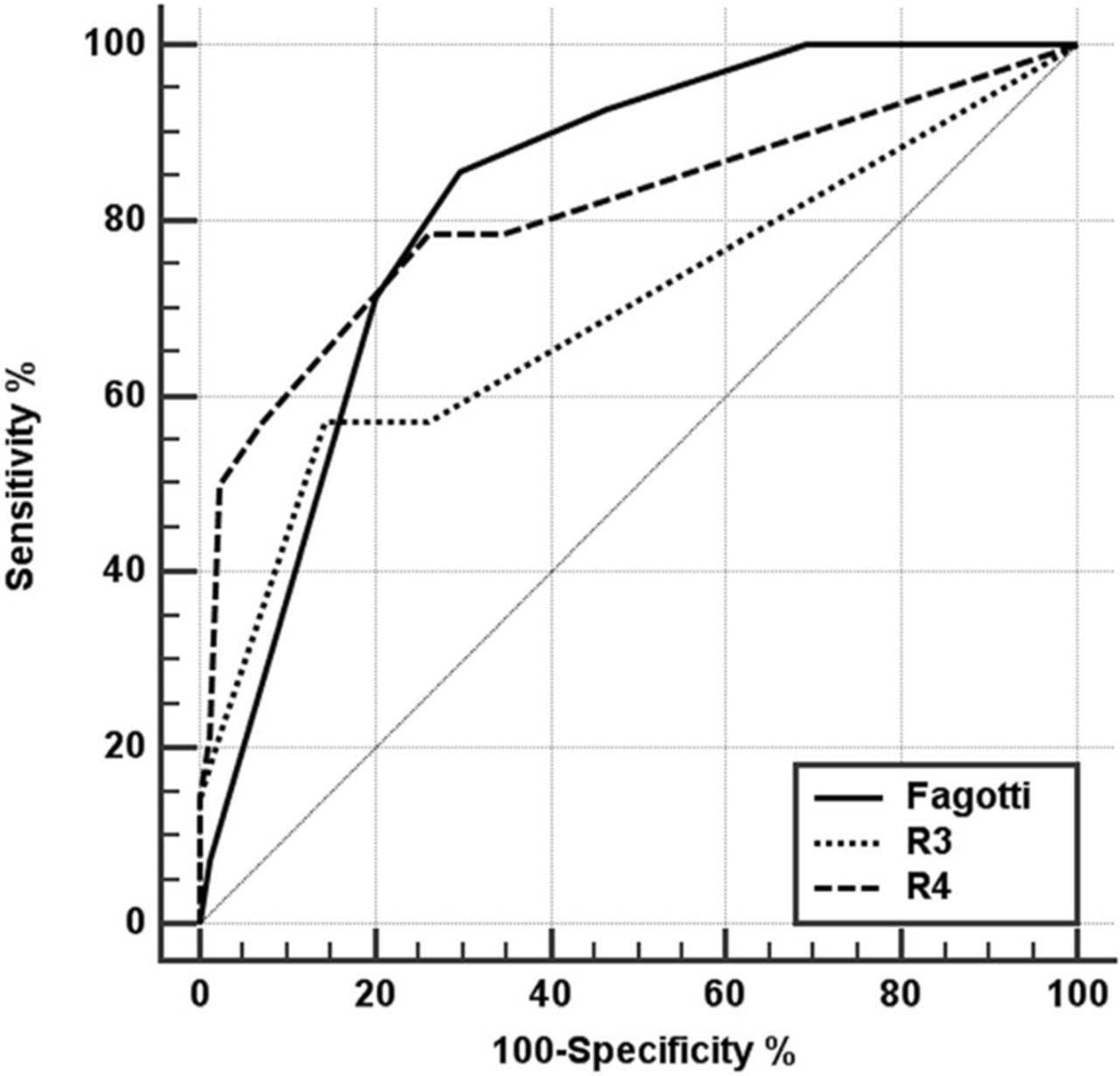
Result(s)*The calibration of the Fagotti, R3 and R4 models showed odds ratios of obtaining SCSs of 1.5, 2.4 and 2.4, respectively, indicating good calibration. The discrimination of the Fagotti, R3 and R4 models showed an area under the ROC curve of 83%, 70% and 81%, respectively. The negative predictive values of the three models were higher than the positive predictive values for SCS.

{kind=link}
{kind=link}
Comparative graph of the ROC curves for the different models
Conclusion*The three models were able to predict suboptimal cytoreductive surgery for advanced ovarian cancer, but they were more reliable for predicting CCS. The R4 model discriminated better because it includes the laparotomic evaluation of the peritoneal carcinomatosis index.