Article Text

Abstract
Introduction/Background*Debulking surgery is the mainstay of treatment for patients (pts) with advanced epithelial ovarian cancer (EOC). Upfront surgery (PDS) with complete macroscopic resection (TR0) is associated with best survival while PDS to small residual disease (TR1-10) provides moderate benefit in high grade serous OC. The impact of resection status in other histological subtypes so far has not been defined and especially the role of TR1-10 is under debate. This analysis should help to better understand the interplay between histological subtype, surgical outcome, and prognosis.
Methodology Data of patients (>FIGO IIIB) from 7 AGO-Studygroup led phase III multicentre trials (AGO-OVAR 3,5,7,9,11,12,15), (1995–2011) were pooled and analysed with focus on PDS resection status on overall survival (OS) in different histological subtypes: low grade (low grade serous or endometrioid), mucinous, clear cell, and high-grade (e.g. serous, endometrioid, undifferentiated histology). Multiple logistic regression of achieving TR0 in the full population and multiple Cox-regression of OS separately in each histological subpopulation adjusting potential confounders (treatment arm within each study, ECOG performance status, age, FIGO stage) were undertaken.
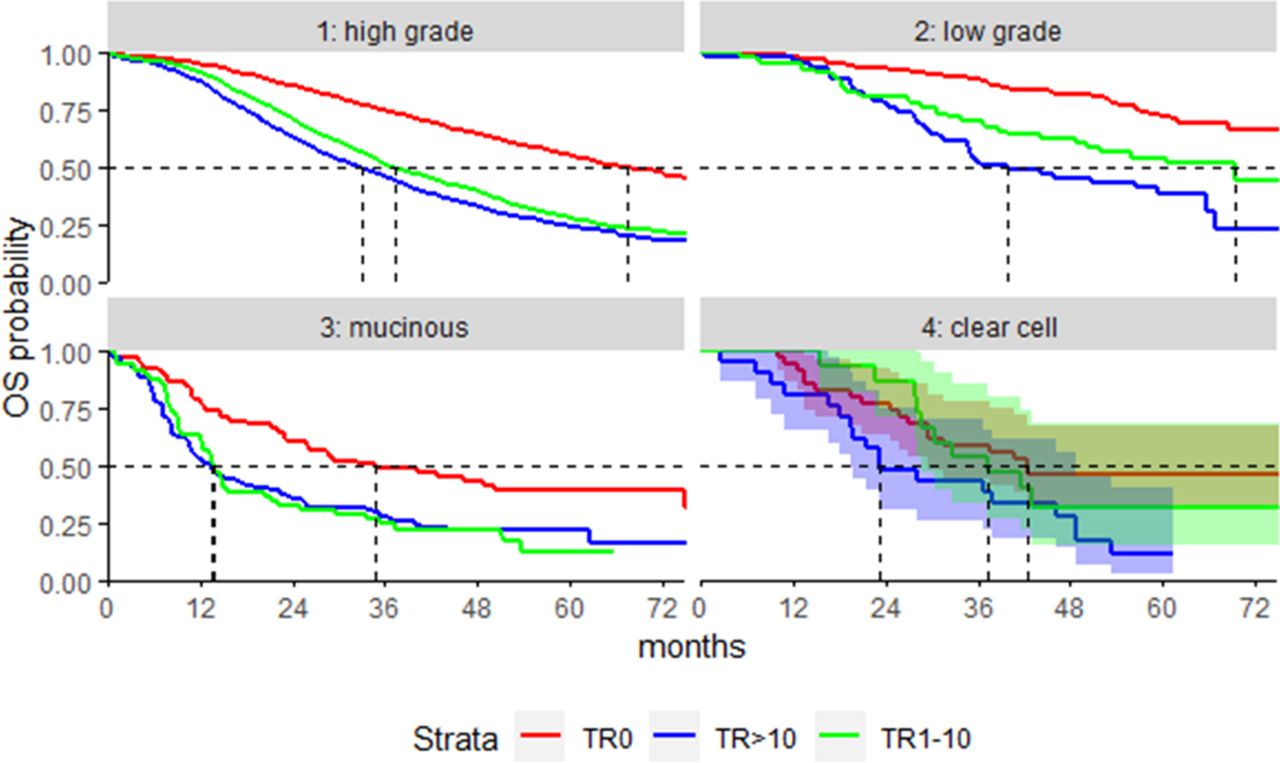
Result(s)*5,745 pts were eligible (5,156 high grade, 299 low grade, 219 mucinous, 71 clear cell). Differences in resection rates between histological subtypes are displayed in the table 1. Adjusted odds ratios showed significantly higher odds for achieving TR0 for low grade and clear cell compared to high-grade, (table 1). Median follow-up was 60.7 months. The figure shows OS within tumour types according to resection status. Hazard ratios between TR0, TR1-10 and TR>10 obtained from multiple Cox regression of OS are shown in the table 1.
OR: odds ratio; OS: overall survival; HR: hazard ratio; *number of patients included into the clear cell cohort was too small to allow meaningful OS analyses

{kind=link}
Kaplan-Meier plots of overall survival within tumour types according to complete (TR0) and largely (TR1-10mm) debulking; number of patients included into the clear cell cohort was too small to allow meaningful OS analyses
Conclusion*Our analysis confirmed the value of complete resection in all subtypes of ovarian cancer. The role of largely resection (TR1-10mm) seemed to be relevant in low grade OC, but marginal although significant in HGSOC and inconclusive in mucinous and clear cell OC. Larger databases are necessary to gain more reliable data in these subgroups.