Article Text

Abstract
Introduction/Background*In the NOVA trial of niraparib maintenance treatment (MT) in platinum-sensitive recurrent ovarian cancer (PSROC), dose reduction due to treatment-emergent adverse events (TEAEs) occurred in 66.5% of patients initiating niraparib at 300 mg. Based on NOVA RADAR analysis, subsequent individualised starting dose (ISD) recommends patients with baseline bodyweight <77 kg or baseline platelet count <150×103/µl to initiate niraparib at 200 mg and all other patients, at 300 mg. ISD was adopted in NORA (NCT03705156), the published pivotal study in Chinese patients, who generally have lower body weights than Western patients. While niraparib demonstrated acceptable safety in NORA, dose reduction remained essential and occurred in 59.9% of patients. This post hoc analysis aims to characterise the major TEAEs necessitating dose modification in NORA, to inform TEAE management in Chinese patients receiving niraparib.
Methodology In NORA, adults with PSROC and complete/partial response to most recent platinum-containing chemotherapy were randomised 2:1 to niraparib or placebo MT of 28-day cycles. Primary endpoint was progression-free survival (PFS). First 16 patients started treatment at 300 mg, before ISD was implemented. Dose interruption ≤28 days and dose reduction were permitted. Niraparib-treated patients with stabilised dosing at Cycle 4 were analysed, with descriptive statistics summarising TEAEs and descriptive PFS analysis by dose levels at the beginning of Cycle 4.
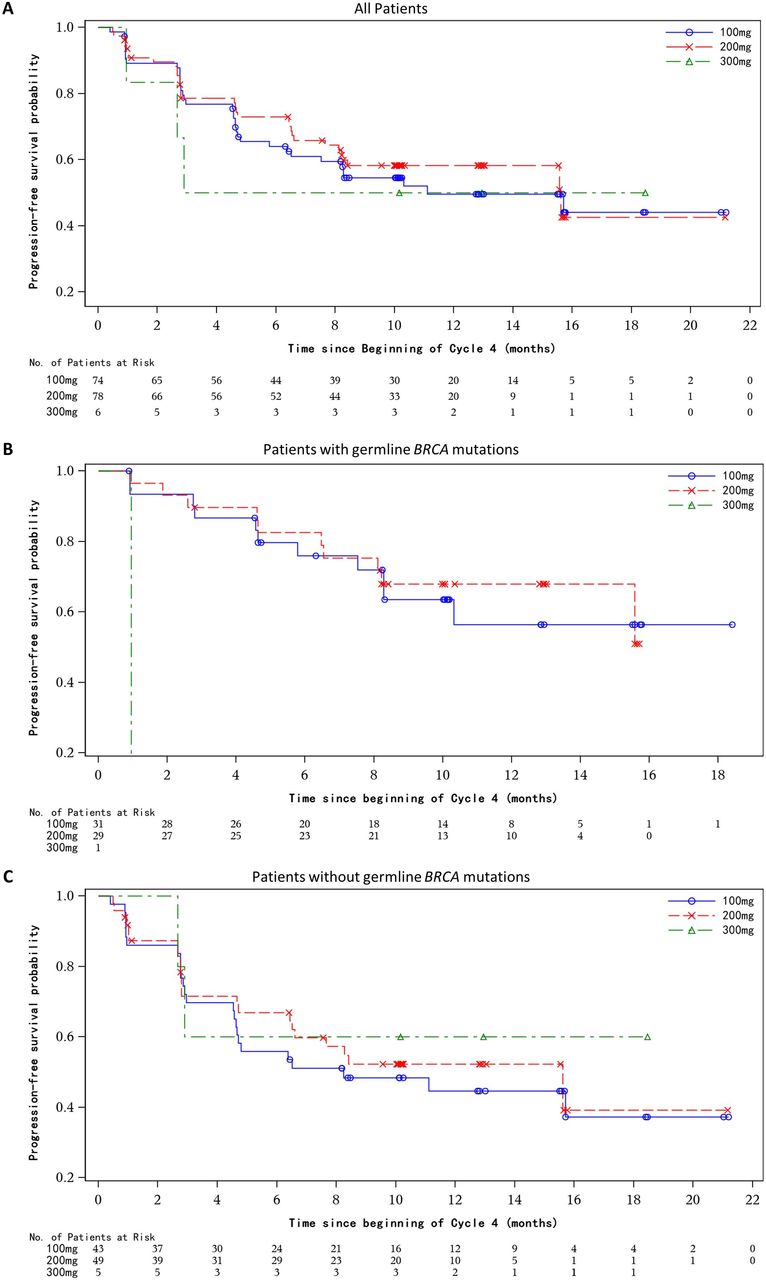
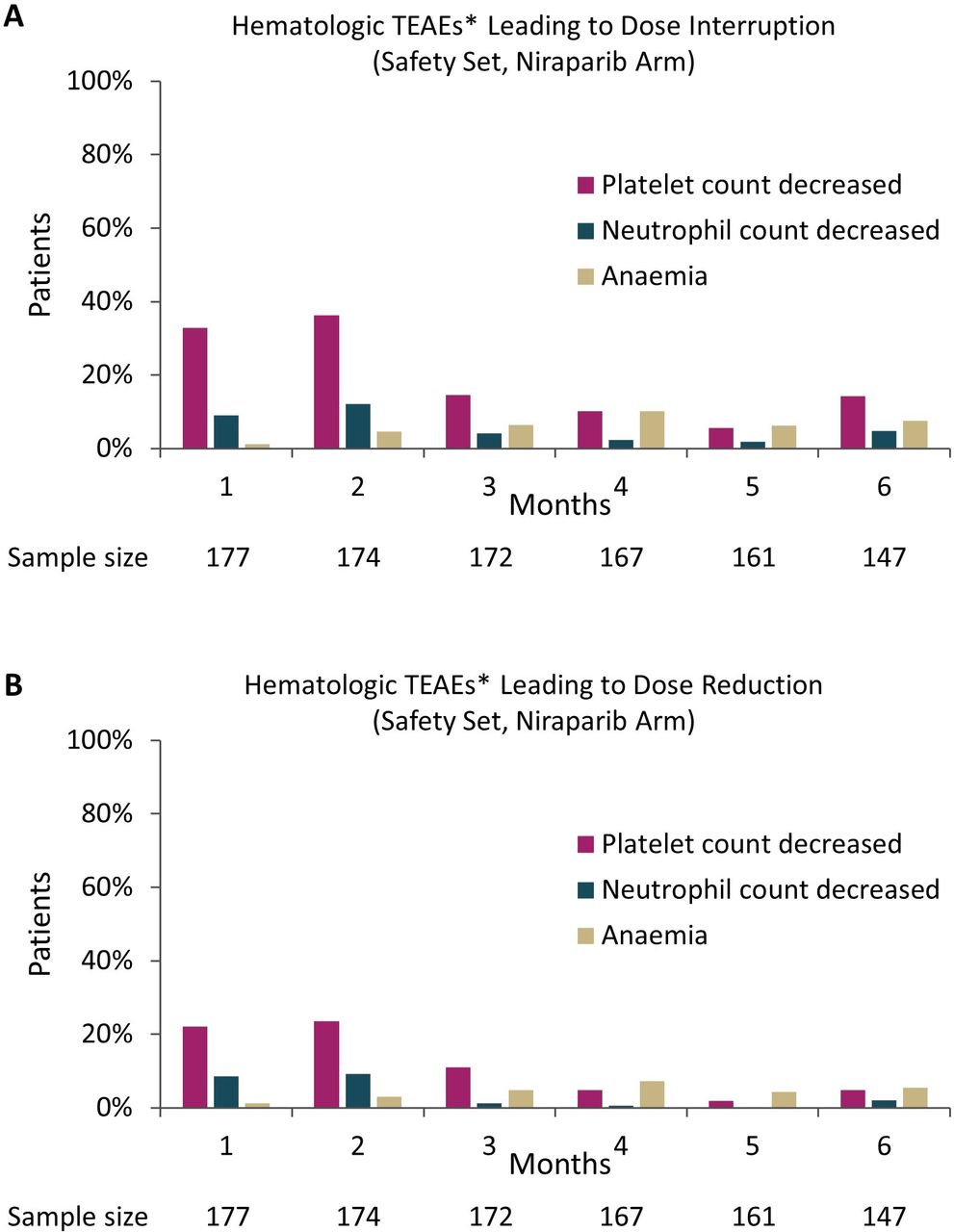
Result(s)*During Month 1/2, platelet count decrease caused dose interruption and reduction in 32.8%/36.2% and 22.0%/23.6% of patients, respectively; neutrophil count decrease caused dose interruption and reduction in 9.0%/12.1% and 8.5%/9.2% of patients, respectively. These percentages decreased from Month 3 and remained low through Months 4–6 (figure 1). Anaemia-related dose interruption/reduction occurred in ≤10% of patients. Most patients’ stabilised doses at Cycle 4 were 100 mg (n=74) or 200 mg (n=78). These two groups had comparable baseline characteristics and showed similar PFS (figure 2) from Cycle 4 onward through 12 months, regardless of germline BRCA mutation status.

Hematologic TEAEs Leading to niraparib dose interruption and reduction by month (Safety set)
{kind=link}
{kind=link}
Kaplan-meier curves for progression free survival by niraparib dose level at the beginning of cycle 4 (Intention-to-treat Set)
Conclusion*Platelet count decrease and neutrophil count decrease were the major TEAEs necessitating niraparib dose modification. Early dose modification helped maintain safety and tolerability in Chinese patients receiving niraparib MT without compromising efficacy.