Article Text

Abstract
Objective Sentinel lymph node mapping has emerged as an alternative to lymphadenectomy in evaluating the lymph node status in endometrial cancer. Several pathological methods to examine the sentinel lymph node are applied internationally. The aim of this study was to determine the value of ultrastaging and to assess the ultrastaging method with the highest detection rate of metastases.
Methods A systematic review was conducted. Inclusion criteria were: pathologically-confirmed endometrial cancer with sentinel lymph node mapping, report of the histological outcomes, metastases found by hematoxylin and eosin staining and metastases found by ultrastaging were separately mentioned, and description of the ultrastaging method. The primary outcome was the detection of metastases found by ultrastaging that were not detected by routine hematoxylin and eosin staining. The secondary outcome was the difference in detection rate of metastases between several ultrastaging methods. Random effects meta-analyses were conducted.
Results Fifteen studies were selected, including 2259 patients. Sentinel lymph nodes were examined by routine hematoxylin and eosin staining. Subsequently, multiple ultrastaging methods were used, with differences in macroscopic slicing (bread-loaf/longitudinal), number of microscopic slides, and distance between slides, but all used immunohistochemistry. A positive sentinel lymph node was found in 14% of patients. In 37% of these, this was detected only by ultrastaging. Using more ultrastaging slides did not result in a higher detection rate. Bread-loaf slicing led to a higher detection rate compared with longitudinal slicing (mean detection rates 53% and 33%, respectively).
Conclusion Pathological ultrastaging after routine hematoxylin and eosin staining in endometrial cancer patients has led to an increased detection rate of sentinel lymph node metastases. Different ultrastaging methods are used, with a preference for bread-loaf slicing. However, due to the large heterogeneity of the studies, assessing which ultrastaging method has the highest detection rate of sentinel lymph node metastases was not possible.
- gynecologic surgical procedures
- pathology
- endometrial neoplasms
Statistics from Altmetric.com
Introduction
Endometrial cancer is the most common gynecological cancer in western countries, with an age-standardized incidence rate of about 20 per 100 000 women. Most women are diagnosed at an early stage, in which the cancer is limited to the uterus. In these women, a favorable 5-year survival of up to 87%–96% is seen, depending on the grade of the tumor (low-risk vs intermediate- and high-risk).1 However, even in presumed early-stage endometrial cancer, lymph node metastases are seen in 10%–15% of the patients.2 Standard treatment of endometrial cancer consists of surgery. In most countries, the need for adjuvant therapy is based on a risk assessment. This risk assessment includes factors such as age, histological subtype, and myometrial invasion. However, the presence of lymph node metastases is the most important risk factor in endometrial cancer. Studies showed that the 5-year survival of endometrial cancer is negatively influenced when lymph node metastases are found.3–8
There are several ways to assess lymph nodes. One way is by performing a lymphadenectomy. However, there is a lack of evidence for the improvement of survival in patients with early-stage low-risk endometrial cancer, while a lymphadenectomy increases complications such as lymphedema.9–11 These results have been discussed in light of studies demonstrating that lymphadenectomy is associated with longer overall survival for patients with intermediate- or high-risk endometrial cancer, however, this did not take into account the contribution of sentinel lymph node biopsy in improving metastasis detection through ultrastaging. Therefore, adding sentinel lymph node mapping to primary surgery, instead of a complete lymphadenectomy, might improve identification of patients at risk, while minimizing complications.
Recent studies have shown that sentinel lymph node mapping has a high sensitivity and specificity in patients with endometrial cancer.12 Besides, performing the sentinel lymph node procedure leads to a higher stage of disease (upstaging) in 14% of presumed low- and intermediate risk endometrial cancer patients and in 30% of high-risk endometrial cancer patients, especially when pathological ultrastaging to the sentinel lymph node specimen was applied (43% of metastases undiagnosed by conventional histology were detected by ultrastaging).2 13–15 Histological examination of lymph nodes is traditionally performed with one longitudinal cross-section through the lymph node with subsequent hematoxylin and eosin stain of the two cut surfaces. Ultrastaging of sentinel lymph nodes involve additional serial sectioning with review of multiple hematoxylin or eosin staining slides with or without immunohistochemistry.
Ultrastaging might improve the detection rate of metastases, especially of low-volume metastases such as micrometastases (size >0.2 mm and ≤2 mm) and isolated tumor cells (solitary tumor cells or tumor cell clusters≤0.2 mm).16–22 In the previous literature on endometrial cancer and ultrastaging, different ultrastaging protocols were applied, without a valid standardized routine protocol.23 The primary aim of this systematic review was the detection rate of metastases in women with endometrial cancer, found by ultrastaging, that were not detected by routine hematoxylin and eosin staining. The secondary aim was to examine differences in the detection rate of metastases between several ultrastaging methods.
Methods
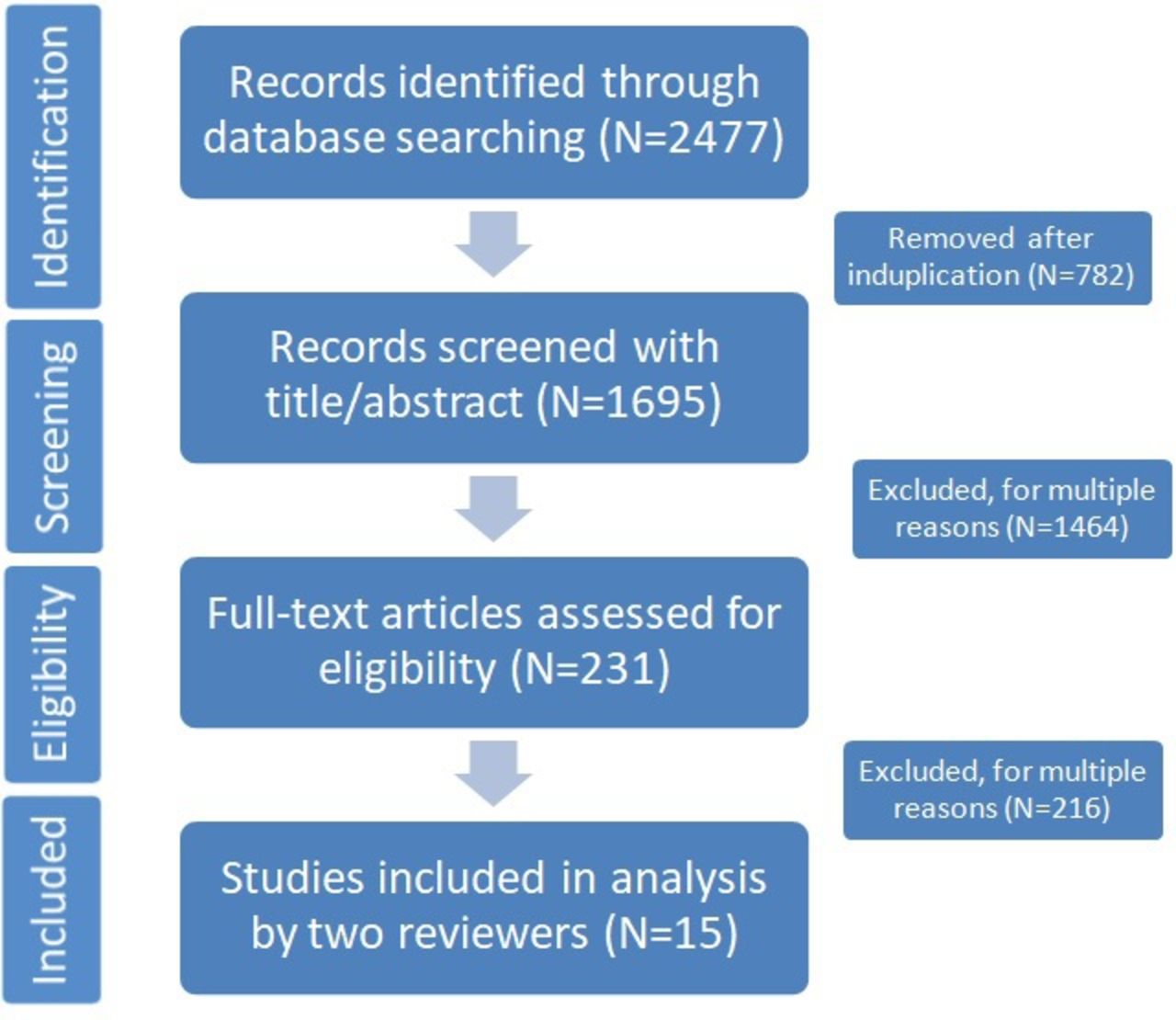
This study was conducted by following the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement.24 A summary of the literature search and study selection is depicted in Figure 1.
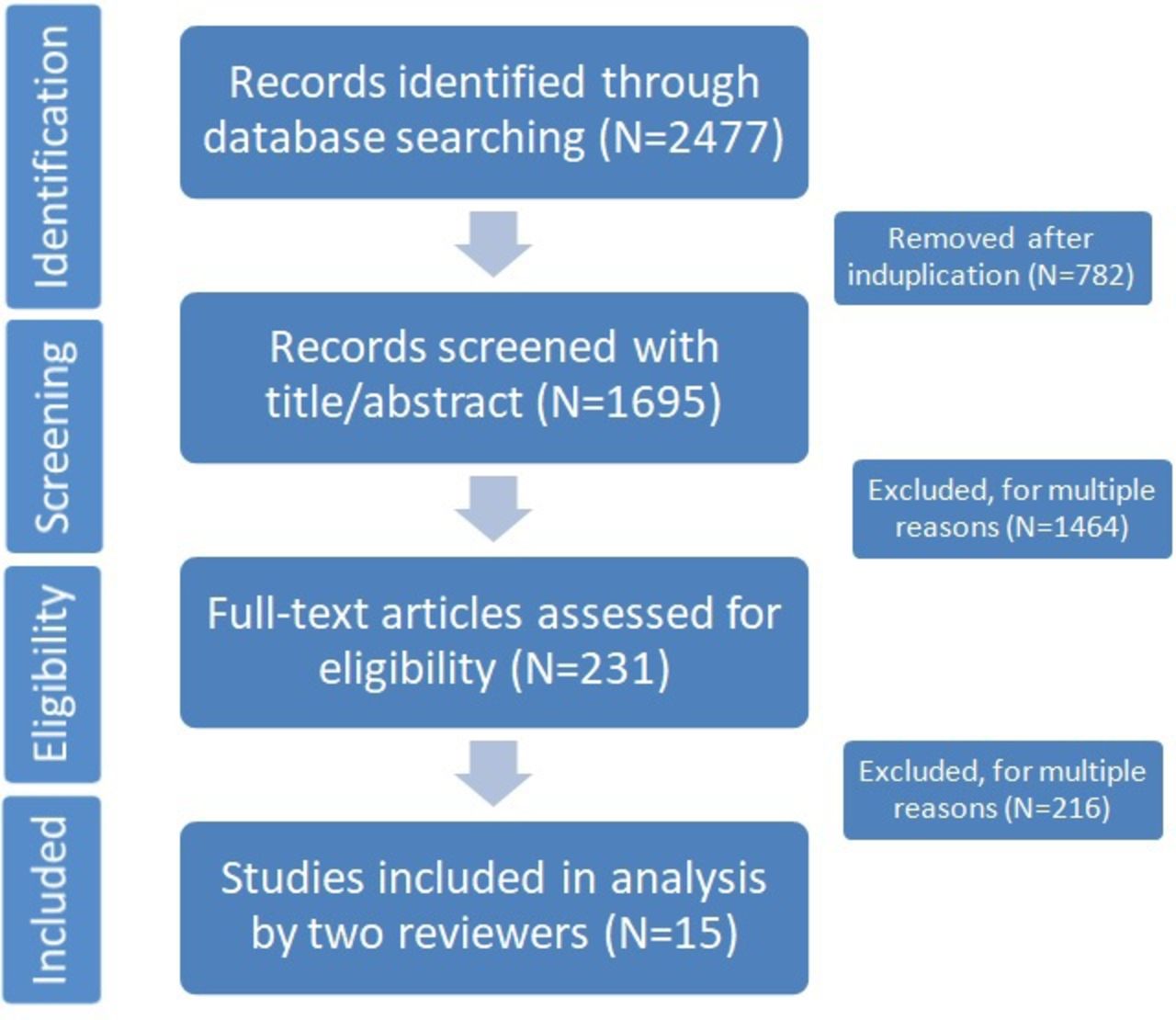
Summary of literature search and selection. All processes were conducted by two independent reviewers (LB/EH). Excluded after assessment for eligibility of full-text article: n=215. Reasons for exclusion: lack of description of ultrastaging technique; results were not specified into routine hematoxylin and eosin staining vs immunohistochemistry; data was based on multiple previous studies.
Search Strategy
A systematic search using electronic databases was performed on October 2020, using the following search engines: MEDLINE, EMBASE, Web of Science, and the Cochrane Library. We did not filter the results on year of publication: all studies published up until the date of the search were taken into account. The search query combined synonyms, including multiple MeSH-terms, for endometrial cancer, lymph node metastases, staining, and ultrastaging. Furthermore, text words were combined to search for relevant literature. We also performed a reference and related article search. A total of 2477 articles were identified through database searching. Duplicated articles were filtered by using ENDNOTE X8. After removal of duplicate records, titles and abstracts of the studies were reviewed (1695 records). In cases where an accurate judgment for inclusion was difficult, the original document was assessed by applying the selection and eligibility criteria. A total of 231 records were assessed for eligibility.
Eligibility Criteria
Studies were included when the following criteria were met: study on pathologically-confirmed endometrial cancer with sentinel lymph node mapping performed; histological outcomes were reported, including reporting metastases found by hematoxylin and eosin staining, and metastases found by immunohistochemistry only; description of the applied ultrastaging technique, including the number of slices made, the type of staining used, and the interval between slices when serial sectioning was applied; data of the study was not based on multiple included studies; full study was available, abstracts only were excluded; studies obtained research ethics approval; and language was restricted to English. Studies in which the frozen section of the sentinel lymph node was applied were included if ultrastaging was performed as well after the frozen section.
Study Selection and Data Extraction
We selected 15 peer-reviewed and published studies that met the eligibility criteria. (Table 1)25–39 The most common reason for exclusion of the other studies was the lack of a description of the ultrastaging technique (Figure 1). Another reason for exclusion was that results were not specified into routine hematoxylin staining vs immunohistochemistry, or because data was based on multiple previous studies. Data extraction of the 15 records included author, year of publication, study design, study population, operation technique, sentinel lymph node mapping, definition of metastases, routine hematoxylin and eosin staining procedure, ultrastaging procedure, and outcomes of staging (Table 1). The current definition of macrometastases (>2 mm), micrometastases (>0.2–2 mm), and isolated tumor cells (solitary tumor cells or tumor cell clusters≤0.2 mm) was used in all studies. The eligibility of all articles was independently assessed by two reviewers (LB/EH). When in doubt, a third or fourth person (PZ/PB) was consulted. No unpublished material was included.
Baseline information of included studies with sentinel lymph node procedure in endometrial cancer
Quality Assessment
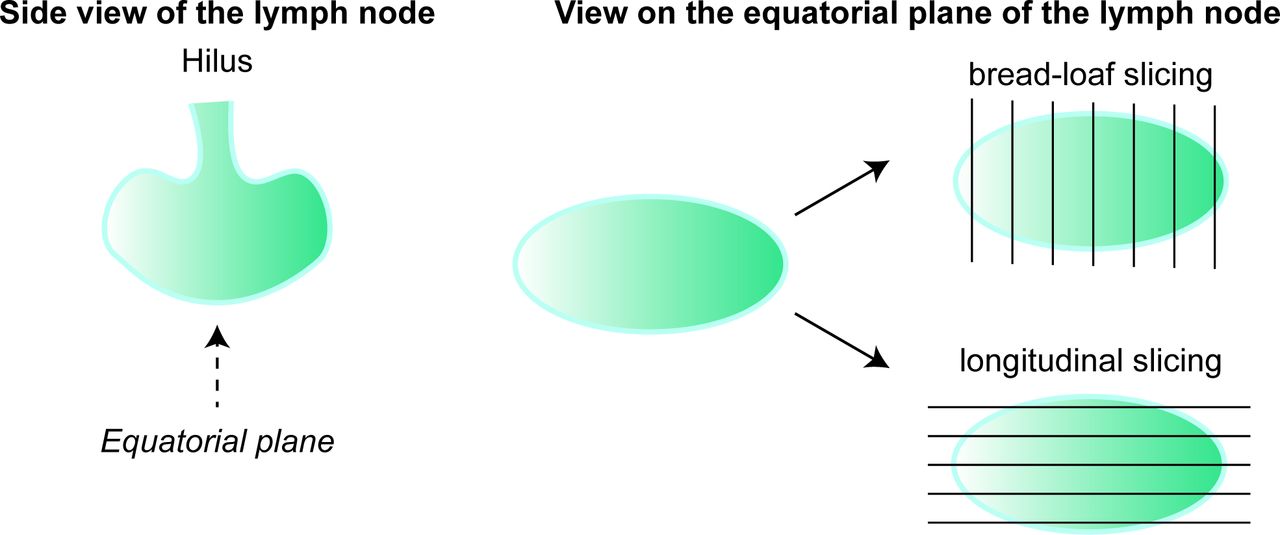
The quality of the selected studies was evaluated using the Quality Assessment of Diagnostic Accuracy Studies-2 (QUADAS-2) tool (online supplemental figures 1; 2).40 The QUADAS-2 is a tool for quality assessment determining the risk of bias and the applicability. The risk of bias is based on four domains: patient selection, index test, reference standard, and flow and timing. Patient selection, index test, and reference standard are also assessed for applicability concerns. The QUADAS-2 assessment was conducted by two independent reviewers (LB/EH): in case of not matching opinions, consensus was reached for all cases after mutual discussion. Not displayed in Online supplemental figure 1, but of importance regarding various biases, is the heterogeneity of the included studies. This heterogeneity consists of differences in ultrastaging variables between the records (eg, macroscopic slicing, number of microscopic slides, interval between slides, ultrastaging staining). Because of this heterogeneity we decided to focus on the slicing method, the number of intervals, and the staining technique, instead of more pathological characteristics such as thickness of slides. Bread-loaf slicing means slicing the lymph node perpendicular to the longest axis of the lymph node and longitudinal slicing means slicing the lymph node along the equatorial plane of the lymph node (Figure 2).
Supplemental material
Supplemental material

Explanation of bread-loaf and longitudinal slicing of a lymph node.
Statistical Analyses
Random-effects meta-analyzes were conducted to estimate the mean proportion of patients with a positive sentinel lymph node, found by hematoxylin and eosin staining and immunohistochemistry, together and separately. The meta-analyzes were conducted using the inverse variance method, the DerSimonian–Laird estimator for tau,2 the HKSJ adjustment, and an arcsine transformation of the proportions.41 The estimates of the mean proportions of patients with a positive sentinel lymph node were based on all studies and in addition – to check robustness of the results – based on the larger studies: once for studies with at least 50 patients. Subgroup analyzes were conducted to investigate the effect of the number of microscopic slides (one vs more than one slide), and the effect of the type of microscopic slides, based on two subgroups: bread-loaf or longitudinal macroscopic slicing. Proportions of patients with positive sentinel lymph nodes in individual studies were presented with Clopper–Pearson confidence intervals. Analyzes were conducted with the statistical software R version 3.5.3, using the ‘metafor' package (version 2.1–0) and 'meta' package (version 4.9–7).42–44 An extra analysis to examine an association between the presence of risk factors (grade, myometrial invasion, lymphovascular space invasion) and the presence of sentinel lymph node metastases was performed.
Results
After removal of duplicate records, the titles and abstracts of 1695 articles were screened. In 231 of these, the title and abstract were considered to be sufficiently contributory, and those articles were assessed for eligibility. In total, 216 of 231 articles were then excluded for multiple reasons, most of them because of a lack of description of the ultrastaging technique. Another reason for exclusion was that the results were not specified into routine hematoxylin and eosin staining vs immunohistochemistry, or because data was based on multiple previous studies (Figure 1).
A total of 2783 patients with endometrial cancer in 15 studies were included. All patients underwent a hysterectomy with bilateral salpingo-oophorectomy and sentinel lymph node mapping. In five studies (33%), blue dye (isosulfan blue dye, methylene blue dye, patent blue dye) was used during sentinel lymph node mapping. Indocyanine green (ICG) was used in two studies (13%). One study used blue dye with or without technetium (7%). Six studies used a combination of blue dye with technetium (40%). One study used several protocols (patent blue with technetium, patent blue alone, ICG, or technetium alone). A pelvic lymphadenectomy was performed in all studies, whereas a para-aortic lymphadenectomy was performed in only two studies (422 patients). A total of 522 patients were excluded because of a variety of reasons, mostly (77%) due to the inability to detect a sentinel lymph node, leading to a total number of 2261 patients remaining.
Incidence of Sentinel Lymph Node Metastases
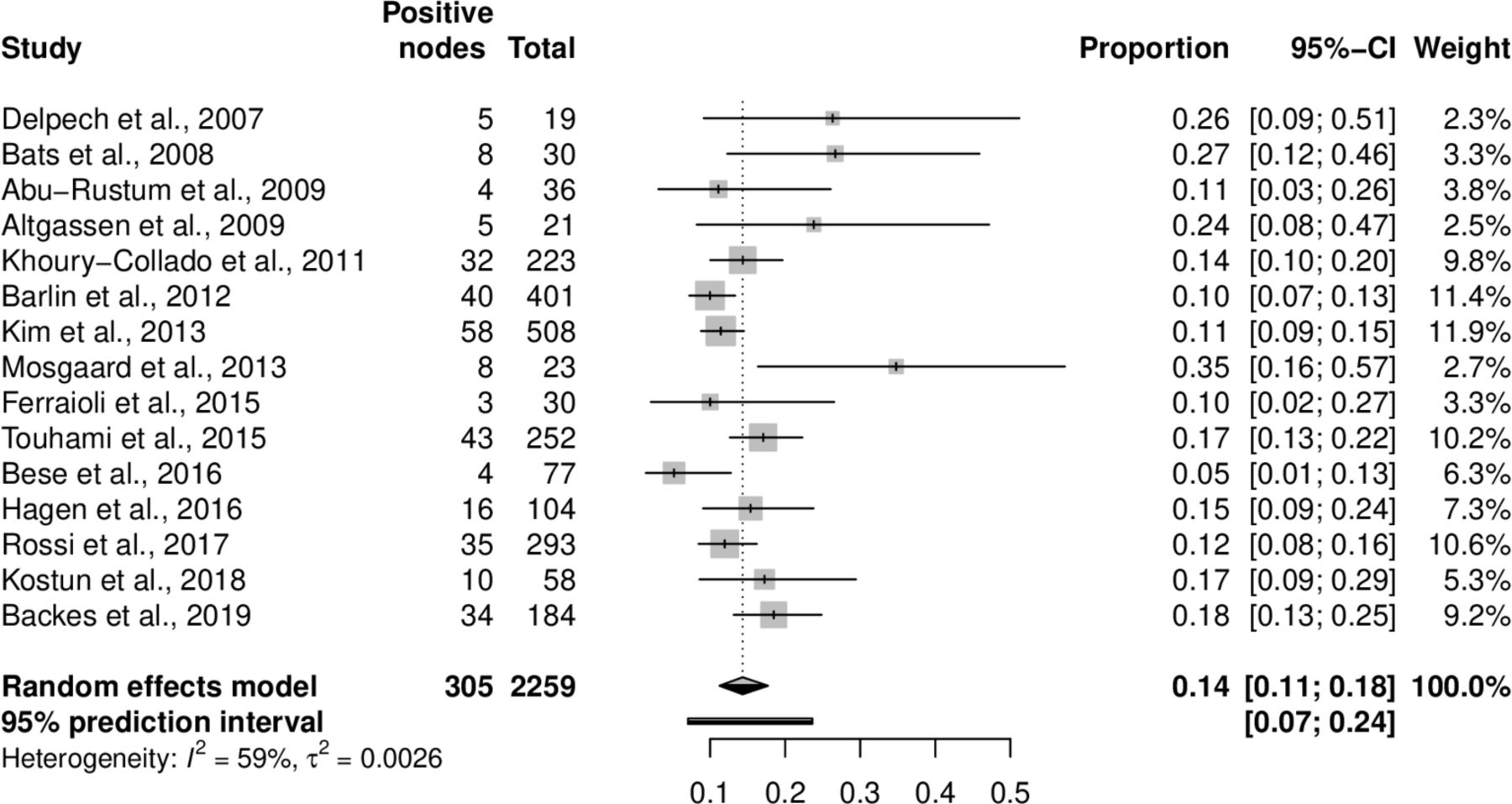
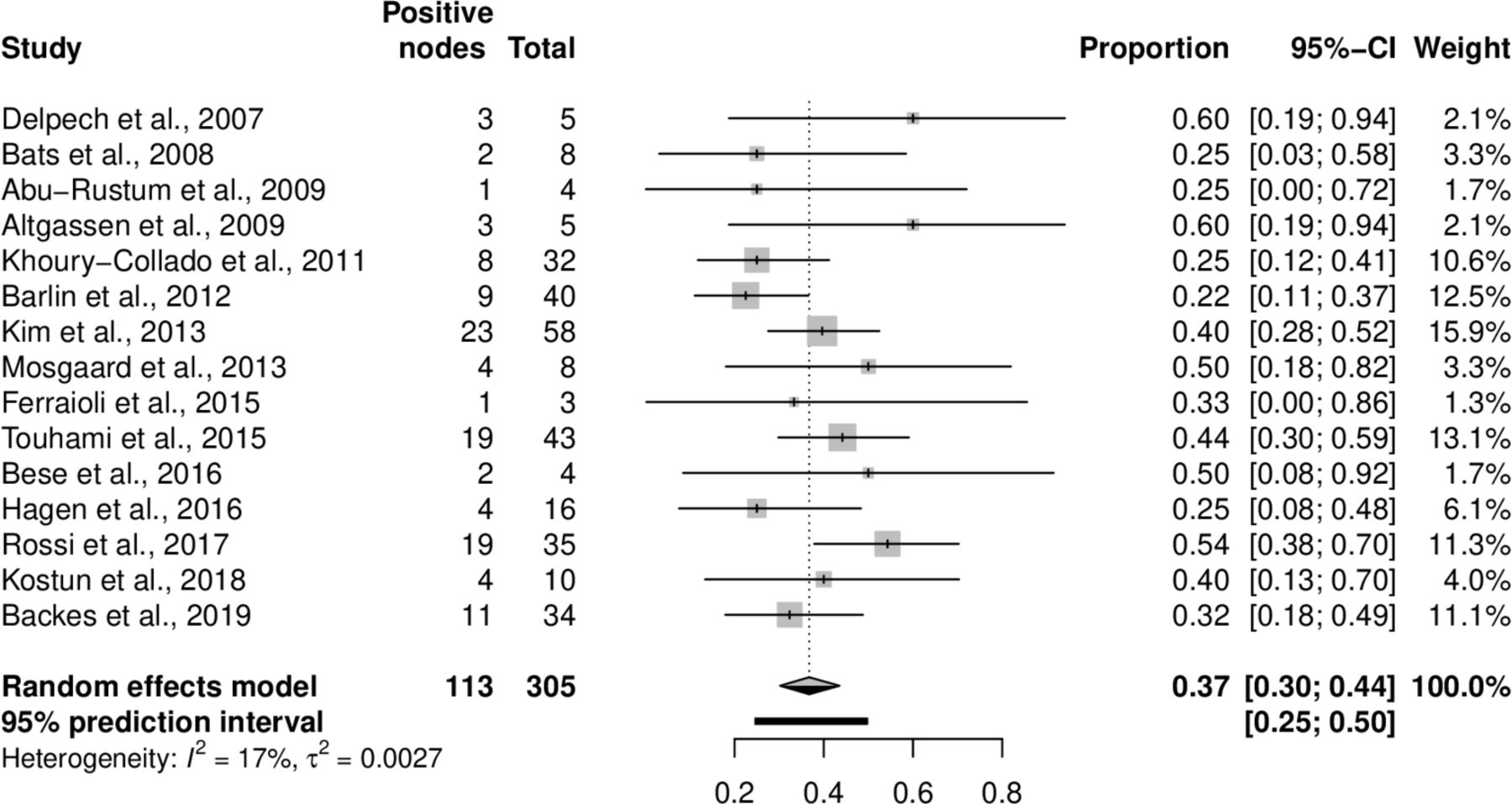
In the remaining 2259 patients (of whom 76% had endometrioid adenocarcinoma, n=1713), on average 14% (n=305) had a positive sentinel lymph node (macro- and micrometastases, isolated tumor cells) detected during histopathological evaluation (95% CI: 11% to 18%, Figure 3). Figure 3 shows an I2 of 59%, representing ‘Mod heterogeneity’. The I2 is a measure of observed heterogeneity in a meta-analysis. On average 37% (n=113) of these patients with positive sentinel lymph nodes, metastases (solely micrometastases and isolated tumor cells) were only detected during ultrastaging after routine hematoxylin and eosin staining (95% CI: 30% to 44%, Figure 4). Sensitivity analyzes including only studies with 50 patients or more showed comparable outcomes: 13% (95% CI: 10% to 16%) of all patients had sentinel lymph node metastases, and in 36% (95% CI: 27% to 45%) of those patients, the metastases were found by ultrastaging only, after hematoxylin and eosin staining (online supplemental figures 3; 4).
Supplemental material
Supplemental material

Number of patients with a positive sentinel lymph node, detected during histopathological evaluation in general (including routine hematoxylin and eosin staining, followed by ultrastaging).
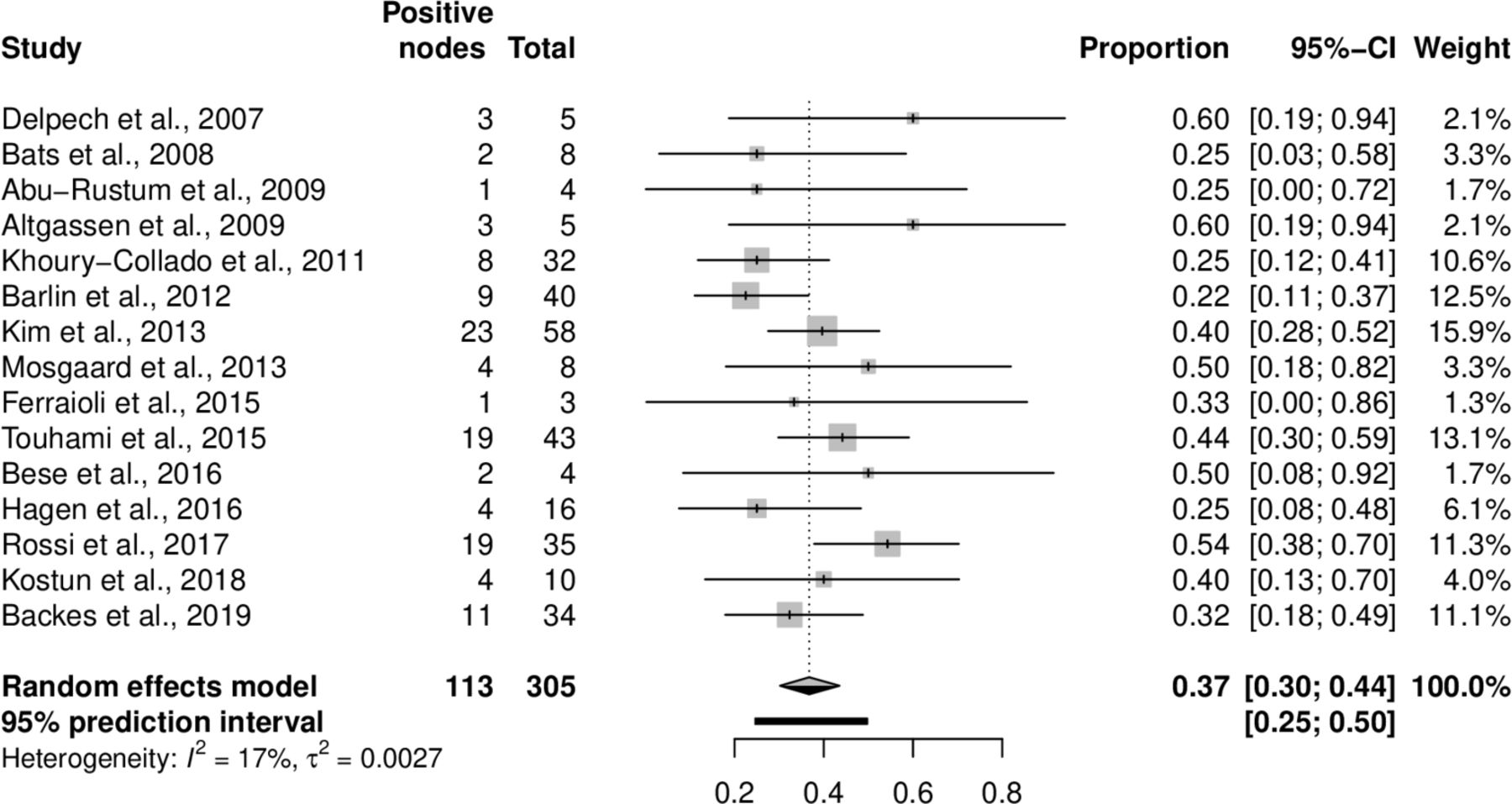
Number of patients with a positive sentinel lymph node detected by ultrastaging (including immunohistochemistry), that were not detected by hematoxylin and eosin staining.
Difference in Detection Rate Between Ultrastaging Methods
The 15 included studies that used a range of different pathological protocols for assessing the sentinel lymph nodes. The differences were mainly found in the way of macroscopic slicing (bread-loaf or longitudinal), the intervals used in case of serial sectioning (interval 50–250 µm and once three sections per mm), and the use of and number of slides used for ultrastaging (number of slides 1–6). In all included studies, the ultrastaging protocol included additional immunohistochemistry testing, using the anti-cytokeratin antibody cocktail cytokeratin AE1–AE3. The different methods used in the studies are described in detail in Table 1.
Using more than one slide for immunohistochemistry during ultrastaging did not result in a higher detection rate of sentinel lymph node metastases. The detection rate was 47% (95% CI: 31% to 63%) when one slide was used, and 32% (95% CI: 26% to 39%) if more than one slide was used for immunohistochemistry (P<0.05, Figure 5). The macroscopic slicing method was influenced by the number of metastases found with immunohistochemistry. In immunohistochemistry, using macroscopic bread-loaf slicing led to a higher detection rate of metastases (micrometastases and isolated tumor cells) than longitudinal slicing, with average metastases detection rates of 53% (95% CI: 41% to 64%) and 33% (95% CI: 27% to 40%), respectively (P<0.05, Figure 6). There was no association between the presence of risk factors (grade, myometrial invasion, lymphovascular space invasion) and the presence of sentinel lymph node metastases (data not shown). Sensitivity analyzes including only studies with 50 patients or more showed comparable outcomes, with reduced significance (online supplemental figures 5; 6).
Supplemental material
Supplemental material

Detection rate of metastases in a sentinel lymph node, based on number of slides for ultrastaging (including immunohistochemistry), P=0.0154.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Detection rate by ultrastaging (including immunohistochemistry) detected metastases in a sentinel lymph node, based on macroscopical slicing (bread-loaf vs longitudinal).
Discussion
The primary aim of this systematic review was to determine the added value of ultrastaging of the sentinel lymph node in endometrial cancer. We showed that ultrastaging leads to an increased detection rate of sentinel lymph node metastases, since 37% of the positive sentinel lymph nodes would not have been found if ultrastaging was not applied, that is, with routine hematoxylin and eosin staining alone. Second, we have tried to examine differences in the detection rate of sentinel lymph node metastases between several ultrastaging methods, in order to find the ultrastaging method with the best detection rate. Although different ultrastaging protocols were used, our systemic review favors the bread-loaf slicing technique with one slide used for ultrastaging as the most effective one to detect sentinel lymph node metastases.
To achieve the ultrastaging method with the best detection rate of metastases in the sentinel lymph node is paramount. Lymph node metastases occur in approximately 5% of presumed low-, 12% of presumed intermediate-, and up to 30% of presumed high-risk endometrial cancer patients.14 45 It is not yet known if sentinel lymph node mapping and, consequently, adjuvant therapy, when a positive sentinel lymph node is found, impacts disease-free and overall survival.46 The presence of micro- and macrometastases, however, predicts the involvement of non-sentinel lymph nodes in endometrial cancer and is associated with worse outcome in comparison to node-negative endometrial cancer.39 The clinical significance of isolated tumor cells is uncertain: survival of patients with isolated tumor cells resembles survival of node-negative patients.47 48 The Society of Gynecologic Oncology’s (SGO) Clinical Practice Committee and SLN Working Group published consensus recommendations on sentinel lymph node mapping in endometrial cancer in 2017, recommending the performance of sentinel lymph node mapping in low- and intermediate-grade endometrioid adenocarcinoma instead of routine pelvic lymphadenectomy.49 For high-grade endometrial cancer, the Society of Gynecologic Oncology considers sentinel lymph node mapping as a possibility, but more information regarding the safety and efficacy is necessary.49 For histopathological evaluation, the Society of Gynecologic Oncology recommends routine hematoxylin and eosin staining with ultrastaging (serial sectioning with immunohistochemistry), to increase the detection of isolated tumor cells and micrometastases.
As our study shows, multiple techniques for ultrastaging have been used, and techniques were often not well or incompletely described, making it difficult to assess the superior technique of ultrastaging. We showed a preference for the bread-loaf slicing technique with one slide used for ultrastaging, however, the large heterogeneity in the studies included and the absence of randomized controlled trials, leads to various biases. The same issue has been described in other cancers as well. In melanoma and breast cancer, sentinel lymph node mapping has been part of standard care for a much longer period of time than in endometrial cancer, but there is still no standardized approach regarding histopathological evaluation of the sentinel lymph node in these cancers. Several authors recommend a standard protocol to achieve uniform practice.50–52 Multiple attempts have been made, however uniformity has not been achieved. For instance, The British Royal College of Pathologists described the bread-loaf slicing technique to be equally sensitive in identifying nodal disease compared with the longitudinal slicing technique. The EORTC trial protocol, however, opted for a longitudinal slicing technique in general.53 The previously mentioned Society of Gynecologic Oncology consensus recommendations do not suggest a specific or superior ultrastaging technique.49 The NCCN guidelines currently recommend ultrastaging of SLNs which involve serial sectioning of nodes at finer cuts, and performing immunohistochemistry for cytokeratin on hematoxylin and eosin negative slides.
To the best of our knowledge this is the first study to systematically assess multiple ultrastaging techniques in sentinel lymph node mapping in endometrial cancer. A previous study by Euscher et al, compared two ultrastaging protocols of sentinel lymph node in endometrial cancer.54 After longitudinal slicing in 2 mm intervals and routine hematoxylin and eosin processing, negative sentinel lymph nodes were ultrastaged by one of the following methods: five hematoxylin and eosin levels at 250 µm intervals with two unstained slides at each level; pankeratin immunohistochemistry (immunohistochemistry) performed on level 1 in cases with negative hematoxylin and eosin levels; one hematoxylin and eosin level +2 unstained slides cut 250 µm into the tissue block; or pankeratin immunohistochemistry performed in cases with negative hematoxylin and eosin. Euscher et al did not find a significant difference between both methods.
The systematical assessment in our study was performed by an extended search by two independent reviewers. Since all non-English articles and ‘abstract-only’ articles were excluded, some important studies might have been missed. Only 15 manuscripts were found applicable for this study. This limited amount is mainly a result of authors not describing full pathological protocols. In the remaining manuscripts, multiple ultrastaging techniques were described, often not fully complete, causing difficulty in comparing the different methods to each other. This led to descriptive rather than qualitative statistics and caused difficulty in assessing the superior ultrastaging technique.
Due to the large heterogeneity in ultrastaging techniques (eg, macroscopic slicing, number of microscopic slides, interval between slides), subgroups were small and therefore a comparison between ultrastaging variables was difficult. This is an important drawback in our systematic review, together with the absence of randomized controlled trials. In our results, the only important factor seems to be the macroscopic slicing procedure. Longitudinal slicing appeared to lead to a lower detection rate of sentinel lymph node metastases compared with bread-loaf slicing. These results could not be explained by differences in patients' pathological characteristics between the studies (ie, tumor grade, myometrial invasion, lymphovascular space invasion). Another limitation of our study might be that we included patients in whom frozen section was applied to the sentinel node. This might have influenced the outcomes of ultrastaging, since frozen section may have influenced the ultrastaging. The Society of Gynecologic Oncology advised against frozen section of sentinel lymph nodes (because of relatively low sensitivity for detection of metastases in normal appearing lymph nodes, cost, and potential alteration of ultrastaging pathology). However we did not exclude these patients because of the scarcity of the included studies.
Furthermore, of a total of 2783 patients with endometrial cancer, distributed over 15 studies, 406 patients were excluded because of the inability to detect a sentinel lymph node (78% of a total of 522 excluded patients). Nowadays, the success rate of detecting the sentinel lymph node has increased, with a high diagnostic accuracy and a negative predictive value up to 95%. This will possibly result in different outcomes. In addition, we have to mention that we excluded patients with a positive node by lymph node dissection but negative by sentinel lymph node mapping, since we were not able to identify the reasons for this finding (eg, technical failure of mapping, dissection of wrong nodes, or empty pockets of lymph nodes, failure of pathological assessment).
Recommendations and Future Research
Our systemic review shows that multiple different ultrastaging protocols are described in assessing the sentinel lymph node in endometrial cancer, making it challenging to assess the most effective protocol. Even though our data are very heterogeneous, the bread-loaf slicing method showed a higher detection rate of lymph node metastases compared with longitudinal slicing. We also found that using more than one slide for ultrastaging (including immunohistochemistry) did not result in a higher detection rate of sentinel lymph node metastases. Based on our data, we suggest that pathological assessment of the sentinel lymph node in endometrial cancer should be based on the bread-loaf slicing technique with one slide used for immunohistochemistry. In this way the sentinel lymph node procedure is standardized based on the best scientific evidence to date. Future research should focus on the amount of slides, as well as cost ramifications, to assess whether the time and effort spent performing the additional sectioning and staining will indeed change the tumor stage, the subsequent treatment, and finally the outcome of the patients. Hopefully, all these efforts will lead to optimal clinical guidelines.
Conclusion
The use of ultrastaging in general after routine hematoxylin and eosin staining in endometrial cancer patients has led to an increased detection rate of sentinel lymph node metastases and ultrastaging might therefore be of additional value in histopathological evaluation of the sentinel lymph node. Although a lot of different ultrastaging protocols were used, our systemic review favors the bread-loaf slicing technique with one slide used for ultrastaging (including immunohistochemistry) as the most effective way to detect sentinel lymph node metastases.
Thus, as sentinel lymph node mapping becomes standard of care in endometrial cancer, a uniform protocol for ultrastaging of the sentinel lymph node is essential for providing reproducible information, on which prognosis can be determined and therapeutic guidelines can be based.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
LCB and EMH are joint first authors.
Contributors PZ conceived of the presented idea. LB and EH performed data extraction. JH performed data analysis in collaboration with LB and EH. LB and EH contributed to the interpretation of the results and the writing of the manuscript. All authors provided critical feedback and helped shape the research, analysis, and manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.