Article Text

Abstract
Introduction Recent evidence has shown adverse oncological outcomes when minimally invasive surgery is used in early-stage cervical cancer. The objective of this study was to compare disease-free survival in patients that had undergone radical hysterectomy and pelvic lymphadenectomy, either by laparoscopy or laparotomy.
Methods We performed a multicenter, retrospective cohort study of patients with cervical cancer stage IA1 with lymph-vascular invasion, IA2, and IB1 (FIGO 2009 classification), between January 1, 2006 to December 31, 2017, at seven cancer centers from six countries. We included squamous, adenocarcinoma, and adenosquamous histologies. We used an inverse probability of treatment weighting based on propensity score to construct a weighted cohort of women, including predictor variables selected a priori with the possibility of confounding the relationship between the surgical approach and survival. We estimated the HR for all-cause mortality after radical hysterectomy with weighted Cox proportional hazard models.
Results A total of 1379 patients were included in the final analysis, with 681 (49.4%) operated by laparoscopy and 698 (50.6%) by laparotomy. There were no differences regarding the surgical approach in the rates of positive vaginal margins, deep stromal invasion, and lymphovascular space invasion. Median follow-up was 52.1 months (range, 0.8–201.2) in the laparoscopic group and 52.6 months (range, 0.4–166.6) in the laparotomy group. Women who underwent laparoscopic radical hysterectomy had a lower rate of disease-free survival compared with the laparotomy group (4-year rate, 88.7% vs 93.0%; HR for recurrence or death from cervical cancer 1.64; 95% CI 1.09–2.46; P=0.02). In sensitivity analyzes, after adjustment for adjuvant treatment, radical hysterectomy by laparoscopy compared with laparotomy was associated with increased hazards of recurrence or death from cervical cancer (HR 1.7; 95% CI 1.13 to 2.57; P=0.01) and death for any cause (HR 2.14; 95% CI 1.05–4.37; P=0.03).
Conclusion In this retrospective multicenter study, laparoscopy was associated with worse disease-free survival, compared to laparotomy.
- uterine cervical neoplasms
- hysterectomy
Statistics from Altmetric.com
HIGHLIGHTS
In early-stage cervical cancer, laparoscopic radical hysterectomy had worse disease-free survival.
After adjustment for adjuvant treatment, more recurrence and death were observed in laparoscopy.
The findings from this study are not sufficient to recommend laparoscopy in tumors less than 2 cm.
Introduction
Cervical cancer is the fourth leading oncological cause of death in women worldwide, with an estimated 569 847 new cases and 311 365 deaths per year. The greatest burden of the disease occurs in less developed regions of the world, where it accounts for almost 12% of all female cancers.1 The preferred management for cervical cancer with International Federation of Gynecology and Obstetrics (FIGO) 2009 stage IA1 with lymph vascular invasion, IA2, and IB1 in women without a desire for fertility preservation is radical hysterectomy with pelvic lymph node assessment.2 After the introduction of minimally invasive surgery, there was an increase in the use of this approach supported by a lower morbidity and similar oncological outcomes, compared with open surgery.3 4
A recent phase III randomized clinical trial demonstrated that minimally invasive radical hysterectomy was associated with lower rates of disease-free survival and overall survival, compared with abdominal radical hysterectomy among women with early-stage cervical cancer.5 These findings were reproduced in a large cohort study, in which the authors demonstrated that the adoption of minimally invasive surgery for early-stage cervical cancer coincided with a decline in the 4-year relative survival rate.6
After the publication of these studies, several authors have published their results regarding the oncological impact of the surgical approach, showing similar findings for patients undergoing minimally invasive surgery when compared with open surgery.7–21 However, in some centers, reference for the management of cervical cancer, especially in Latin America, had not been evaluated. The main objective of this study was to compare the year disease-free survival in patients with early-stage cervical cancer who underwent radical hysterectomy and pelvic lymphadenectomy either by laparoscopy or laparotomy.
Methods
Study population
We conducted a multicenter retrospective cohort study in seven reference centers for cervical cancer management from six countries: Instituto Nacional de Cancerología (Bogotá, Colombia), Instituto de Cancerología Las Américas (Medellin, Colombia), Instituto Nacional de Cancerología-INCAN (México), Hospital Italiano (Buenos Aires, Argentina), Foundazione IRCCS Istituto Nazionale Tumori (Milan, Italy), Instituto Nacional de Enfermedades Neoplasicas-INEN (Perú), and Hospital Universitario La Paz (Madrid, Spain). IRB approval was obtained in each institution.
Patients diagnosed with an early-stage cervical cancer who underwent a radical hysterectomy and pelvic lymphadenectomy, either by minimally invasive surgery or the open approach were identified from January 1, 2006 to December 31, 2017. We included patients older than 18 years, with diagnosis of stage IA1 with lymph vascular invasion, IA2, and IB1 (FIGO 2009 classification).22 Histologies included were: squamous, adenocarcinoma, or adenosquamous. Patients with non-radical hysterectomy, laparoscopic-assisted vaginal radical hysterectomy, robotic radical hysterectomy, abandoned surgery due to intraoperative findings, radical hysterectomy for stage II endometrial cancer, patients that received neoadjuvant chemotherapy prior to surgical treatment, women who underwent fertility-preserving treatment, cervical cancer diagnosed during pregnancy, prior or concurrent neoplasia at the time of diagnosis, and patients registered in a prospective controlled trial were excluded. Pre-operative imaging (MRI, CT, or ultrasound) was performed according to availability in each institution. Radical hysterectomy type B or C according to the Querleu–Morrow classification was performed according to the local institutional protocol.23 In all laparoscopic radical hysterectomy cases, a uterine manipulator was used, which was chosen at the surgeon’s discretion. In all patients, pelvic lymphadenectomy without sentinel lymph node mapping was performed. Adjuvant treatment was provided in each center according to Sedlis'24 and Peters'25 criteria (with radiotherapy or radiotherapy plus chemotherapy, respectively).
Data collection
The collection and audit of the quality of the data was carried out in two phases. First, the data were extracted by a coordinator, collected in the Research Electronic Data Capture (REDCap) software, and audited by the researcher from each participating center. Subsequently, a central verification of the information was carried out in the Data Analysis Unit of the Instituto Nacional de Cancerología, comparing the medical records with the REDCap data. Clinical information, final pathology reports, the need for adjuvant treatment, recurrence rate, and vital status were included. The preoperative tumor size was registered as <2 cm and >2 cm according to the size determined by physical examination, as allowed by the FIGO 2009 classification. The pathology data in each center was reviewed by an expert in gynecological malignancies. Data are available on reasonable request.
Statistical analysis
The exposure of interest was the initial treatment approach of laparoscopy vs laparotomy. We performed an intent-to-treat analysis, in which patients who had initial laparoscopy were included even if they were converted to an open procedure. The primary outcome of interest was disease-free survival, calculated from the time of surgery to the date of recurrence or death from cervical cancer. Recurrence diagnosis date with biopsy or imaging studies was extracted from the medical record. Overall survival was calculated from the time of surgery to death for any cause. Patients were censored at the time of the last oncological medical visit recorded in their clinical history if they did not have the event or had been lost to follow-up. Additional outcomes included lymph node count, frequency of positive lymph nodes, parametrial involvement, and positive surgical margins. Control variables included age at diagnosis (22–39, 40–49, 50–59,>=60), year of diagnosis (2006–2008 vs 2009–2011 vs 2012–2014 vs 2015–2017), stage (IA1 with lymphovascular space invasion vs IA2 vs IB1), histology (squamous vs adenocarcinoma vs adenosquamous), grade (grade 1, grade 2, grade 3), tumor size (<2 cm vs >2 cm), cone biopsy (yes, no), and adjuvant treatment (yes, no). Missing values were included for each variable as a separate group.
We compared categorical variables using χ2 tests and continuous variables using independent sample t-tests in the unweighted cohort. In the main patient-level analysis we used inverse probability of treatment weighting based on propensity score to construct a weighted cohort of subjects who differed with respect to surgical approach but were otherwise similar on other measured characteristics.26 27 To calculate the inverse probability of treatment weighting, we estimated each patient’s propensity to undergo laparoscopic radical hysterectomy using a logistic regression model that included predictor variables selected based on their a priori possibility of confounding the relationship between surgical approach and survival (age, year of diagnosis, stage, histology, grade, tumor size). We assigned patients who underwent laparoscopic radical hysterectomy a weight of 1⁄ (propensity score) and those who underwent a laparotomy a weight of 1⁄ (1-propensity score).28 To reduce the variability in the inverse probability of treatment weighting models, we used stabilized weights as suggested by Robins et al.29 To ensure the weighted cohort was balanced on observed covariates, we calculated absolute standardized differences, and considered a difference of 0.1 or less to be well balanced.28
The comparison of the distributions of categorical variables was done using weighted logistic regression models in the cohort after inverse probability of treatment weighting. Survival, perioperative, and pathologic outcomes were evaluated for approach. We compared disease-free survival and all-cause mortality using inverse probability of treatment weighting log-rank test, and plotted weighted survival functions.30 We estimated the HR for disease-free survival and all-cause mortality after minimally invasive surgery radical hysterectomy, relative to laparotomy, with weighted Cox proportional hazard models.
In the intention-to-treat population, we performed several sensitivity analyzes assessing the robustness of the findings observed in the main analysis. To ensure that treatment-related differences in survival were not confounded by differential use of adjuvant therapy, we refitted the survival model after including postoperative treatment as a covariate (radiotherapy, chemoradiotherapy, chemotherapy, or no further treatment). We repeated analyzes stratified by tumor size (<2 cm vs. >2 cm) in the propensity-balanced cohorts groups, using weighted Cox proportional hazard models: we also tested for the interaction of treatment approach by size in separate models. The proportional hazards assumption was verified in the models for approach. In addition, an analysis was performed including in the model the variable control residual postconization disease (yes, no), defined as the presence of residual tumor in the surgical specimen of radical hysterectomy, having previously performed a conization, through multiple imputation. Finally, we repeated the analysis with centers that performed more than 10 radical hysterectomies per year.
Significance levels of α=5% were used for all hypothesis tests. The statistical analysis of the information was performed in the statistical software R- project version 3.6.2 (Vienna, Austria; http://www.R-project.org/), and SAS Enterprise Guide version 7.11.
Results
A total of 1385 patients among all institutions underwent a radical hysterectomy and pelvic lymphadenectomy (Figure 1). Until 2012, the majority of cases were performed by laparotomy (n=453; 61.4%) compared with laparoscopy (n=285; 38.6%), but since 2013 there was a higher frequency of laparoscopy (n=403; 62.3%) vs laparotomy (n=244; 37.7%) (Figure 2). The number of cases performed by approach in each center is shown in the Online supplemental material. Cases were done concurrently in all centers using the two approaches during the study period (online supplemental Table S1).
Supplemental material

Population flowchart.
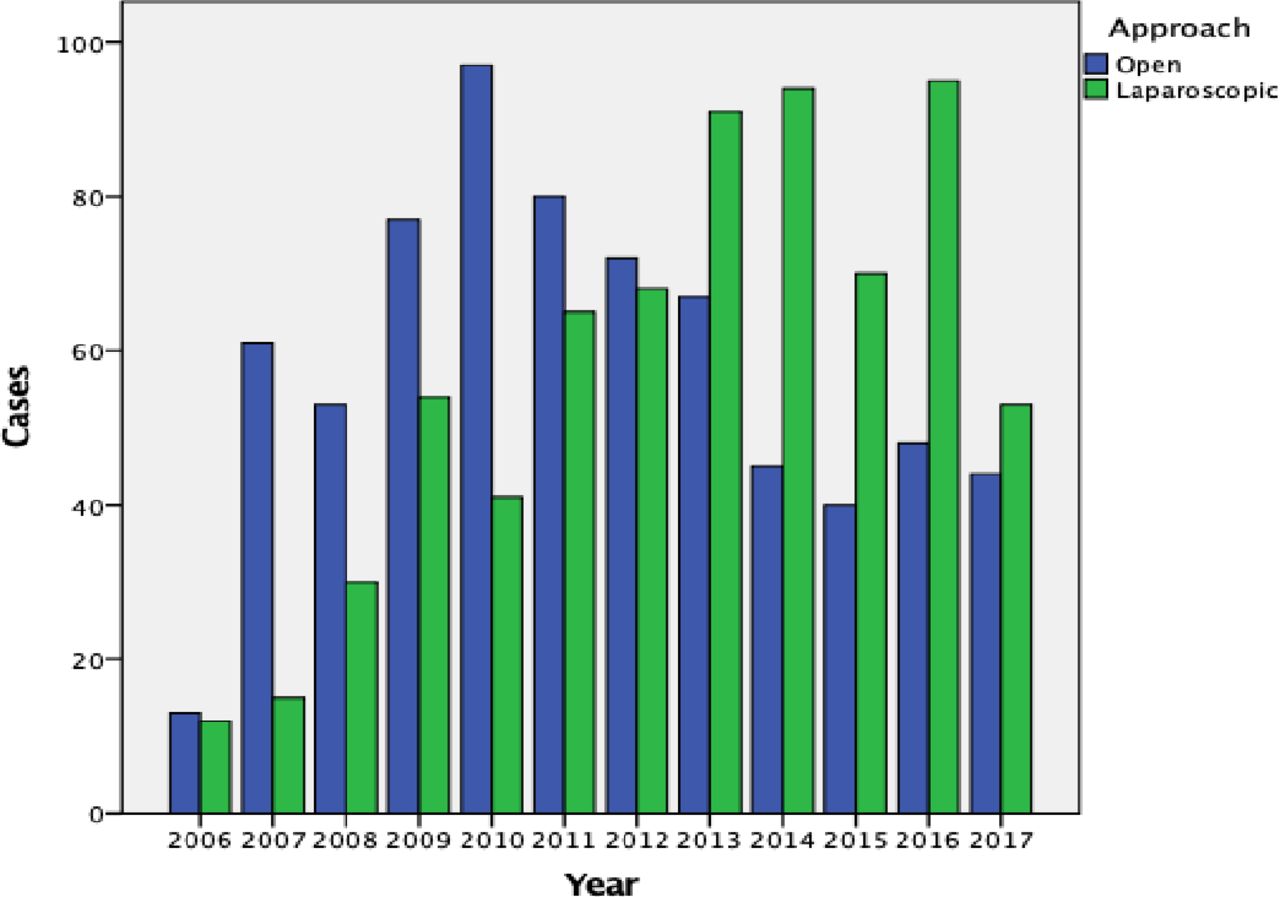
Procedure by approach during the study follow-up.
The demographic and clinical characteristics before and after propensity score balancing are shown in Table 1. For the inverse probability of treatment-weighting analysis, 1379 patients were included, of whom 681 (49.4%) patients underwent surgery by laparoscopy and 698 (50.6%) by laparotomy. Seven (1.0%) patients in the laparoscopy group were converted to laparotomy. In the balanced cohort, there were missing data by approaches (laparoscopy vs laparotomy) for the variables' histological grade (10% vs 9.5%, P=0.98), tumor size (2.4% vs 2.2%, P=0.92), cone biopsy 0.2% vs 0.2%, P=0.99),and adjuvant treatment (0.1% vs 0.5%, P=0.41), respectively, without differences.
Characteristics of patients for surgical approach, before and after inverse probability of treatment weighting
Regarding postoperative pathology in the weighted cohort, when comparing patients in the laparoscopy vs laparotomy group, there were no differences in the rates of positive vaginal margins (4.0% vs 6.0%, P=0.09), deep stromal invasion (more than two-thirds of cervical stroma) (19.3% vs 11.7%, P=0.45), and lymphovascular space invasion (26.1% vs 27.3%, P=0.95). In the laparotomy group, the rates of pelvic lymph node involvement were lower (8.0% vs 11.3% P=0.04). The median number of pelvic nodes removed was 18 (range, 1–55) in the laparoscopy group and 19 (range, 1–79) in the laparotomy group (P=0.054).
Recurrence rate in the overall cohort was 7.1% (n=98). Of the patients, 64.3% (n=63) were operated by laparoscopy and 35.7% (n=35) by laparotomy. Regarding tumor size, 59.2% (n=58) were recurrences in patients with <2 cm and 40.8% (n=40) in >2 cm. A different recurrence pattern was found between the groups, with local presentation in 22.5% of patients (n=16 laparoscopy and n=6 laparotomy), regional 20.4% (n=13 laparoscopy and n=7 laparotomy), distant 18.4% (n=11 laparoscopy vs n=7 laparotomy), and multiple 38.8% (n=23 laparoscopy vs n=15 laparotomy), respectively (P=0.042). The median time to recurrence was similar between groups, 24 months (range, 2.27–124) in the laparoscopy group vs 21.9 months (range, 1.08–54) in the laparotomy group (P=0.29). Online supplemental Table S2 shows the rate of recurrence by centers and approach. Death rate in the overall cohort was 2.5% (n=35). Regarding tumor size, 68.6% (n=24) were recurrences in patients with <2 cm and 31.4% (n=11) in >2 cm.
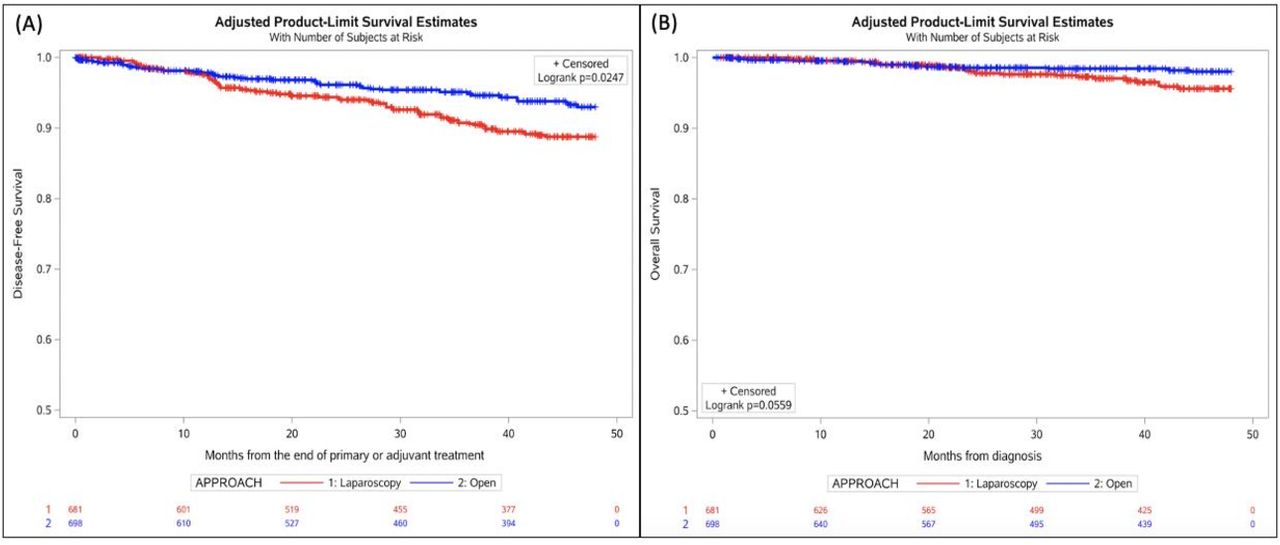
Survival functions in the inverse probability of treatment-weighted cohort for women who underwent radical hysterectomy by laparoscopy and laparotomy are plotted in Figure 3. Median follow-up in the propensity-balanced cohort was 52.1 months (range, 0.8–201.2) for those who underwent laparoscopy and 52.6 months (range, 0.4–166.6) for those who underwent laparotomy. Women who underwent laparoscopic radical hysterectomy had inferior disease-free survival compared with those who underwent laparotomy (4-year rate, 88.7% vs 93.0%; HR 1.64; 95% CI 1.09 to 2.46; P=0.02). The risk of recurrence or death from cervical cancer within 4 years of surgery was 11.3% vs 7%, respectively. No differences were found by approaches in the risk of death for any cause (HR 2.04; 95% CI 1.00 to 4.16; P=0.06). Cumulative incidence of death for any cause at 4 years of diagnosis was 4.4% for laparoscopy vs 2% for laparotomy.

Inverse probability of treatment-weighted survival curves according to surgical approach. (A) disease-free survival. (B) overall survival.
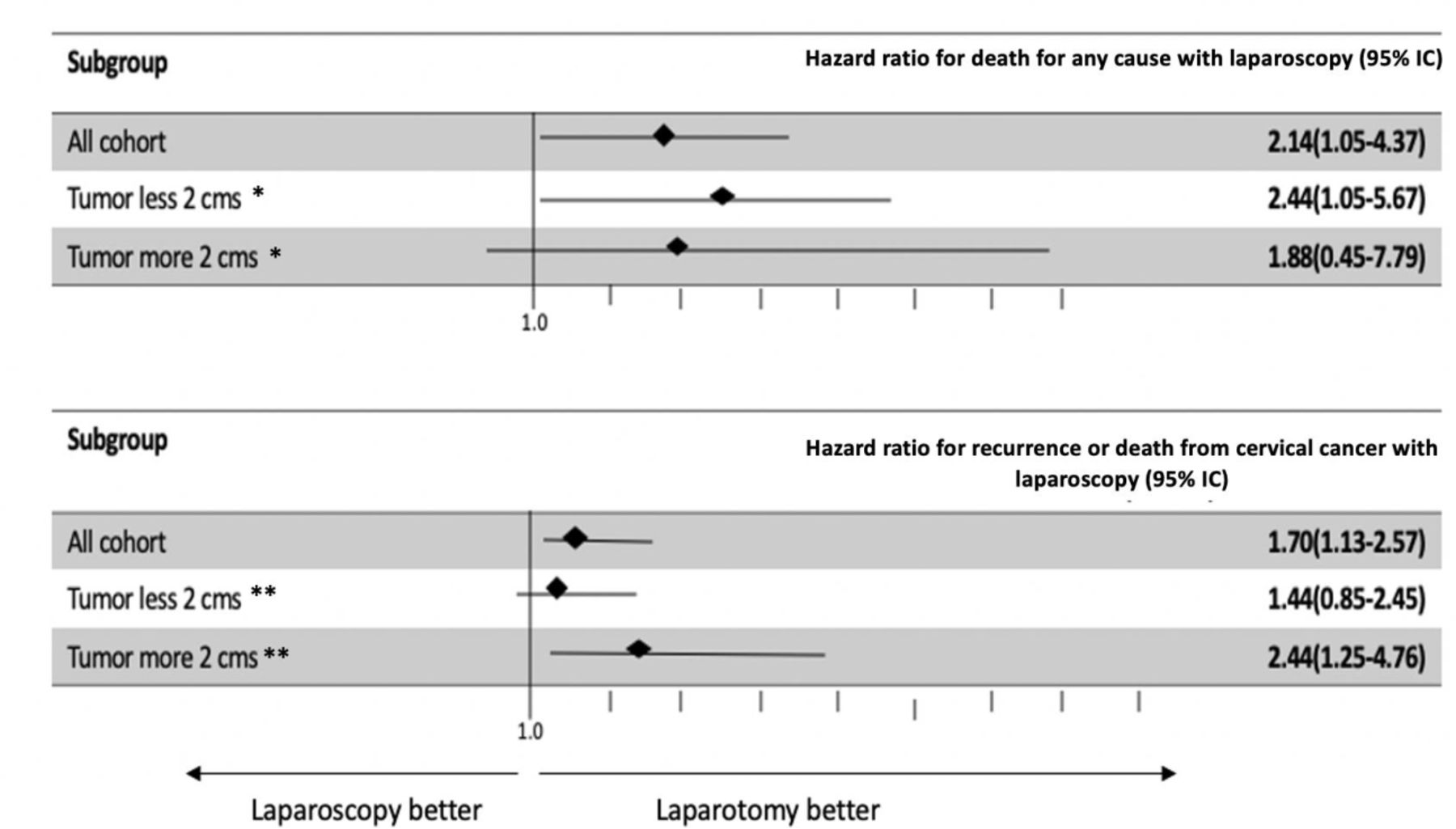
In sensitivity analyzes, after adjustment for adjuvant treatment, radical hysterectomy by laparoscopy compared with laparotomy was associated with increased hazards of recurrence or death from cervical cancer (HR 1.7; 95% CI 1.13 to 2.57; P=0.01) and death for any cause (HR 2.14; 95% CI 1.05–4.37; P=0.03)(Figure 4). We repeated analyzes stratified by tumor size in the propensity-matched groups, and we also tested for the interaction of treatment approach by tumor size and treatment approach by period of diagnosis in separate models. Results differed slightly after stratifying by tumor size. For tumors<2 cm (n=486 laparoscopy and n=492 laparotomy), there was not a statistically significant difference when comparing disease-free survival (HR 1.44; 95% CI 0.85 to 2.45; P=0.18), although the patients had a higher risk of death after laparoscopic radical hysterectomy (HR 2.44 95% CI 1.05 to 5.67; P=0.04). In tumors larger than 2 cm (n=181 laparoscopy and n=188 laparotomy), a higher risk of recurrence was identified in the laparoscopic surgery group (HR 2.44; 95% CI 1.25 to 4.76; P=0.009), although we did not identify a difference in overall survival by approach (HR 1.88; 95% CI 0.45 to 7.79; P=0.39). These differences were not statistically significant: disease-free survival P-value for interaction=0.26 and overall survival P-value for interaction=0.57 (Figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Multivariate Cox modeling adjusted for adjuvant treatment – overall survival and disease-free survival. *P-value for interaction=0.57. **P-value for interaction=0.26
When analyzing the presence of residual postconization disease within the model, worse oncological outcomes were observed with respect to recurrence and death from cervical cancer (HR 1.6; 95% CI 1.07 to 2.41; P=0.024) and death for any cause (HR 1.96; 95% CI 0.96 to 3.99; P=0.06), regardless of tumor size (online supplemental material, Figure 1).
A separate analysis was conducted in a propensity-balanced cohort of centers that performed more than 10 cases of radical hysterectomy per year (n=5). The analysis included 1234 cases, and there was no difference in disease-free survival (HR 1.30; 95% CI 0.82 to 2.07; P=0.30) and overall survival (HR 2.12; 95% CI 0.95 to 4.73; P=0.07) by surgical approach. Also, we did not find differences according to preoperative tumor size in hazards of recurrence and death from cervical cancer (<2 cm: HR 1.02; 95% CI 0.56 to 1.83; P=0.95.>2 cm: HR 1.90; 95% CI 0.84 to 4.32; P=0.20), and death for any cause (>2 cm: HR 2.09; 95% CI 0.87 to 5.03; P=0.09.>2 cm: HR 2.30; 95% CI 0.31 to 16.8; P=0.52), respectively (online supplemental materials, Figures 2 and 3).
Discussion
Summary of main results
Our study showed that patients who underwent a laparoscopic radical hysterectomy had worse disease-free survival compared with those that underwent a laparotomy. Additionally, in sensitivity analyzes, after adjustment for adjuvant treatment and the presence of postconization residual disease, we observed a higher risk of recurrence and death in the laparoscopy group. We could not demonstrate such differences when low-volume centers were excluded from the analysis.
Results in the context of published literature
Although observational studies do not provide the same level of evidence regarding the benefits of treatment approach as randomized controlled trials, several retrospective studies have confirmed the increased risk of recurrence and death of laparoscopy compared with open surgery in patients undergoing radical hysterectomy for early cervical cancer. These studies include population-based analyzes,6 10 19 single institution studies,7 8 multicenter series,9 11–18 20 21 and a meta-analysis of high-quality observational studies.31 Despite the consistent findings observed in these studies with the LACC trial,5 a smaller number of series have not identified differences in recurrence or survival.32–38 Differences in analytical approach, number of patients included, surgical technique, and follow-up time, could explain, at least in part these differences. Similarities and differences among studies that used propensity-score methods (including the current one) are shown in online supplemental Table S3.
The role of tumor size has important clinical implications. Prior studies have suggested that in women with tumors less than 2 cm, laparoscopy might not be associated with worse oncological outcomes compared with open surgery,7 8 11 14–19 32 34 36 39 40 while other authors have described worse results for minimally invasive surgery.9 12 13
However, it is important to consider the method of estimating tumor size to critically evaluate these studies.41 In the current study, tumor size was assessed by clinical examination in all the patients, as recommended by the FIGO 2009 cervical cancer classification.22 However, the inaccuracy of clinical staging and better imaging performance for tumor size estimation have been established. Therefore, it is possible that studies that primarily assessed tumor size by clinical examination can lead to erroneous estimates.42 Furthermore, previous studies that evaluated the impact of surgical approach on tumor size (<2 cm) were either not designed to assess this subgroup of patients or do not have the power to detect a difference in this group. In the current study, although not all the results of the stratified analysis are statistically significant, it is important to highlight that all the hazard ratios indicate a worse outcome with laparoscopy. When the presence of residual postconization disease was considered, laparoscopy had a higher risk of recurrence and death. The interaction term was not statistically significant, suggesting that in our cohort, the adverse effect of laparoscopy on either disease-free or overall survival did not depend on tumor size. Current evidence, including the findings from this study, is not sufficient to recommend laparoscopy in tumors less than 2 cm.
Among the hypotheses related to the negative oncological impact of minimally invasive surgery, the use of a uterine manipulator has been proposed. Chiva et al21 presented the results of a cohort study involving 582 women of 23 European countries. A propensity-matching score was performed for the analysis. The use of a manipulator was associated with a worse disease-free survival in the minimally invasive surgery group (HR 2.38; 95% CI: 1.32 to 4.29). However, it should be noted that in that study the design was not aimed at determining whether the uterine manipulator use was associated with oncologic outcomes. In addition, reasons for selection of the uterine manipulator were not specified. This aspect was not evaluable in our study, since in all cases a uterine manipulator was used to perform laparoscopic radical hysterectomy.
The association between surgical volume and oncological outcomes in women with early-stage cervical cancer has also been investigated. Matsuo et al43 found that surgery at high-volume centers (105 surgeries or more over a 5-year period) remained an independent prognostic factor for decreased recurrence (adjusted HR 0.69, 95% CI 0.57 to 0.84, P<0.001) and all-cause mortality (adjusted HR 0.75, 95% CI 0.59 to 0.95, P=0.016) compared with surgery at mid- and low-volume centers. Contrary to these findings, Aviki et al44 evaluated the oncological outcomes based on hospital surgical volume. High volume was defined as the performance of 6–20 hysterectomies in the prior year. The authors found that hospital volume was not an independent predictor of mortality. However, about 75% of the centers performed five or fewer cases of radical hysterectomy per year and thus may not be a true representation of the population of interest. It is also worth noting that the number of cases per surgeon were not included in these studies. Finally, Cusimano et al performed a population-based retrospective cohort study of cervical cancer patients undergoing primary radical hysterectomy from 2006 to 2017 in Canada.10 Technique-specific volume was defined as the number of simple and radical hysterectomies performed by the patient’s surgeon with the selected approach in the 1 year prior to the index procedure. Cervical cancer volume was defined as the number of hysterectomies of any type (simple and radical) or approach (minimally invasive and open) performed for cervical cancer in the 2 years prior to the index procedure. Neither technique-specific volume (death HR, 0.70; 95% CI, 0.45 to 1.07; recurrence HR, 0.79; 95% CI, 0.49 to 1.28) nor cervical cancer volume (death HR, 0.88; 95% CI, 0.46 to 1.68; recurrence HR, 1.17; 95% CI, 0.73 to 1.87) were significantly associated with oncologic outcomes in their final models.
In our cohort, among five centers that performed more than 10 cases per year, there were no differences in disease-free and overall survival by surgical approach or tumor size. While our results are intriguing, these findings should be interpreted with caution. Surgical volume limit was not established, as recommended for this type of analysis,43 44 and the number of procedures/years was selected by consensus. The change in surgical volume over time in each center, and the volume of cases per surgeons was not analyzed. Furthermore, the number of cases per approach was different between centers, and due to the small number of patients in the “low volume” centers, we were unable to compare outcomes with “high volume” centers.
Strengths and weaknesses
This study is a large multicentric cohort that evaluated long-term outcomes of laparoscopy for early stage cervical cancer, including centers in Latin America and Europe. However, we recognize a number of limitations, including the retrospective nature of the study, the lack of robot-assisted laparoscopy cases, since there was no availability of robotic platform in some participant’s institutions, the difference in proportion of open and laparoscopic cases across centers, and the difference in surgical volume among institutions (online supplemental Table S1). Additionally, although we used the inverse probability of treatment weighting based on the propensity score, this method has limitations, such as the inability to assess “unmeasured” factors involved in the treatment selection of the study population.45
Implications for practice and future research
The available information has led the National Comprehensive Cancer Network (NCCN),2 the European Society of Gynaecological Oncology (ESGO),46 FIGO,47 and the European Society for Medical Oncology (ESMO),48 to state that open radical hysterectomy should be considered the standard of care in the management of patients with early-stage cervical cancer. Given the controversy generated by the LACC trial, and the retrospective evidence from several studies that have shown similar outcomes, some groups have designed prospective clinical trials.49 50
Conclusions
In summary, in this retrospective multicenter study, the laparoscopic approach for early-stage cervical cancer was associated with a higher risk of recurrence and also a higher risk of death after adjustment for adjuvant treatment.
Until new results are obtained from prospective studies, patients should be informed of the increased risk of recurrence and death associated with laparoscopy prior to the decision on the approach in managing their disease.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @DrFMartinelli, @dramilagrospqGO
Contributors Study design: JR, RP, GR, DI, VV, DO, IZ, FM. Data acquisition: JS, MH, MH, AH, JS, VV, FN. Central audit: JS, MH. Data interpretation: JAR, JR, SF, RP. Manuscript writing: JR, JAR, RP. Manuscript review: JR, JAR, JS, DI, GR, DO, VV, IZ, JS, SF, FN, AL, RP.
Funding This study was not supported by any person or institution.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval IRB in each participant institution.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.