Article Text

Abstract
Fertility preservation is an integral component of clinical decision-making and treatment design. However, the selection criteria on imaging for patients eligible for fertility preservation is still unclear. The present review aimed to summarize the main findings reported in both the literature and international guidelines on the role of imaging in the selection of patients for fertility preservation. A search strategy was developed and applied to PubMed, Scopus, Web of Science, and EMBASE to identify previous citations reporting imaging and fertility preservation in patients with gynecological cancer. We also retrieved the published guidelines on the eligibility criteria for fertility-sparing treatment of gynecological neoplasms. A description of the internal multidisciplinary guidelines, clinically in use in our institution, is provided with representative clinical cases. The literature review revealed 1291 articles and 18 of these were selected for the analysis. Both ultrasound and MRI represented the primary imaging methods for selecting patients for fertility preservation in cervical and endometrial cancers. Eligibility criteria of fertility-sparing management in patients with cervical cancer were: tumor size <2 cm, tumor distance from the internal os >1 cm, and no parametrium invasion. For patients with endometrial cancer, these included no myometrial and cervical stroma invasion. Both ultrasound and MRI play a key role in characterizing adnexal masses. These modalities provide a useful tool in identifying small ovarian lesions, thus key in the surveillance of patients after fertility sparing surgery. However, efficacy in excluding disease beyond the ovary remains limited. This review provides an update of the literature and schematic outline for the counseling and management of patients with the desire for fertility preservation.
- ovarian cancer
- cervical cancer
- gynecology
- endometrial neoplasms
Statistics from Altmetric.com
Introduction
Currently, there is an increasing tendency to treat women with cancer and ensure good quality of life, including future fertility. Indeed, fertility preservation is an integral component of clinical decision-making and treatment design.1 2 Fertility-sparing options for young patients with gynecologic cancer are influenced by patient age, type of primary cancer, treatment, and patient preferences.3 Defining which patients are eligible for fertility preservation significantly relies on accurate cancer staging. In this context, ultrasound evaluation4 and MRI5–7 play an important role in the preoperative assessment of gynecological cancers.
In the literature, however, there are currently few reviews on fertility-sparing treatment,4 5 8–10 describing selection criteria on imaging for patients eligible for fertility preservation.7 11–14 An understanding of the potential pitfalls of imaging methods is crucial to avoid misinterpretation, as well as to guide management. The current review aims to summarize the main findings reported in both the literature and international guidelines (NCCN, ESMO/ESGO/ESTRO) on the role of imaging in the selection of patients eligible for fertility preservation. Additionally, a brief summary of the methodology used at our center for selecting these patients by using images of both ultrasound and MRI is described.
Methods
Review of the Literature
A search strategy was developed and applied to PubMed, Scopus, Web of Science, and EMBASE to identify previous citations reporting imaging and fertility preservation in patients with gynecological cancer. We used the following words for selection: (“fertility preservation” or “fertility sparing” or “fertility-sparing” or “conservative surgery” or “conservative management” or “conservative treatment” or “trachelectomy” or “hysteroscopic endometrial resection” or “fertility-sparing management” or “fertility sparing management”) and (“gynecological cancer” or “gynecology oncology” or “gynecologic malignancy” or “gynecologic cancer” or “gynecological malignancy” or “cervical cancer” or “cervical carcinoma” or “endometrial cancer” or “endometrial carcinoma” or “ovarian cancer” or “ovarian carcinoma” or “ovarian malignancy”) and (“ultrasound” or “image” or “imaging” or “MRI” or “ultrasonography” or “magnetic resonance”) and “imaging” or “ultrasound” and (“fertility preservation”) and (“gynecological cancer”) and “fertility sparing surgery” and (“gynecology” or “gynecological cancer”) and (“fertility sparing”) and (“imaging “) .
The search and selection criteria were restricted to full English language papers published from 1993 to 2020. We also retrieved the guidelines (NCCN, ESMO/ESGO/ESTRO)15–20 on the eligibility criteria for the fertility-sparing treatment of gynecological neoplasms. A description of the internal multidisciplinary guidelines used in our institution is provided, with representative clinical cases.
Results
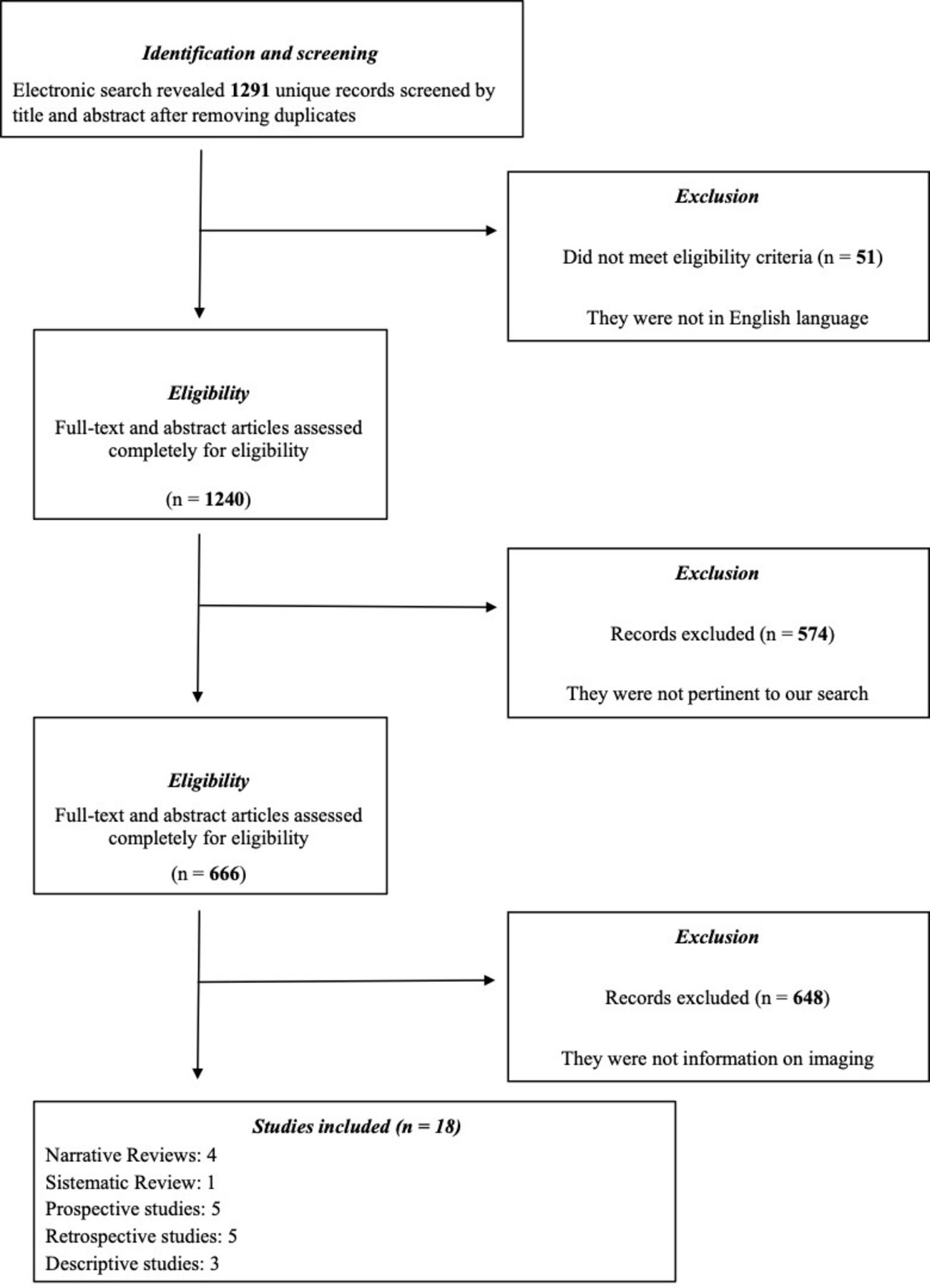
The literature review revealed 1291 articles, and 51 of these were excluded as they were not in the English language. We also excluded 574 articles that were not pertinent to our search, and finally, excluded another 648 articles that were mainly related to fertility-sparing treatment, but with no information on imaging. On completion of all exclusion criteria, there were 18 remaining articles that were evaluated and reported herein. The flowchart diagram is shown in Figure 1. According to the primary site of disease, we divided the selected manuscripts into three main subgroups: cervical cancer, endometrial cancer, and ovarian cancer (Table 1).
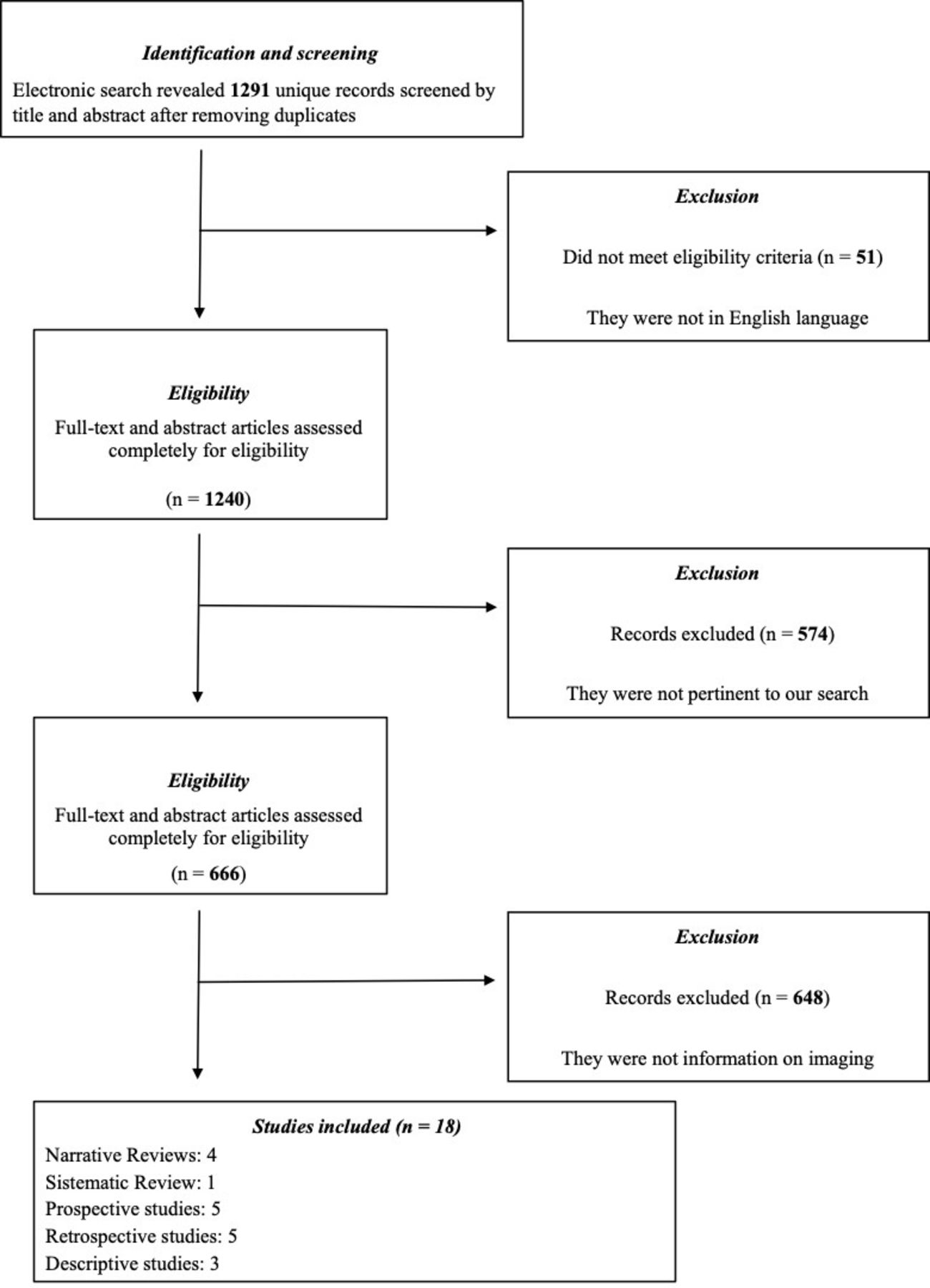
Flowchart diagram summarizing the selected articles.
Summary of studies reporting imaging parameters indicating patients eligible for fertility preservation
Cervical Cancer
Cervical cancer is the second most commonly diagnosed cancer and the third cause of cancer death among women in less developed countries (sub-Saharan Africa, Latin America and the Caribbean, and Melanesia) with more than 40% of patients with early cervical cancer affected during reproductive age where there is a desire for future fertility.21 According to international society guidelines, including NCCN, ESMO/ESGO/ESTRO, patients with microinvasive disease (FIGO stage IA1) and no lymphovascular space invasion (LVSI) are candidates for cone biopsy only. For patients with FIGO stage IA1 but with LVSI, the risk of node involvement is greater and a sentinel lymph node (SLN) mapping algorithm or pelvic lymphadenectomy is recommended.15 16 Radical trachelectomy may offer a reasonable fertility-sparing treatment option for patients with cervical cancer of FIGO 2018 stage IA2 or IB1. Laparoscopic pelvic lymphadenectomy complements the procedure and can be performed with or without SLN mapping.15 16 Patients with an histology of squamous cell carcinoma, adenocarcinoma, or adenosquamous carcinoma are eligible for fertility-sparing treatment, whereas patients with small cell neuroendocrine tumors, gastric type, or adenoma malignum are ineligible.15 16 Tumor size, tumor extending to the internal os, stromal invasion, parametrial invasion, and the presence of lymphovascular invasion and extrauterine spread are among the most important parameters when selecting patients who might benefit from fertility-sparing surgery.
Among the articles on cervical cancer and fertility-sparing options, we selected 11 articles dealing with MRI and one with ultrasound evaluation. In particular, we found one systematic review,10 one narrative review,8 three retrospective studies,11–13 two prospective studies,22 23 and one descriptive article on MRI in cervical cancer,14 whereas four articles (two descriptive studies6 7 and two narrative reviews4 5) reported fertility-sparing in several gynecological cancers including data for fertility preservation in patients with cervical cancer (three on MRI and one on ultrasound) (Table 1).
Tumor Size
The current selection criteria for vaginal radical trachelectomy include a tumor size of <2 cm where the measurement is based on the three dimensions (anteroposterior, craniocaudal, and transverse).5–8 11 12 14 23 MRI has been shown to be accurate in evaluating tumor size to within 5 mm of surgical dimension.14 The shape of the lesion and its pattern of growth, which may be exophytic (outward or eccentric to the cervical canal) or endophytic (inward or along the cervical canal), must be reported.14 For tumors measuring more than 2 cm, neoadjuvant chemotherapy followed by conization or trachelectomy may also be an acceptable choice, but downstaging by neoadjuvant chemotherapy in patients with FIGO 2009 Stage IB1 and IB2 before fertility-sparing surgery is still an experimental technique.15
Tumor-to-Internal Os Distance
The ideal distance between the superior margin of the cervical tumor and the internal os (inner aspect of the cervix) is ≥1 cm in order to allow for a 1 cm of healthy cervical stroma between internal os and anastomosis, however, some authors accept ≥0.5 cm.5–7 10 12–14 22 23 The internal os is defined as the region where the uterine vessels enter the uterus and the narrowing of the uterine contour where the low-signal-intensity cervical stroma changes to the intermediate-signal intensity of the uterine myometrium. The distance between the internal os and the cranial margin of the tumor should be assessed in the sagittal plane.12 MRI has a high specificity for identifying invasion of uterine cervical cancer into the internal os.10 13 The length of the endocervical canal is also an important measurement for adequate surgical planning.14 Indeed, it was suggested that a cervix length of more than 2 cm is necessary for performing trachelectomy or conization.
Depth of Stromal Cervical Invasion
To achieve a fertility-sparing treatment, stromal cervical invasion should be less than half of the stromal thickness.5 6 8 12 14 The assessment of stromal invasion at MRI has been demonstrated to be imprecise.
Stromal invasion is seen on T2-weighted MRI as partial or complete disruption of the low-signal-intensity cervical stroma by an intermediate- to high-signal-intensity lesion.14 The presence of a low-signal-intensity ring of cervical stroma around the tumor excludes parametrial involvement with a negative predictive value of 94%–100%.14 The presence of a complete disruption of the hypointense stromal rim has been shown to have only a 50% predictive value for parametrial involvement. However, if the hypointense cervical stromal ring is completely interrupted by the tumor, either focally or diffusely, with the presence of nodular or spiculated tumor-to-parametrial interface, or encasement of peri-uterine vessels, the accuracy for parametrial involvement raises to 77%–96%.14 Tumor spread beyond the cervix is a contraindication to conservative surgery.5 7 11
Lymph Node or Distant Metastases
Lymph node involvement is also a contraindication to fertility-preserving surgery.5–7 14 Regarding ultrasound examination, one narrative review describing ultrasound parameters for fertility preservation for gynecological cancer reported data on cervical cancer.4 According to this manuscript, ultrasound examination provides detailed images of the cervical tumor, and tumorous distance from the internal os. Moreover, with ultrasound examination, deep stromal tumor invasion, parametria, and metastatic disease (bladder infiltration, rectum infiltration) can be evaluated.4 Ultrasound has demonstrated low sensitivity and high specificity in evaluating lymph node metastases in cervical cancer.24 In our institution, preoperative evaluation of patients eligible for fertility preservation is based on both ultrasound and MRI imaging. We acknowledge that, according to international guidelines, in patients with early cervical cancer, transvaginal ultrasound examination is sufficient if performed by experienced ultrasound examiners, as it is able to provide fundamental parameters for the selection of patients for fertility preservation.15 16 However, despite the high costs, in our institution we also request MRI in order to have a panoramic assessment of the pelvis, with particular regards to lymph node evaluation. On the other hand, we do not exclude transvaginal examination as it represents the first diagnostic approach in all our oncological patients.
Ultrasound Methodology
Patients are examined in the lithotomy position with an empty bladder with a transvaginal or transrectal approach: this is complemented by an abdominal ultrasound examination to evaluate for lymph node enlargement within the pelvis.24 Cervical tumor is measured (in mm) in three dimensions: cervical fundal diameter, anteroposterior diameter in sagittal projection, and lateral diameter in transverse plane. It usually appears as a solid lesion with mostly hypoechoic echostructure in comparison with the surrounding cervical stroma.25 Echogenicity of the tumor can appear as isoechoic, hyperechoic, or mixed, according to the surrounding cervical stroma (Figure 2).24 According to its growth pattern, the cancer may appear as a ‘mushroom-shaped’ lesion when exophytic and ‘ovoidal’ or ‘conic-shaped’ lesions when endophytic.25
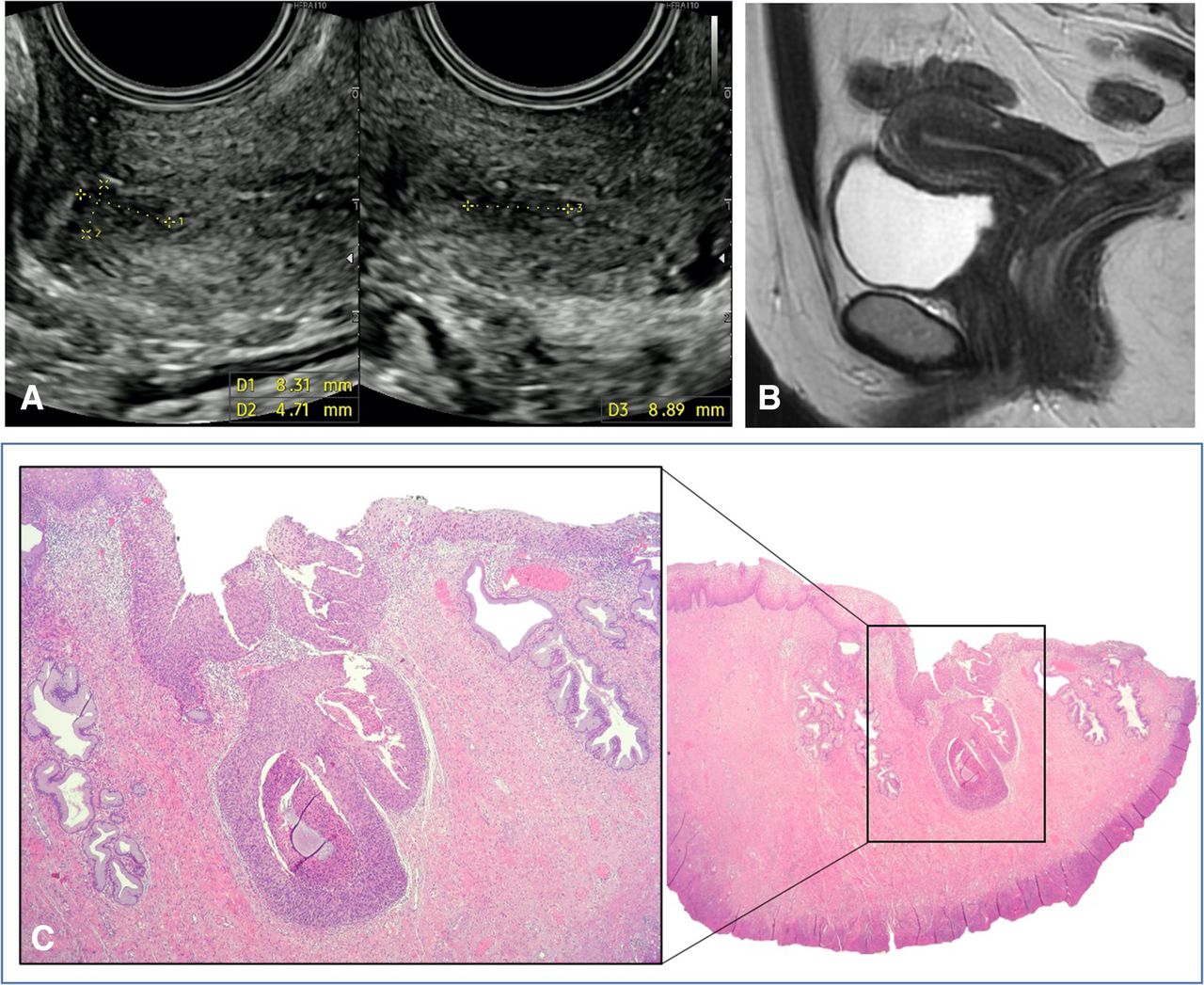
Ultrasound, MRI, and microscopic images of a 33 years' old patient with abnormal uterine bleeding. Ultrasound image (a) shows a hypoechoic lesion of 8x4×8 mm in size, with irregular margins suspicious for an early cervical cancer. The sagittal T2-weighted Mr image (b) shows the normal appearance of the cervix, with no visible tumor; no area of restricted diffusion at diffusion-weighted MR imaging or abnormal contrast enhancement was present (not shown). Histology (c) confirmed an area of 6 mm (zoom area in the box) of severe cervical dysplasia.
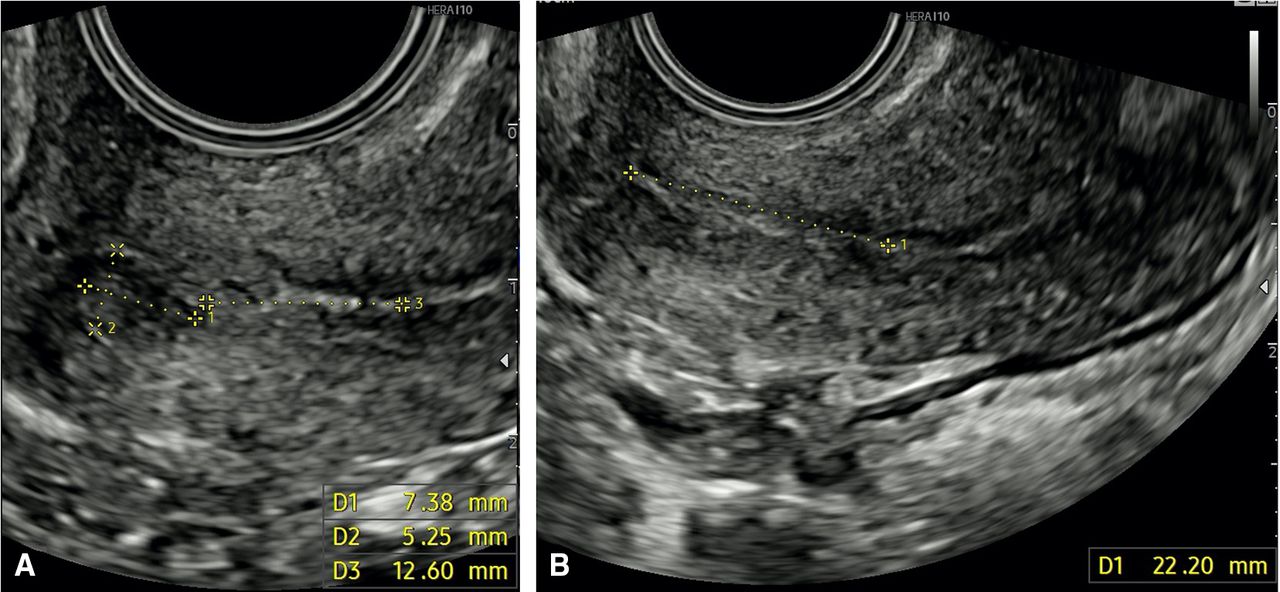
The next step is the evaluation of the superior margin of the tumor to internal os distance. The total length of the cervix is also evaluated (Figure 3). The third priority is to evaluate the extent of tumor stromal invasion. The proportion of stromal invasion can be defined as either partial (≤2/3 or >2/3) or full thickness or, more precisely, it can be defined based on the measurement of tumor-free stroma.4 One should then evaluate parametrial involvement, at the level of anterior, lateral, and dorsal parametria.25 26

Ultrasound images showing the distance between the superior margin of the cervical lesion and the internal uterine os (a) and the total cervix length (b).
MRI Protocol and Methodology
MRI protocol. At our institution, patients are examined with a 1.5 T MR scanner using a standard 8-channel phased-array body coil. Patients are encouraged to fast 4 hours and empty the bladder prior to MRI examination to reduce peristalsis-related motion artifacts. An anti-peristaltic agent is administered intramuscularly at the start of the examination to further reduce peristalsis. Conventional sequences included axial T1-weighted and T2-weighted sequences for panoramic pelvic evaluation and high-resolution T2-weighted sequences performed in the sagittal, axial oblique (perpendicular), and coronal oblique planes (parallel) along the long axis of the cervix. Diffusion-weighted imaging is performed in the sagittal and axial oblique planes in the same orientation as T2-wieghted planes (b=0 and 800–1000 sec/mm2) and apparent diffusion coefficient maps obtained. Large field-of-view T2-weighted (T2WI) images from the top of the kidneys to the iliac crests are acquired to exclude hydronephrosis and para-aortic lymphadenopathy. Dynamic contrast-enhanced MRI (DCE-MRI) is currently optional with newly diagnosed cervical cancer at an advanced stage. However, DCE-MRI has been demonstrated to improve tumor-to-cervical stromal contrast in patients with small tumors (<2 cm) and should be used in patients considered for fertility preservation.14 We use sagittal DCE-MRI both before and after administration of contrast material, in order to identify small-volume lesions that may be difficult to detect on T2-weighted images and to better evaluate stromal invasion. Diffusion-weighted imaging should always be read in combination with T2WI sequences and contrast-enhanced images.
Cervical cancer demonstrates intermediate singal intensity on T2-weighted imaging, high-signal intensity on high b-value diffusion-weighted imaging,and low- signal intensity on the apparent diffusion coefficient map.
MRI reports to assess eligibility for fertility-sparing treatment should include (Figure 4):
Uterus information: length of the cervix from the internal os to the external os and length of the endometrial cavity from the fundus to the internal os, both measured on sagittal plane.
Tumor information: diameter of the tumor on three axes, evaluated on sagittal plane for cranio-caudal and anteroposterior diameters and on oblique axial for transvers diameter; site of the tumor within the cervix (anterior or posterior lip, right or left side, circumferential); tumor growth characteristics (exophytic or infiltrating); presence and extent of cervical stroma infiltration (<50% or 1 cm with measurement of free stromal ring; or full-thickness); and distance of the proximal margin of the tumor to the internal os, vaginal fornix, or parametrium
Lymph nodes information: absence or presence of pelvic or para-aortic nodal enlargement (short-axis diameter larger than 10 mm); and other suspicious lymph nodes characteristics consist of round morphology, irregular borders and presence of necrosis.
Other findings in pelvis or abdomen: presence of peritoneal implants, bladder, rectum, ovaries, liver, kidney, bone.

A sagittal T2-weighted MR image (a) showing soft tissue with intermediate signal intensity (green arrows), consistent with a cervical tumor, in the anterior and posterior lips of the cervix with maximum diameter of 2 cm, with a distance from the tumor and the internal uterine os more than 1 cm. sagittal T2-weighted MR image. (b) shows the measurements that should be assessed in order to plan fertility-sparing treatment. level of internal uterine os (yellow line). Length of the cervix from the internal uterine os to the external uterine os (white line), distance from the cranial margin of the tumor to the internal os (red line).
Endometrial Cancer
Endometrial cancer is the most common gynecological cancer in developed countries. More than 90% of endometrial cancers occur in women >50 years of age, with a median age at diagnosis of 63 years. However, 4% of patients diagnosed with endometrial cancer are younger than 40 years, and many of these patients wish to conceive.27 According to international societies and guidelines, including NCCN, ESMO/ESGO/ESTRO,17 18 patients with an histology of endometrioid adenocarcinoma, grade 1or 2, or a premalignant condition (atypical hyperplasia), are eligible for fertility presentation, whereas patients with other histologies (serous carcinoma, clear cell carcinoma, carcinosarcoma) are ineligible.7 17 18
Among the literature on endometrial cancer and fertility-sparing, we selected three on MRI and one on MRI and ultrasound evaluation. In particular, we found three retrospective studies28–30 on MRI and endometrial cancer and one narrative review on MRI and ultrasound;31 and three articles (two descriptive studies6 7 and one narrative review5) reported fertility-sparing and gynecological cancer including data on MRI parameters for fertility preservation in endometrial cancer patients (Table 1). Myometrial and cervical stromal invasion: absence of myometrial and cervical invasion is required to consider fertility-sparing treatment.5–7 28–31MRI has high sensitivity in diagnosing myometrial invasion.28–31 However, very early myometrial invasion may be difficult to identify by MRI.7 Evidence of an uninterrupted low-signal-intensity junctional zone on T2WI is useful to exclude myometrial invasion and to confirm that tumor is confined to the endometrial canal.6 On DCE-MRI, the presence of a continuous rim of subendometrial enhancement of the inner junctional zone, evident within the first minute after contrast administration, helps to exclude myometrial infiltration. On T2WI, cervical stromal invasion is suspected when intermediate-to-high-signal-intensity tumor disrupts low-signal intensity cervical stroma.5 On DCE-MRI, stromal invasion is suspected when a hypo-enhancing tumor disrupts continuous enhancement of cervical epithelium.5
Absence of Synchronous Primary Ovarian Cancer or Ovarian Metastases
Synchronous or metastatic ovarian cancer in women with endometrial cancer is relatively uncommon, but this has to be excluded when considering fertility-sparing treatment.5–7 31 The presence of a large endometrial tumor and a small ovarian lesion may favor diagnosis of ovarian metastasis from endometrial cancer, whereas a small endometrial tumor and a large unilateral complex ovarian mass ±endometriosis raises the possibility of a synchronous primary ovarian malignancy.5
Regarding ultrasound examination, one narrative review has been published, describing ultrasound parameters for fertility preservation on endometrial cancer.31 Transvaginal ultrasound examination showed comparable accuracy to MRI scan and could be used in centers with difficult access to an MRI scan to define myometrial invasion and exclude suspicious ovarian lesions.31
Ultrasound Methodology
In our institution, preoperative evaluation of patients eligible for fertility preservation treatment is mainly based on transvaginal ultrasound examination or alternatively on MRI.
Endometrial lesions are described at ultrasound according to International Endometrial Tumor Analysis (IETA) terminology.32
Endometrial tumor is measured in three orthogonal diameters: anteroposterior (tumor thickness) and craniocaudal (tumor length) diameters, in the sagittal plane, and laterolateral diameter (tumor width), in the transverse plane.33 Color or power Doppler is used to assess the vascular pattern. Indeed, endometrial tumors with poor vascularization and with a “single vessel” patter are more indicative of a tumor of grade 1 and Stage IA than tumors with rich vascularization and multiple vessel patter that are more indicative of tumors at advanced stage. Moreover, one should measure the tumor-free margin in the plane in which one observes the smallest distance from the tumor to the serosa.34
The depth of myometrial invasion is evaluated subjectively and classified into no invasion,<50%, or ≥50% (Figure 5). Invasion of the cervix is diagnosed when the neoplastic tissue extends caudally merging with the endocervical mucosa. It is important to apply slight pressure with the transvaginal probe, in order to differentiate between mild protrusion of the endometrial tissue to the cervical canal and true infiltration of the endocervical mucosa.34 35 Finally, assessment of the adnexa is suggested to exclude adnexal masses.

Ultrasound, MRI and microscopic images of a 36 years' old patient with histological diagnosis of endometrial adenocarcinoma of grade 1 (histology obtained from previous polypectomy). Color Doppler image (a) shows an endometrium with homogeneous echostructure, no myometrial invasion, and a single dominant vessel penetrating into the endometrial tissue. sagittal T2-weighted MR image. (b) shows normal thickness endometrium with no evidence of myometrial invasion. No area of restricted diffusion at diffusion-weighted MR imaging or abnormal sub-endometrial contrast enhancement was observed within the inner myometrium (not shown). The patient underwent hysteroscopic ablation of the endometrium. Final histology (c) confirmed adenocarcinoma of grade 1 (zoom) with no myometrial invasion (black arrow).
MRI Protocol and Methodology
MRI protocol for the evaluation of a patient with endometrial cancer is similar to the previous one described for cervical cancer but with some differences. High-resolution T2-weighted sequences performed in the axial oblique and coronal oblique planes are respectively obtained perpendicular and parallel to endometrial cavity. Diffusion-weighted imaging is also performed in the sagittal and axial oblique planes in the same orientation as T2-wieghted planes (b=0 and 800–1000 sec/mm2) and apparent diffusion coefficient \maps obtained. DCE-MRI is essential for local staging of endometrial cancer because it is helpful in delineating myometrial invasion. DCE-MRI is acquired in the sagittal plane with delayed contrast-enhanced images acquired in the axial oblique plane (90–120 s after intravenous administration of gadolinium). Diffusion-weighted imaging should always be read in combination with T2WI sequences and contrast-enhanced images.
Endometrial cancer shows similar signal intensity on T2WI to the myometrium and relative hyperintensity to the adjacent low-signal junctional zone (inner myometrium). Most tumors enhance more slowly and less intensely than adjacent myometrium. Maximal tumor-to-myometrial contrast occurs at delayed phase after intravenous administration of gadolinium with DCE-MRI. Endometrial tumors show high-signal intensity on the high-b-value diffusion-weighted imaging and low signal on apparent diffusion coefficient maps. However, the normal endometrium also shows slight high signal on diffusion-weighted imaging due to its cellularity, but minor restriction compared with that of endometrial cancer.
MRI reports to assess eligibility for fertility-sparing treatment include:
Tumor information: diameter of the tumor on three axes, evaluated on sagittal plane for cranio-caudal (tumor length) and anteroposterior (tumor thickness) diameters, and on oblique axial for transvers diameter (tumor width); site of tumor within the endometrial cavity (corpus, fundus, anterior, or posterior wall; right or left side, cornus); absence or presence of myometrial invasion (<or >50%); and absence or presence of cervical stromal invasion (Figure 5).
Ovarian information: evidence of synchronous primary ovarian cancer or ovarian metastases
Lymph nodes information: absence or presence of pelvic or para-aortic nodal enlargement (short-axis diameter larger than 10 mm); and other suspicious lymph nodes characteristics consist of round morphology, irregular borders, and presence of necrosis.
Other findings in pelvis or abdomen: bladder, rectum, ovaries, liver, kidney, presence of peritoneal implants, bone.
Ovarian Cancer
Ovarian cancer is the leading cause of death among all gynecological cancers in developed countries, with most patients presenting with advanced stage. More than 90% of malignant ovarian tumors are of epithelial origin.19 20 36 37 According to international societies and guidelines, including NCCN, ESMO/ESGO/ESTRO, fertility-sparing surgery is based on unilateral salpingooophorectomy and complete surgical staging with preservation of the uterus and contralateral ovary. This is possible for most young women who desire future fertility and have any stage malignant germ cell tumors, sex-cord stromal tumors, borderline tumors, or early stage epithelial carcinomas.19 20 The key point is to avoid rupture of the mass.38
Among the literature on ovarian cancer and fertility-sparing options, we have selected two articles (a descriptive study6 and a narrative review5 on MRI); two studies (a prospective study39 and a narrative review4 on ultrasound evaluation); a prospective study40 on intraoperative ultrasound: and finally, one narrative review7 on fertility-sparing surgery and gynecological cancer, including data on MRI and ultrasound evaluation in ovarian cancer patients (Table 1). According to these articles, the eligibility criteria of fertility-sparing treatment on MRI and ultrasound should be based on the absence of extraovarian disease in young patients with ovarian masses suspicious for malignancy (borderline or invasive).4 5
The criteria for distinguishing between benign and malignant adnexal masses on MRI5–7 and ultrasound41 have been extensively described in the literature.
Ultrasound Methodology
Ovarian lesions are described as ultrasound according to International Ovarian Tumor Analysis (IOTA) terminology.41 In particular, ovarian tumor is measured in three diameters, in two perpendicular planes. The morphology aspect of the mass, cystic content, external and internal walls, presence of solid component, as well as of papillary projections, septum, and vascularization are reported (Figure 6).41 Based on pattern recognition in transvaginal examination, an expirienced examiner is able to provide high accuracy in selecting malignant lesions.42

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
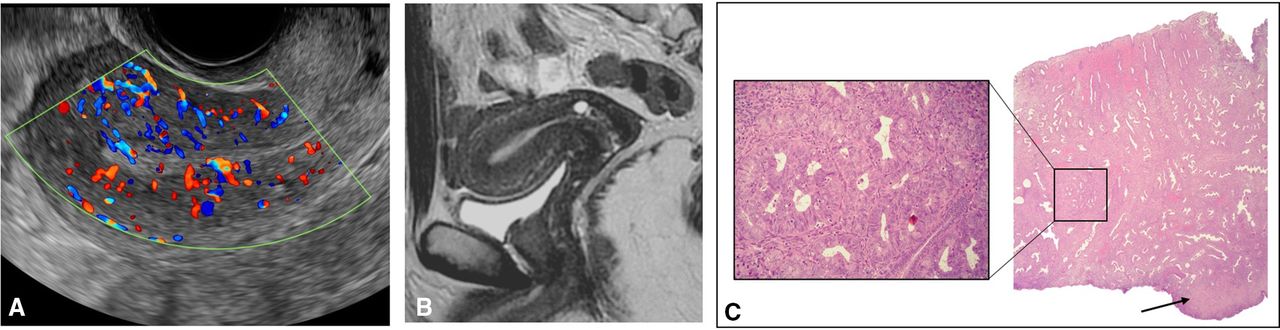
Ultrasound, MRI, and macroscopic images of a 29 years' old patient who underwent a left salpingoopherectomy for a left adnexal mass. Gray-scale ultrasound images (a) shows a left normal ovary (yellow arrow) and an exophytic mass (white arrow). Axial T2-weighted MR image (b) shows the left ovary (yellow arrow) with an exophytic mass (white arrow) with multiple nodular papillar projections with restricted diffusion at diffusion-weighted MR imaging and a type t2 curve (not shown). Macroscopy (c) confirmed the left exophytic tumor (white arrow) adjacent to normal ovary (yellow arrow). Final histology (d) was positive for serous borderline tumor with microinvasive foci.
The IOTA ADNEX model has been now extensively validated providing a high accuracy in discriminating between benign and malignant adnexal masses.43 This model is also able to provide the relative risk of each subgroups of malignancy (borderline, early stage, advanced, and metastatic tumors). However, the discrimination between borderline and invasive early-stage ovarian cancer, which is clinically relevant in planning the correct surgical treatment in young patients, remains a clinical challenge.44 45 Transvaginal examination is now able to identity ovarian lesions of very small size, thus representing a significant role in the follow-up of patients after fertility-sparing surgery.39 A large series of young women previously treated with fertility-sparing surgery and presenting with ovarian recurrences have been followed for a long period with transvaginal examination. It has been demonstrated that borderline ovarian recurrences can be detected at a very small size and the growth rate is about 1–2 mm/month. These findings are clinically useful in planning surveillance of these patients in order to plan a subsequent fertility-sparing surgery at the most appropriate time (ie, when the ovarian recurrence that had been detected in the inner part of the ovary is visible at the surface of the ovary).39 In some patients, an intraoperative ultrasound examination facilitated complete tumor excision in recurrent ovarian borderline tumors minimizing the removal of ovarian tissue.40 46 47 Regarding the preoperative assess of extraovarian disease, ultrasound examination demonstrated high specificity but low sensitivity in the detection of abdominal peritoneal carcinomatosis.48–50
MRI Protocol and Methodology
The MRI protocol for the evaluation of patients with ovarian cancer is similar to the previous one described for cervical cancer but with some differences. High-resolution T2-weighted sequences are performed in the sagittal, axial, and axial oblique T2WI planes. The axial oblique plane is obtained being parallel to the endometrial cavity (referred as “ovarian axis”), which can assist in visualizing the gonadal vessels to confirm the ovarian origin of the mass. Axial diffusion-weighted imaging is used for adnexal mass assessment (b=0 and 800–1000 sec/mm2) and apparent diffusion coefficient maps are obtained. Diffusion-weighted imaging should always be evaluated in conjunction with other sequences such as T2WI and contrast-enhanced images. It is fundamental for adnexal masses because both benign and malignant ovarian masses may show diffusion restriction (high-signal intensity on high b-value images and low-signal intensity on apparent diffusion coefficient maps).
DCE-MRI is acquired on the axial plane applying a dynamic multiphase approach or perfusion imaging. Perfusion imaging is performed for a minimum of 3 min after contrast administration with a temporal resolution less than 15 s. Perfusion images are evaluated by placing regions of interest on the most avidly enhancing portion of the ovarian mass and on the outer myometrium determining one of three types of time-intensity curves (using the enhancement of the outer myometrium as a reference). The Type 1 curve demonstrates a low level of enhancement without plateau, and indicates benignity. The type 3 curve, rapid high level of enhancement (faster than that of the myometrium), suggests possible malignancy. An in-between Type 2 curve, moderate level of enhancement with a plateau, may indicate for borderline ovarian tumor.
MRI characteristics that are highly predictive of benign disease include purely cystic morphology, cystic morphology with blood content as endometriomas, and purely fatty masses; absence of wall enhancement; and masses with solid components with low T2 signal intensity.7 When a solid enhancing mass is present a slow wash-in or a time-signal-intensity curve with slow gradual enhancement (Type 1 curve) is predictive of benign lesions.7 MRI characteristics indicative of malignant masses (Figure 6) are represented by complex solid cystic lesions whose solid components have intermediate T2 signal intensity and, when compared with the adjacent myometrium, demonstrating a rapid wash-in rate and more intense enhancement during dynamic contrast-enhanced MR imaging (Type 3 curve).7 However, an algorithmic evaluation of the adnexal mass can be used to determine the associated risk for malignancy (ADNEX MR Imaging Score).7 51
MRI reports to assess eligibility for fertility-sparing treatment in patients with ovarian cancer include:
Tumor information: evaluation of adnexal mass with description of risk of malignancy, as described above.
Other ovarian information: presence of preserved ipsilateral ovarian and evaluation of contralateral ovary.
Lymph nodes information: absence or presence of pelvic or para-aortic nodal enlargement (short-axis diameter larger than 10 mm). Other suspicious lymph nodes characteristics consist of round morphology, irregular borders, and presence of necrosis.
Other findings in pelvis or abdomen: presence of peritoneal implants, bladder, rectum, liver, kidney, bone.
Computer tomography (CT) staging. When a mass is suspected of being malignant on the basis of ultrasound examination, the detection of additional localization of disease in the pelvis and peritoneum becomes important for the detection of measurable disease beyond the mass, which would change the fertility preservation decision. CT is the current standard technique for this detection, as suggested by the National Institute for Health and Care Excellence, the European Society of Urogenital Radiology, and the American College of Radiology.12 However, CT has low sensitivity for the identification of small peritoneal nodules and unsatisfactory accuracy in the staging of early peritoneal disease.
Discussion
Ultrasound and MRI play a key role in selecting patients who might benefit from fertility preservation in cervical and endometrial cancers. There is also evidence supporting the fundamental role of both ultrasound and MRI in identifying adnexal masses, however, their efficacy in excluding metastatic disease outside the ovary in patients with ovarian cancers remains to be clarified. We recognize that our study is a narrative review and not a systematic review or metanalysis, lacking important requirements for quality control such as risk of bias, quality assessment, and statistical analysis. Our goal was to provide an overview of the literature on imaging and fertility preservation, and to offer parameters on the management of these patients in clinical practice.
Other reviews have focused on imaging and fertility-sparing surgery, however, most analyzed only data on MRI and cervical cancer,8 10 or MRI and gynecological cancers,5 and only one narrative review reported data on ultrasound and gynecological cancers.4 In particular, Rob et al,8 in a narrative review, evaluated the selection criteria based on MRI for the preservation of fertility in cervical cancer, but the authors manly focused on the surgical procedures of fertility-sparing rather than imaging data. De Boera et al10 conducted a systematic review on the accuracy of MRI in detecting involvement of the internal uterine os in cervical cancer patients, without providing which parameters are needed for selecting patients for fertility preservation. The authors found that MRI had a sensitivity of 91% and specificity of 97% in evaluating involvement of the internal os, using histology as a reference standard. Similar to ourstudy, McEvoy et al5 reported a narrative review on the role of imaging in the proper selection of patients with gynecological cancers for fertility preservation, but in that study the authors focused only on MRI. They found that MRI criteria were tumor size ≤2 cm, tumor-to-internal os distance ≥1 cm (or alternatively ≥0.5 cm), and cervical stromal invasion <50%, for cervical cancer: disease confined to the endometrium with the absence of any myometrial invasion and stromal invasion, absence of synchronous primary ovarian cancer, or ovarian metastases, for endometrial cancer. However, the authors did not report any specific indication for fertility preservation in ovarian cancer patients but only suggested that MRI is useful in discriminating between benign and malignant tumors.5 Fischerova et al4 described the ultrasound methodology of gynecological cancer staging, providing ultrasound criteria for selecting patients for fertility-sparing surgery. However, the authors were mainly based on methodology and sonographic features, with some clinical considerations in assessing local tumor extent, lymph nodes, and distant metastases by ultrasound examination.
In conclusion, fertility preservation is an integral component of clinical decision-making and treatment planning. Therefore, knowledge of the imaging parameters that guide clinicians in selecting patients who are candidates for fertility preservation is of the utmost importance. This review provides an update of the data used for the counseling and management of patients with a desire for fertility preservation. This study may provide an insight into areas that still need to be prospectively explored and may provide new perspectives for further multicenter studies.
Acknowledgments
We acknowledge Professor Gian Franco Zannoni and Dr Damiano Arciuolo, Fondazione Policlinico Universitario Agostino Gemelli, IRCCS, Rome, for macroscopic and microscopic images of clinical cases.
References
Footnotes
Contributors All authors contributed in the creation of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.