Article Text

Statistics from Altmetric.com
Case presentation
A 48-year-old woman presented in February 2020 with 2 weeks of vulvar pain and swelling on the right labium minus with associated intermittent tenderness. Past medical history was significant for hypertension. Past surgical history was significant for three conizations and a bilateral salpingectomy for tubal sterilization. Family history was unremarkable. At that time, the pelvic examination showed an indurated palpable 2×2 cm nodule involving the medial aspect of the right labium minus. The remainder of the external female genitalia revealed no other abnormalities. The inguinal lymph nodes were not palpable. The nodule was slightly painful during the examination. Speculum examination showed no vaginal lesions, a scarred cervix without obvious masses, no blood in the vault, and clear discharge. Bimanual examination revealed a normal size uterus, anteverted with a shortened cervix. The adnexa were not palpable. Rectovaginal examination was negative for nodularity or palpable masses. On presentation, the patient was afebrile.
Initial laboratory studies showed a white blood cell count of 7×103/µL and C-reactive protein <10 mg/L. Pelvic ultrasound showed a uterus measuring 7.1×5.4×4.2 cm. The endometrial stripe was 9 mm. The ovaries were normal. The patient was diagnosed with a Bartholin’s gland infection. The plan was for marsupialization. The intra-operative findings revealed a solid, white, well-circumscribed mass measuring 2 cm without firm adhesions to the surrounding tissue. The intra-operative findings changed the planned surgery and the mass was dissected, and the entire gland was resected without complications. The post-operative course was uncomplicated and the patient was discharged home the day after surgery.
Dr Andrade
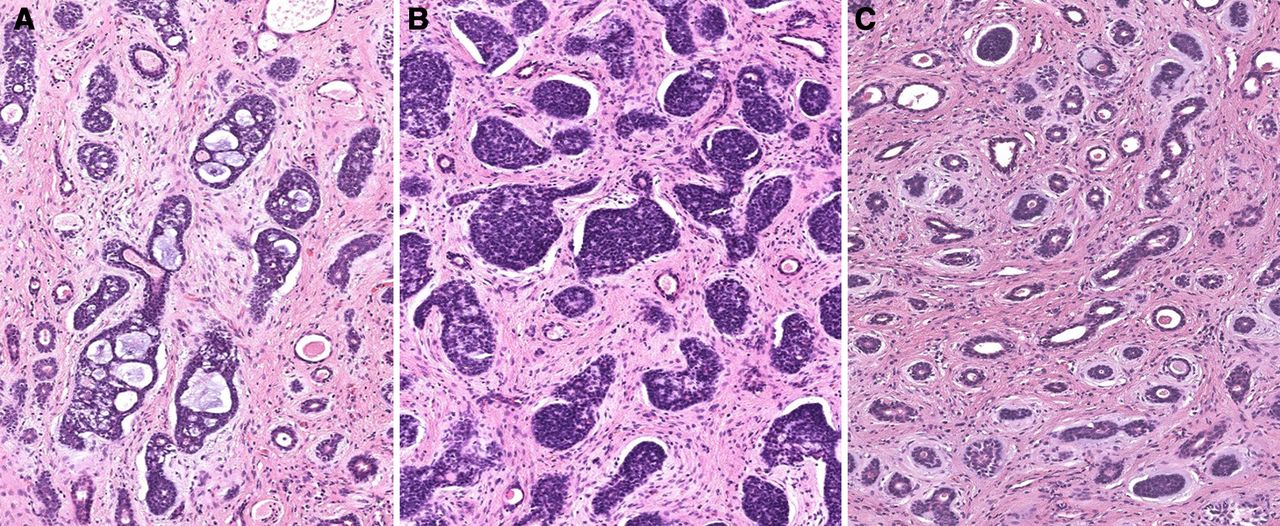
Gross tumor evaluation revealed the tumor size was 2.5 cm and the surgical margins were involved by invasive carcinoma. After the microscopic study the definitive diagnosis was adenoid cystic carcinoma of the Bartholin’s gland. Adenoid cystic carcinoma is a malignant tumor composed of a dual population of basal/myoepithelial and luminal cells (Figure 1). The cellular component is arranged in three main growth patterns: cribriform, solid, and tubular (Figure 2A–C). 1
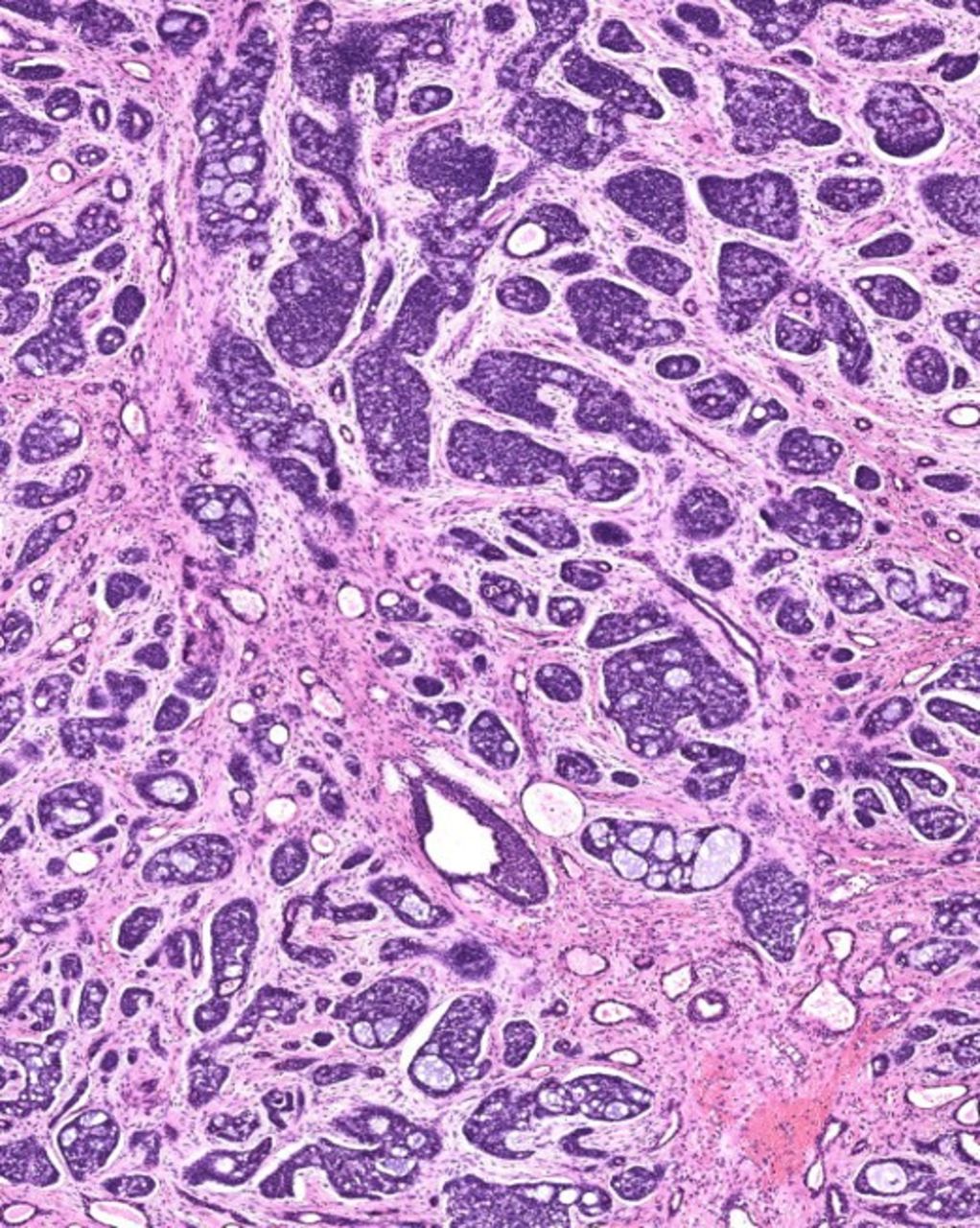
Adenoid cystic carcinoma with dual population of basal/myoepithelial and luminal cells.

(A) Cribriform pattern with multiple cribriform structures composed of epithelial and basal/myoepithelial cells. (B) Solid (basaloid) pattern with large solid sheets of tumor cells. Surrounding stroma is desmoplastic. (C) Tubular pattern with small tubules without significant cytological atypia.
Figure 2A Cribriform: This is the most characteristic microscopic feature, dominated by multiple cribriform structures composed of epithelial and basal/myoepithelial cells. The nuclei are usually dark, hyperchromatic, and angulated. The contents of the spaces can be loose and basophilic or dense and eosinophilic.
Figure 2B Solid (basaloid): This is dominated by large solid sheets of tumor cells. Within the solid masses of tumor cells there are small duct-like spaces surrounded by a definite layer of epithelial cells. The surrounding stroma is desmoplastic.
Figure 2C Tubular: This is composed of small tubules lined with one or two cell types, luminal and abluminal, without significant cytological atypia. 2
Adenoid cystic carcinoma may display considerable variability in staining for epithelial and myoepithelial markers. Immunochemistry for broad-spectrum keratins (CKAE 1–3) and myoepithelial cells (p63) was performed and revealed a strong positive expression (Figure 3). The most common differential diagnosis includes adenocarcinoma of skin appendage origin, metastatic adenocarcinoma, small cell carcinoma, and Bartholin’s glands adenocarcinoma. The latter lacks the uniform acinar arrangement and intraluminal basement membrane material of adenoid cystic carcinoma. Metastatic carcinoids and small cell carcinomas are more solid, have fewer lumens, and stain for neuron-specific enolase.

Immunochemistry for broad-spectrum keratins CKAE 1–3 and p63 demonstrating strong positive expression.
Adenoid cystic carcinoma is distinct from other sub-types of Bartholin’s gland carcinomas. It seems to arise from myoepithelial cells of the Bartholin’s gland. The morphology is identical to the adenoid cystic carcinoma of salivary glands or the upper respiratory tract and skin and tends to have extensive perineural invasion (Figure 4). Adenosquamous carcinoma of the Bartholin gland contains a mixture of squamous cells with intra-cellular bridges and glandular cells that typically contain mucin. The differential diagnosis with vulvar squamous cell carcinoma and basal cell carcinoma is the involvement of overlying squamous epithelium. 1 3 4

{kind=link}
{kind=link}
{kind=link}
{kind=link}
S100: Perineural infiltration.
Immunohistochemical staining for CK and CD117 is positive in the inner epithelial cells and p63 and SMA in the peripheral myoepithelial. In contrast, the immunohistochemical features of squamous cell carcinoma and basal cell carcinoma are typically immunoreactivity for CK5/6 and p63 and negative for SMA and S100. Adenocarcinoma is positive for CK 8/18 and CEA. 1 3 4 The mammary-like adenocarcinoma of the vulva is associated with benign mammary acini and ducts with breast cancer biomarkers, and its location is away from Bartholin’s gland. 5
The patient was referred to the Gynecology Oncology Department. In March 2020, to assess the local and distant extension of the disease, a post-operative pelvic MRI and a CT scan were performed without evidence of local or metastatic disease.
Dr Llueca
Based on the findings described at pathology, what should be the recommendation regarding additional surgery?
Because of the rarity of these lesions, treatment remains elusive and should be individualized, as there is no level I evidence available, given that data on the subject exist mostly as case reports. This patient was classified as a pT1B with a 2.5 cm tumor in the largest dimension. We consider it such a unifocal lateral vulvar tumor, less than 4 cm and without suspicious groin lymph nodes. Therefore, the European Society of Gynecology Oncology (ESGO) guideline 6 recommends imaging of the groins and a wide local excision. Regarding the lymph node dissection, it is required for authors who consider the adenoid cystic carcinoma as a vulvar tumor. 7 8 In contrast, others support wide local excision, with or without inguinal lymphadenectomy as initial treatment. 1
The limited available literature 9 suggests that a lymph node dissection may be restricted to those patients with high risk for nodal involvement. If performed, it should at least be limited to the ipsilateral side of the tumor. 9 10 Recent studies consider performing a lymphadenectomy just in case of suspicion of nodal involvement in the pre-operative imaging. 11 Approximately 65% of patients undergoing complete lymphadenectomy would have negative lymph nodes, therefore deriving no benefit from this procedure. 12 No lymph node metastasis was found in five patients with adenoid cystic carcinoma of Bartholin's glands to analyze the clinical outcomes before and after the primary treatment. 13 Therefore, most authors do not recommend lymphadenectomy unless there is a clinical or radiological suspicion of lymph node dissection as this tumor often metastases to distant organs before involving locoregional lymph nodes. 14–17 However, performing lymph node dissection is still a debate in treating this specific tumor, and sentinel lymph node biopsy with less morbidity than a full lymphadenectomy is an option for those who prefer a lymph node assessment. 12
Regarding the margins, the goal of excision is to obtain tumor-free pathological margins. A tumor-free surgical margin of at least 1 cm decreases local recurrence. 12 The ESGO guideline 6 advises surgical excision margins of at least 1 cm for all vulvar cancers. It is acceptable to consider narrower margins where the tumor lies close to midline structures such as the clitoris, urethra, or anus, and preservation of these structures is desired.
The patient was presented in the tumor board and several options, such as a partial vulvectomy or a re-excision to amplify the margins of the last surgery, were discussed. The multidisciplinary committee recommended repeat surgery to ensure adequate margins were resected. Three weeks later the surgery to obtain cancer-free margins was performed without complications. Frozen section evaluation revealed that all margins were more than 1 cm and free of tumor. The post-operative recovery was uneventful and the patient was discharged home on the day of surgery. No post-operative complications occurred. However, in the final report the inferior and deepest margins were involved by invasive carcinoma. Given these findings, the multidisciplinary committee discussed the case again and the recommendation was for radiotherapy as adjuvant treatment. The ESGO guideline6 suggests both options: re-excision if possible or radiotherapy. The risk/benefit and morbidity of both options must be considered and individualized in each patient.
The patient recovered from the surgery and underwent a post-operative CT scan, which did not show any evidence of enlarged lymph nodes or measurable distant metastatic disease. External beam radiotherapy was started in June 2020 and completed 1 month later. The patient completed a total dose of 50 Gy in fractions of 2 Gy per day for 5 days per week. The radiotherapy was well tolerated except for a grade 3 dermatitis in the vulvar and perineal region. This was treated with an oral antihistamine and a topical antimicrobial combined with an antibacterial mesh impregnated with fatty substances, hydrocolloid, and silver particles (Urgotul; Urgo Medical).
Dr Llueca
If the patient had shown evidence of metastatic disease at the completion of the second surgery, what would have been your recommendation at that time?
The prognosis of adenoid cystic carcinoma with distant metastasis is poor and the management is not well established. Overall, surgical resection is the primary treatment for this carcinoma. 3 12 If the metastasis is also resectable, a second surgery to obtain margin-free tumors with the resection of the metastasis will be the first option. 18 However, if the metastatic disease is unresectable, chemoradiotherapy will be the alternative. 6 19
In stage IV Bartholin’s gland carcinoma with infiltration of the bladder, rectum, proximal urethral mucosa, fixation to bone or distant metastases, neoadjuvant chemoradiation followed by no surgery or less radical surgery should be considered to avoid exenterative surgery required to obtain negative resection margins. 3 12 Exenterative surgery is very infrequently performed in patients with Bartholin’s gland cancer. In a review performed by Di Donato 3 with a total of 275 patients with cancer of the Bartholin’s gland (30.7% squamous cell carcinoma, 29.6% adenoid cystic carcinoma, 25% adenocarcinomas), only two patients (0.7%) underwent pelvic exenterative surgery. However, the risk of associated morbidities and the psychosexual impact of such procedures is high; after radical vulvectomy 89% of patients have sexual complications. 20 Thus, neoadjuvant chemoradiation such as 5-fluorouracil and cisplatin or bleomycin 12 with less radical surgery is the preferred approach for most patients with advanced disease.
Dr Llueca
Please provide details as to what should be the recommended surveillance for this patient?
Given the lack of international recommendations, the optimal follow-up schedule for this rare vulvar cancer is undetermined. In our institution, we opted for a combination of the vulvar cancer ESGO guidelines and the National Cancer Comprehensive Network (NCCN) guidelines for vulvar and salivary gland cancers. After primary surgical treatment, the first follow-up visit is scheduled 4 weeks after surgery, then every 3–6 months during the first 2 years and, thereafter, visits are planned every 6–12 months until 5 years, and then annually based on the risk of disease recurrence. 6 19 21
Follow-up after surgical treatment should include a clinical examination of the vulva and groins. Laboratory and imaging assessments are based on symptoms or examination findings suspicious for recurrence. Patient education regarding symptoms of potential recurrence and vulvar dystrophy and also periodic self-examinations are always recommended. 6
At the time of the last visit in August 2020, 1 month after the last treatment with external beam radiotherapy, the patient had resumed normal daily activities and the dermatitis had healed. Her next follow-up visit will be in November 2020.
Dr Llueca
If the patient develops metastatic recurrent disease in the future, what would be your recommendation at that time?
In a review of the literature published by Alsan et al 22 the lungs were the most common site of distant metastasis, followed by the liver and, less frequently, the bone; other sites reported are kidney and brain. 1 It is not feasible to have a large cohort or randomized studies on adenoid cystic carcinoma of Bartholin’s gland because of its low prevalence, making it difficult to obtain a consensus regarding its optimal treatment. However, our institutional recommendation in case of four or fewer metastases, considered oligometastases and depending on the affected organ, is that these could be treated with surgery or by stereotactic radiotherapy. This recommendation is based on results reported in the literature for other gynecologic cancers and adenoid cystic carcinomas from other primary sites such as salivary glands. 18 23 24 However, if there are multiple (polymetastasis) or unresectable metastases, chemotherapy may be an alternative.
Although no specific guideline for adenoid cystic carcinoma of the Bartholin’s gland has yet been established and chemotherapy is still under evaluation, according to a review of chemotherapy for adenoid cystic carcinomas of the head and neck tumors the response rates to chemotherapy are low and the response duration is generally short, and no standard chemotherapy regimen is recommended at this time. 25 However, Budd et al 26 reported complete remission of metastatic adenoid cystic carcinoma of the salivary gland using a combination of intravenous 5-fluorouracil 500 mg/m2 and adriamycin 30 mg/m2 every 4 weeks, and mitomycin-C on the first day and every 8 weeks at a dosage of 10 mg/m2. Yang et al 14 reported two cases of adenoid cystic carcinoma in a review where they found that a combination of methotrexate, dactinomycin, chlorambucil, adriamycin, and cyclophosphamide was reported for metastatic adenoid cystic carcinoma of the Bartholin’s gland. The authors used six cycles of combination chemotherapy consisting of cyclophosphamide (400 mg/m2), adriamycin (40 mg/m2), and cisplatin (60 mg/m 2 ) for one of the patients who developed recurrence 4 months after a lung resection of her first recurrence. Ten months after completion of chemotherapy the patient had stable disease.
In a phase 2 randomized trial, patients with recurrent salivary tumors with all kinds of histologies, 22 of whom had adenoid cystic carcinoma, were treated either with vinorelbine or with vinorelbine and cisplatin.The response rate was 15% (2/13 patients with adenoid cystic carcinoma) after vinorelbine monotherapy and 44% (4/9 patients with adenoid cystic carcinoma) after combination therapy. 27 In a recent study to evaluate the efficacy of chemotherapy with cyclophosphamide, doxorubicin, and cisplatin in patients with recurrent metastatic unresectable adenoid cystic carcinoma, 14 patients received a combination of cyclophosphamide 750 mg/m 2 , cisplatin 60 mg/m 2 , and doxorubicin 40 mg/m 2 , all administered intravenously on day 1 every 3 weeks. Chemotherapy was continued for a maximum of six cycles. The median patient age was 49 years and the patients received a median of five treatment cycles. Two patients had a partial response, 10 patients showed stable disease, and two patients have progressive disease. The response rate was 14.3% and the disease control rate was 85.7%. Median progression-free survival was 5.7 months and the median overall survival was 23.4 months. 28
Furthermore, new agents are in development. A phase 2 trial including 32 patients with recurrent or metastatic adenoid cystic carcinoma regardless of the primary site showed a disease control rate of 90.6% (partial response of 15.6% and stable disease in 75%) for the multitargeted tyrosine kinase inhibitor, lenvatinib. 29 However, none of the primary tumors originated in the Bartholin’s gland.
Given the lack of evidence-based options for recurrent or metastatic adenoid cystic carcinoma specifically in the Bartholin’s gland, the current NCCN guideline for head and neck cancers 19 may be helpful in the decision-making process in the real-world clinical practice. The guideline includes cisplatin/doxorubicin/cyclophosphamide (category 2B) and cisplatin/vinorelbine as other recommended chemotherapy options for recurrent, unresectable, or metastatic salivary gland tumors. Adding lenvatinib (category 2B) is also considered in certain circumstances for adenoid cystic carcinoma.
Dr Llueca
Closing summary
Adenoid cystic carcinoma of the Bartholin’s gland is an extremely rare tumor without an established diagnostic and treatment. Despite its rarity, a neoplasm of the Bartholin’s gland is an important differential diagnosis to consider in women presenting with a mass in this gland, particularly in patients over 40 years of age. Any solid lesion or Bartholin’s gland enlargements should initially be biopsied to rule out underlying carcinoma. 3 Even when a drainage and marsupialization surgery is performed, taking several biopsies instead of needle aspiration biopsy is recommended in order to achieve a definitive diagnosis. 30
All patients should undergo an evaluation of the extent of local and metastatic disease. Translabial ultrasonography has been described as a valid and cost-effective tool for early evaluations in the presence of a solid vascularized lesion, especially in elderly patients. Abdominal and pelvic CT scan has been described to determine the local and lymph nodal extent of the disease. MRI was used mainly to evaluate the anterior infiltration of the urethra or posterior invasion of the rectum. However, until now, no imaging modality has been shown to be superior to others in evaluating the extension of disease and deep pelvic lymph node metastasis. 3
Routine lymphadenectomy does not appear to improve survival and prognosis. 13 A recent study constructed a prognostic nomogram combined with the clinical features and treatment options of adenoid cystic carcinoma to predict the disease-specific survival of patients diagnosed with adenoid cystic carcinoma in different anatomic sites, including genital sites. Its results demonstrated a markedly decreased survival for patients with adenoid cystic carcinoma with lymph node involvement. 31 Anatomic studies failed to identify the lymph vessels of Bartholin’s gland. We must therefore assume that the lymphatic channels are the same as those supplying the vulva and lower portion of the vagina. Some authors consider that the vulva is an area within which there is free communication between the lymphatic vessels of either side. 3 While the lymphatic drainage of the Bartholin’s gland is not entirely clear, the role of the lymphadenectomy remains unknown. Therefore, one may consider the sentinel lymph node as the best option in these patients if feasible.
Unlike squamous vulvar cancer, which is often caused by human papillomavirus (HPV), adenoid cystic differentiation may be sub-classified into two distinct groups based on the presence or absence of high-risk HPV. Cervical and vulvar mixed carcinomas with some adenoid cystic differentiation are high-risk HPV-related. However, pure adenoid cystic carcinomas of vulvar and cervical origin appear to be unrelated to high-risk HPV. 32 33 The hypothesis that HPV does not play a role in the pathogenesis of pure adenoid cystic carcinoma of Bartholin's gland was confirmed in two cases by Nakamura et al in 2020, 34 given that p16 expression was not detected in either patient. Thus, other mechanisms must be responsible for the development of these tumors.
The study by Nakamura et al 34 was the first to report the genomic profiling of adenoid cystic carcinoma of Bartholin’s gland using targeted gene sequencing to analyze 160 cancer-related genes in two patients. Cytogenetic analysis of vulvar adenoid cystic carcinomas has shown that chromosomal translocation involving the genes encoding the transcription factors MYB and NFIB functions are the driving force of adenoid cystic carcinomas regardless of anatomic site of origin. Novel chromosome translocations involving NFIB but with an intact MYB (MYBL1-NFIB gene fusion involving t(8;9)) likely occur in a sub-set of vulvar adenoid cystic carcinomas, indicating the presence of novel oncogenic mechanisms. Togashi et al 35 also detected MYB or MYBL1 locus rearrangements in 97 of 100 adenoid cystic carcinomas examined, suggesting that the fundamental alteration in the development of adenoid cystic carcinoma is a dysregulated overexpression of the two domains in MYB or MYBL1 led by translocation of super-enhancers (mostly those of NFIB) in the proximity of MYB or MYBL1. Given its high frequency, MYB/MYBL1 locus rearrangement might constitute a sensitive diagnostic marker for this tumor. However, the diversity of the rearrangements was also shown and, thus, the method of detection needs further clarification.
KRAS and KDM6A mutations were detected in tumor samples collected from each patient in the study by Nakamura et al. 34 KRAS mutations have not been previously reported in salivary gland adenoid cystic carcinomas, suggesting that one might have discovered a novel pathway related to adenoid cystic carcinoma of the Bartholin’s gland carcinogenesis, which could in turn provide a novel therapeutic target. However, KDM6A mutations, which are related to chromatin remodeling, are often reported in salivary gland adenoid cystic carcinomas suggesting that the genetic profile of adenoid cystic carcinoma of Bartholin’s glands could be similar to adenoid cystic carcinomas of the salivary gland and facilitate novel gene-targeted therapy, including the use of sensitivity to bromodomain and extra-terminal motif (BET) protein inhibitors and romidepsin, a histone deacetylase inhibitor (HDAC). Future research into the detailed roles of these chromosome translocations and the unique genetic pathways involved in carcinogenesis will potentially allow for improved gene-targeted therapy as a step toward developing precision medicine strategies (Table 1).
Adenoid cystic carcinoma has a high predisposition to infiltrate into adjacent tissues, often metastasizing to neighboring nerves leading to perineural invasion. There is some dispute about the association between perineural invasion and survival. The head and neck studies of this tumor showed that intraneural invasion was an independent predictor of poor survival and recurrence. Its presence is often associated with positive margins. 31 34 The tendency for extensive perineural invasion combined with delayed diagnosis characterizes adenoid cystic carcinoma as high risk of local recurrence and late distant metastases. However, patients with adenoid cystic carcinoma in the Bartholin’s gland generally have a good prognosis. Even in the presence of repeated local recurrence and/or distant metastases, 32 approximately more than 80% of patients were alive at 5 years, according to a review published in 2017. 3
The prognosis of adenoid cystic carcinoma has been reported in a few studies with population-based data; however, these analyses were limited to the head and neck or a single site and did not compare different anatomic sites. The studies reporting on survival rates of adenoid cystic carcinoma of Bartholin’s gland are not recent studies. Survival rates reported by Lelle et al 10 were 71% and 59% at 5 and 10 years. Overall survival rates at 5, 10, and 15 years were 71%, 50%, and 51%, respectively, as reported by Copeland et al. 36 Patients in this study were treated with cyclophosphamide, radiotherapy, or a combination of excision and radiotherapy or radical surgery and radiotherapy. However, cases with hematogenous distant metastasis occurring after a long disease-free period have also been reported.17
Yang et al 14 summarized the recurrence rate according to resection margin status in a literature review. The resection margin status was known in 45 patients, and the recurrence rates were 52.9% in the margin positive group and 52.1% in the margin negative group. Nevertheless, half of the patients with a positive resection margin had adjuvant radiotherapy, which could explain the result in part. In contrast, of 27 patients with a negative resection margin, six (22.2%) had adjuvant radiotherapy. There is also a limitation in evaluating the importance of resection margin status and primary treatment given that follow-up times are not routinely specified. Adjuvant radiotherapy is thought to reduce the recurrence rate for patients with positive surgical margins with deep local and perineural invasion.
Neoadjuvant chemotherapy or in combination with radiotherapy can avoid ultraradical surgery and inherent complications to patients. However, in later stages the resection frequently needs to be enlarged, and it is sometimes necessary to perform a pelvic exenteration, but these patients can be either treated with neoadjuvant chemotherapy or primary chemoradiation followed by tailored surgery. In the literature, neoadjuvant treatment consisted of external radiotherapy of the vulva plus the inguinal and pelvic areas with cisplatin or 5-fluorouracil. 12 Surgical procedures after this regimen showed no residual tumor for the majority of the patients and complete pathological response in 47–75% of patients. 37
Guidelines for post-operative chemotherapy or chemoradiotherapy for adenoid cystic carcinoma of the Bartholin’s gland are not established. Reported chemotherapy regimens in adjuvant setting or palliation include a variety of drugs such as methotrexate, dactinomycin, doxorubicin, cyclophosphamide, and cisplatin, alone or in combination. However, all of these regimens tend to induce considerable hematologic as well as non-hematologic toxicities. 11 A case report on the use of chemoradiotherapy for a patient with a positive margin instead of a new resection was published by Takatori et al. 38 The dose for whole pelvc irradiation was 59.4 Gy in 33 fractions combined with irinotecan 50 mg/m 2 . A grade 2 neutropenia (1024 neutrophils/mm 3 ), grade 2 anemia (9.4 g/dL), grade 1 nausea, and grade 2 radiation dermatitis were observed as manageable adverse events. After 24 months since treatment completion, the patient was free of recurrence.
In conclusion, adenoid cystic carcinoma is a rare form of vulvar cancer. These tumors are slow-growing but are locally aggressive and have a high recurrence rate. Early diagnosis by a biopsy to rule out underlying carcinoma in patients with a mass in the Bartholin’s gland is recommended. Although there is no standard recommendation for the treatment of this disease, one should aim for a margin-free resection (at least 1 cm), and sentinel lymph node biopsy may be considered a valid option. Radiotherapy should be considered as adjuvant treatment if the margins are positive. Chemoradiation is the treatment of choice in patients with unresectable disease in locally advanced stages, similar to the recommendation for the squamous cell carcinoma in the NCCN and ESGO guidelines. 6 21 Surgery should be considered in cases of oligometastasis (<4 metastases) and resectable disease in patients with good performance status. As we learn more about the oncogenic mechanisms of this rare tumor, molecular tests and gene-targeted therapy may be developed to achieve more precise management of adenoid cystic carcinoma of Bartholin’s gland.
References
Footnotes
Twitter @BSegarraVidal
Contributors BS and SCM are the co-authors who decided to publish this case. PAC is the pathologist who reviewed the case and images and answered the questions related to the pathology issues. ALA is the expert who answered the questions about the treatment and management of the case.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Commissioned; externally peer reviewed.