Article Text

Abstract
Objective Ovarian suppression is recommended to complement endocrine therapy in premenopausal women with breast cancer and high-risk features. It can be achieved by either medical ovarian suppression or therapeutic bilateral salpingo-oophorectomy. Our objective was to evaluate characteristics of patients with stage I–III hormone receptor positive primary breast cancer who underwent bilateral salpingo-oophorectomy at our institution.
Materials and methods Premenopausal women with stage I–III hormone receptor positive primary breast cancer diagnosed between January 2010 and December 2014 were identified from a database. Patients with confirmed BRCA1/2 mutations were excluded. Distribution of characteristics between treatment groups was assessed using χ2 test and univariate logistic regression. A multivariate model was based on factors significant on univariate analysis.
Results Of 2740 women identified, 2018 (74%) received endocrine treatment without ovarian ablation, 516 (19%) received endocrine treatment plus ovarian ablation, and 206 (7.5%) did not receive endocrine treatment. Among patients undergoing ovarian ablation 282/516 (55%) received medical ovarian suppression, while 234 (45%) underwent bilateral salpingo-oophorectomy. By univariate logistic analyses, predictors for ovarian ablation were younger age (OR 0.97), histology (other vs ductal: OR 0.23), lymph node involvement (OR 1.89), higher International Federation of Gynecology and Obstetrics (FIGO) stage (stage II vs I: OR 1.48; stage III vs I: OR 2.86), higher grade (grade 3 vs 1: OR 3.41; grade 2 vs 1: OR 2.99), chemotherapy (OR 1.52), and more recent year of diagnosis (2014 vs 2010; OR 1.713). Only year of diagnosis, stage, and human epidermal growth factor receptor 2 (HER-2) treatment remained significant in the multivariate model. Within the cohort undergoing ovarian ablation, older age (OR 1.05) was associated with therapeutic bilateral salpingo-oophorectomy. Of 234 undergoing bilateral salpingo-oophorectomy, 12 (5%) mild to moderate adverse surgical events were recorded.
Conclusions Bilateral salpingo-oophorectomy is used frequently as an endocrine ablation strategy. Older age was associated with bilateral salpingo-oophorectomy. Perioperative morbidity was acceptable. Evaluation of long-term effects and quality of life associated with endocrine ablation will help guide patient/provider decision-making.
- surgical oncology
- gynecologic surgical procedures
Statistics from Altmetric.com
HIGHLIGHTS
Ovarian ablation for adjuvant breast cancer treatment was offered to women with high-risk features
A total of 45% of patients undergoing ovarian ablation had therapeutic bilateral salpingo-oophorectomy
Complication (5.4%) and readmission (1.8%) rates after bilateral salpingo-oophorectomy were low
Introduction
In 2020, an estimated 276 480 women will be diagnosed with breast cancer in the United States.1 Approximately 85% of newly diagnosed breast cancers are hormone receptor positive,2 92% being potentially curable stage I–III disease.3 Among women with hormone receptor positive breast cancer, 19–30% are younger than 50 years at the time of diagnosis.3 Traditionally, premenopausal women were treated with tamoxifen for 5 years,4 allowing a switch to an aromatase inhibitor if a postmenopausal state was reached. This changed following the SOFT and TEXT trial results,5 6 published in 2014. Especially in premenopausal women who had undergone adjuvant chemotherapy due to high-risk features, adding an aromatase inhibitor with ovarian suppression resulted in significant improvement in disease-free survival (71.4% tamoxifen alone vs 80.4% exemestane plus ovarian suppression).7 Bui and colleagues performed a systematic Cochrane review and meta-analysis that included 15 earlier trials to evaluate the effects of ovarian ablation for the treatment of premenopausal women with hormone receptor positive breast cancer.8 The authors found evidence to support the addition of ovarian ablation in this patient population, with persisting benefit compared with observation, or when added to tamoxifen, or when added to chemotherapy and tamoxifen.
Bilateral salpingo-oophorectomy is an accepted alternative to medical ovarian suppression,9 but is irreversible. Due to current recommendations,10 11 premenopausal women with high-risk features commit to ovarian ablation and prolonged endocrine therapy. Ovarian function can be suppressed either with gonadotrophin-releasing hormone agonists (GnRHa) goserelin, leuprolide, or triptorelin administered subcutaneously monthly or 3-monthly, by ovarian irradiation, or surgical bilateral salpingo-oophorectomy.10 Because of the resulting implications for fertility and family planning, some patients may choose definitive surgical ablation. However, data are lacking about use and timing of therapeutic bilateral salpingo-oophorectomy. We sought to evaluate the patient, disease, and treatment characteristics of premenopausal women undergoing bilateral salpingo-oophorectomy, compared with women receiving medical ovarian suppression, as part of adjuvant treatment of hormone receptor positive breast cancer. This information will provide an insight into the current use of bilateral salpingo-oophorectomy in this population, and may improve patient/provider decision-making.
Methods
Database and patient selection
This study was approved by our institutional review board. We performed a retrospective review of a prospective institutional breast cancer database, identifying all premenopausal women with hormone receptor positive (estrogen or progesterone receptor >1%) breast cancer diagnosed between January 2010 and December 2014 who underwent mastectomy or breast conserving surgery and either neoadjuvant or adjuvant medical treatment. Premenopausal status was determined by the clinician at initial consult and was defined by regular menses without exogenous hormones before treatment initiation. This period was chosen to capture all patients undergoing bilateral salpingo-oophorectomy in the first 5 years of adjuvant treatment. Clinical, pathological, and treatment variables were collected; 3321 women were identified (Figure 1). Any malignant histology was included and assigned to one of five categories: any ductal no lobular; any lobular no ductal; both lobular and ductal; inflammatory; other. Women who did not undergo breast surgery, presented more than 90 days from initial diagnosis, who had stage IV disease, or a known BRCA mutation, or insufficient documentation were excluded. A total of 2740 premenopausal women with stage I–III were included in the final analysis and assigned to the following groups: group 1, no endocrine therapy; group 2, endocrine therapy without ovarian suppression; group 3, endocrine therapy with medical ovarian suppression; or group 4, endocrine treatment with bilateral salpingo-oophorectomy at any time point. Patients receiving medical ovarian suppression (leuprorelin or goserelin) at any point during adjuvant treatment were assigned to group 3 unless ovarian suppression was started after a recurrence or a bilateral salpingo-oophorectomy was performed. Women undergoing bilateral salpingo-oophorectomy after documented relapse, progression of disease, or for other reasons (adnexal mass, ovarian cancer, uterine cancer) were not classified in group 4 for the primary diagnosis; instead these patients were assigned to groups 1–3 irrespective of the endocrine treatment they had received prior to recurrence.
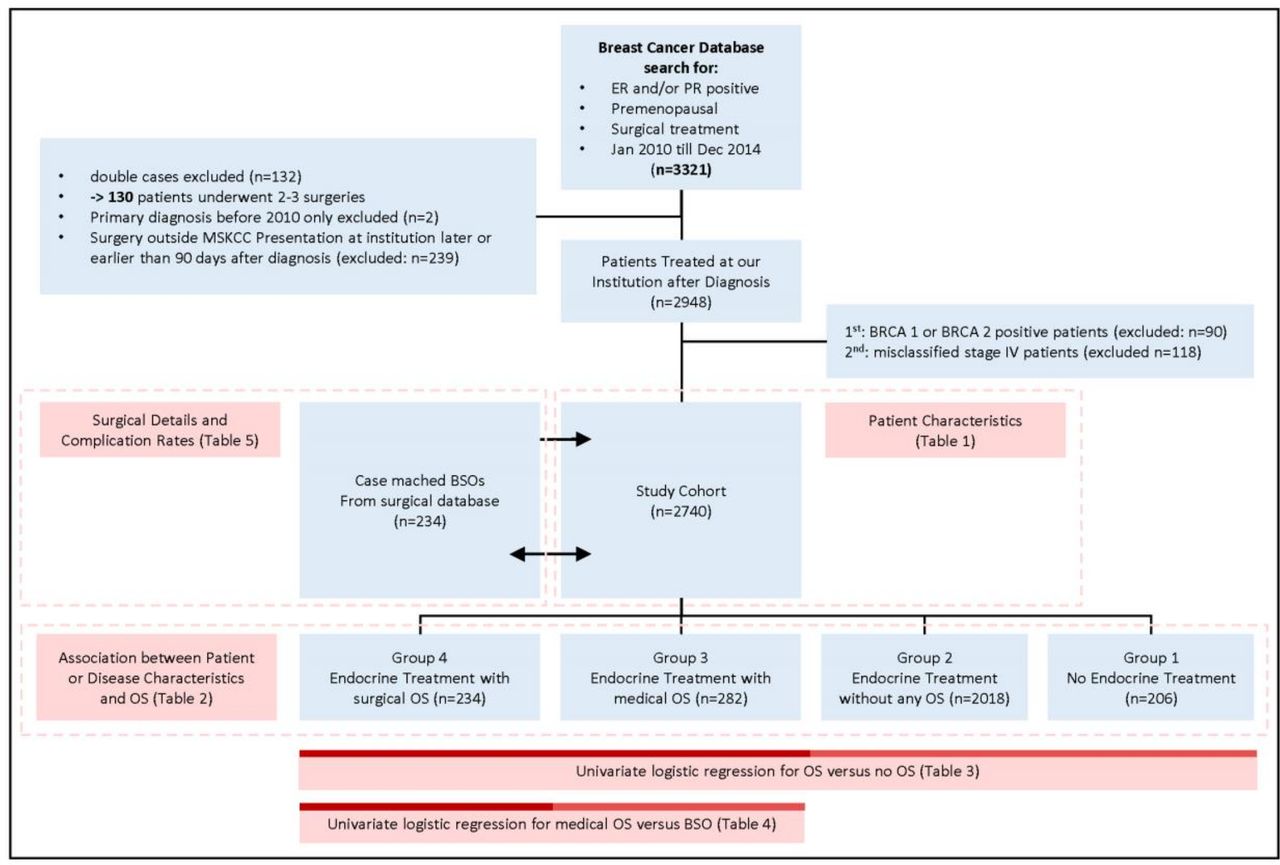
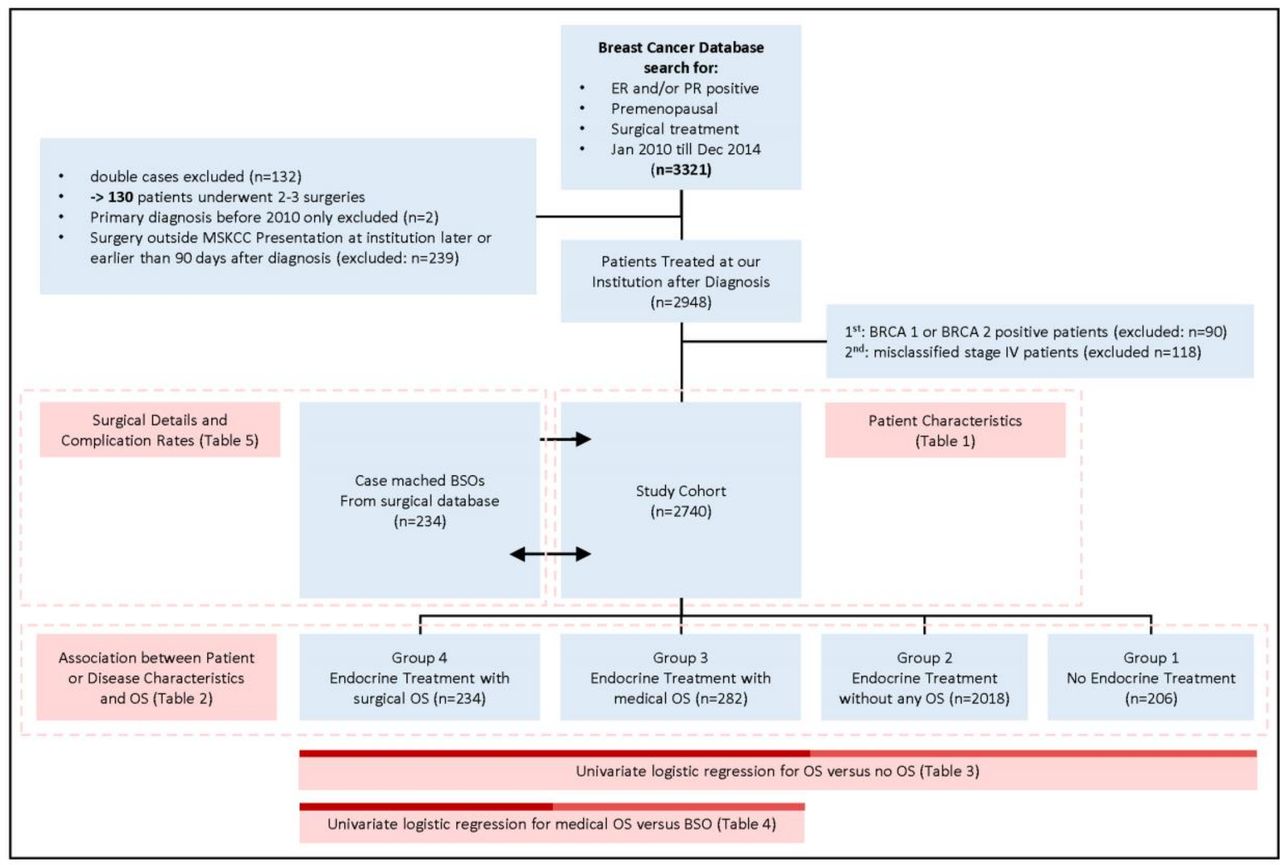{kind=link}
Study cohort selection. BSO, bilateral salpingo-oophorectomy; ER, estrogen receptor; OS, ovarian suppression; PR, progesterone receptor.
For bilateral salpingo-oophorectomy, gynecological oncologists were consulted and minimally invasive surgery was the preferred method. Surgical details and complications were extracted from the gynecological oncology surgical database. Complications were recorded and graded on a 1–5 scale according to a previously published classification system.12
Statistical analysis
Association between the treatment groups and patient or disease characteristics was assessed using the χ2 test/Fisher’s exact test for categorical variables and Kruskal-Wallis test for continuous variables. Two sets of univariate logistic regression analyses were performed to identify predictors among patient and tumor characteristics. The first regression analysis compared women undergoing any type of ablation (medical ovarian suppression and bilateral salpingo-oophorectomy) with those who did not. A multivariate logistic model was created, based on all the variables with p less than 0.05 in univariate analysis. The second regression analysis was performed among all ovarian ablation patients, comparing those receiving medical ovarian suppression versus bilateral salpingo-oophorectomy. Microsoft Excel was used for data collection, SAS9.4 for statistical analyses.
Results
Patient demographics
The final cohort comprised 2740 premenopausal women with a primary diagnosis of hormone receptor positive breast cancer during the study period, with median follow-up of 62.2 months (IQR 47.7–81.1) (Table 1). Median age was 45 years (IQR 40–48). Half (n=1445; 54%) of the study cohort had a family history of breast cancer. Most (n=1991; 73%) had children at the time of diagnosis. Most cancers were ductal histology (n=2188; 80%), poorly differentiated (tumor grade 3; n=1694; 67%). One-third (n=991; 36%) of women had lymph node involvement. The majority were diagnosed with International Federation of Gynecology and Obstetrics (FIGO) stage I (n=1377; 54%) or II (n=846; 33%) disease; 307 (12%) with stage III. Most received adjuvant or neoadjuvant chemotherapy (n=1720; 63%), adjuvant endocrine therapy (n=2527; 92%), or human epidermal growth factor receptor (HER-2) targeted treatments (n=434; 16%). Of 516 receiving ovarian ablation, 234 (45%) had bilateral salpingo-oophorectomy and 282 (55%) underwent medical ovarian suppression.
Patient and disease characteristics (n=2740)
Distribution of treatment groups
Patients were assigned to four groups (Table 2): roup 1 (n=206; 11%), no endocrine treatment; group 2 (n=2018; 74%), any endocrine treatment without ovarian ablation; group 3 (n=282; 10%), any endocrine treatment with medical ovarian suppression; or group 4 (n=234; 9%), therapeutic bilateral salpingo-oophorectomy at any time during primary treatment. Median follow-up for women receiving endocrine treatment without or with ovarian suppression (groups 2 and 3) was 64.1 (IQR 48.9–82.7) and 60.1 (IQR 49.2–77.7) months, respectively. Median follow-up for women undergoing bilateral salpingo-oophorectomy was 67.3 months (IQR 51.9–84.4).
Distribution of patients and disease characteristics between treatment groups
Neither family history of breast cancer nor history of giving birth to one or more children showed an association with any treatment group. All other characteristics—histological subtype, lymph node status, tumor grade, chemotherapy, HER-2 targeted treatment, age at diagnosis—were unevenly distributed between the groups.
Factors associated with ovarian suppression
Univariate logistic regression was performed (Table 3). Women who did not receive ovarian ablation (group 1—no endocrine, group 2—endocrine without ovarian suppression) were pooled and compared with those undergoing either medical ovarian suppression or bilateral salpingo-oophorectomy (group 3—ovarian suppression, group 4—bilateral salpingo-oophorectomy). Younger age (OR 0.98; 95% CI 0.96 to 0.99; p=0.001), more recent diagnosis (2014 vs 2010; OR 1.71; 95% CI 1.27 to 2.31; p<0.001), higher-grade tumors (grade 3 vs 1: OR 3.41; 95% CI 1.95 to 5.95; grade 2 vs 1: OR 2.99; 95% CI 1.67 to 5.33; p<0.001), lymph node involvement (OR 1.89; 95% CI 1.56 to 2.30; p<0.001), higher FIGO stage (stage II vs I: OR 1.48; 95% CI 1.18 to 1.86; stage III vs I: OR 2.86; 95% CI 2.15 to 3.80), uncommon histology (other vs ductal: OR 0.23; 95% CI 0.10 to 0.58; p=0.019), or chemotherapy (OR 1.52; 95% CI 1.23 to 1.87; p<0.001) were associated with likelihood of either medical ovarian suppression or bilateral salpingo-oophorectomy. Positive family history, and children, were not associated with ovarian ablation.
Univariate logistic regression for patients undergoing endocrine treatment without ovarian ablation (group 1 and group 2: n=2224) versus with ovarian ablation (group 3 and group 4: n=516)
A multivariate model using all patient and disease characteristics showed significance on univariate analyses (online supplemental table S1). With existence of other covariates in the same model, only more recent year of diagnosis (2014 vs 2010; OR 1.557; 95% CI 1.11 to 2.24), higher stage (stage III vs I: OR 2.26; 95% CI 1.37 to 3.72), and HER-2 treatment (trastuzumab plus other vs no HER-2 targeting; OR 2.39; 95% CI 1.342 to 4.231) were significantly associated with medical ovarian suppression or bilateral salpingo-oophorectomy.
Supplemental material
A subgroup analysis was performed for all women receiving ovarian ablation, comparing group 3—ovarian suppression versus group 4— bilateral salpingo-oophorectomy (Table 4). Older age at diagnosis (1.05; 95% CI 1.02 to 1.08; p<0.001) was associated with higher likelihood of bilateral salpingo-oophorectomy. For all other patient and disease characteristics there were no significant differences in distribution between bilateral salpingo-oophorectomy and medical ovarian suppression.
Univariate logistic regression for patients undergoing bilateral salpingo-oophorectomy (n=234) versus ovarian suppression (n=282) for ovarian ablation
In total, 335 women started medical ovarian suppression; 53 of these underwent bilateral salpingo-oophorectomy later. When comparing these 53 with the 282 who received only medical ovarian suppression, older age was the only factor associated with bilateral salpingo-oophorectomy (p=0.035).
Timing of ovarian ablation
Endocrine treatment began after a median of 6.7 months (IQR 4.3–8.6) in all three treatment groups (group 2: 6.8, IQR 4.4–8.7; group 3: 6.3 months, IQR 3.7–8.3; group 4: 6.6 months, IQR 3.8–8.4). Median time from diagnosis to any type of ovarian suppression was 12.4 months (IQR 64–28.4) (online supplemental table S2).
In group 3, 119 women started endocrine therapy and medical ovarian suppression at the same time; 135 had medical ovarian suppression after a median endocrine treatment time of 13.6 months (IQR 4–34). Median time from diagnosis to bilateral salpingo-oophorectomy was 22.9 months (IQR 13.5–37.7). Most women undergoing bilateral salpingo-oophorectomy (n=193, 93%) received endocrine therapy without medical ovarian suppression for a median of 18.3 months (IQR 9.4–34.7) before bilateral salpingo-oophorectomy. Of 234 patients undergoing bilateral salpingo-oophorectomy, 53 (22%) started medical ovarian suppression and had bilateral salpingo-oophorectomy later. For women crossing over to bilateral salpingo-oophorectomy, median time from first administration of medical ovarian suppression to bilateral salpingo-oophorectomy was 11.7 months (IQR 5.95–22.8).
Complications of surgical ovarian ablation
The majority (n=192, 85%) underwent outpatient surgery (Table 5); 33 (15%) had inpatient surgery. Median length of hospitalization was 0 (range 0–7). Most surgeries were laparoscopically (n=152, 67%) or robotically assisted (n=62, 27%); 14 (6%) were laparotomies. All laparotomies included additional abdominal procedures at the time of bilateral salpingo-oophorectomy. Eighty-nine women (39%) undergoing bilateral salpingo-oophorectomy had concomitant surgical procedures, including breast reconstruction (46, 20%), hysterectomy (35, 15%), hernia repair, vulvar surgery, or additional intraabdominal resections (24, 11%). Twelve (5%) had postoperative complications with four readmissions. Among those undergoing bilateral salpingo-oophorectomy without concomitant surgery, 2 (1.5%) had complications with one readmission. Grade 1 complications were documented in two patients: one urinary tract infection after laparoscopic bilateral salpingo-oophorectomy, and one postoperative wound infection and seroma after laparotomy for total abdominal hysterectomy/bilateral salpingo-oophorectomy in a patient with diabetes. Grade 2 complications included a wound infection requiring readmission for intravenous antibiotics after laparoscopic bilateral salpingo-oophorectomy with concomitant breast surgery, and symptomatic anemia requiring transfusion after robotic-assisted total laparoscopic hysterectomy/bilateral salpingo-oophorectomy. One patient was readmitted for a grade 3 pelvic hematoma requiring drainage; she had a history of peritonitis with adhesions, requiring conversion to laparotomy with enterolysis for bilateral salpingo-oophorectomy.
Surgical details and complication rates of bilateral salpingo-oophorectomy in the study cohort
Median duration of surgery was 95 min (IQR 53.2–145.8). Eighty-four (38%) patients had an operative time greater than 120 min. Twenty-five (11%) had an operative time greater than 180 min; in 24 of these 25, combined surgical procedures were performed. Median blood loss was 20 mL (range 0–1000). Among women undergoing bilateral salpingo-oophorectomy only, median surgical duration was 62 min (IQR 40–92); 16 (12%) exceeded 120 min.
Discussion
In this study, we assessed the characteristics of premenopausal women undergoing surgical ovarian ablation compared with women receiving medical ovarian suppression for hormone receptor positive breast cancer at our institution. Of 2740 women identified, 516 (19%) were treated with medical or surgical ovarian ablation. Those selected for ovarian ablation presented with high-risk tumor features (higher tumor grade or stage, lymph node involvement), or were younger at the time of diagnosis. Among those selected for ovarian ablation, older age was associated with bilateral salpingo-oophorectomy. We detected a delayed induction of ovarian suppression therapy in a large proportion of women in both the medical ablation (13.6 months) and the bilateral salpingo-oophorectomy (22.9 months) treatment groups. Surgical complications were few, even with combined surgical procedures.
The landscape of adjuvant endocrine therapy in premenopausal women has changed significantly since the joint analysis of the SOFT and TEXT trials.7 These data had a median follow-up of 8 years, with findings suggesting an overall survival benefit of 1.8% for women receiving tamoxifen plus ovarian suppression versus tamoxifen alone (HR 0.59; 95% CI 0.42 to 0.84). This group was characterized by high-risk clinicopathological features and younger age (median 40 years). The absolute benefits of ovarian suppression were prominent in women who remained premenopausal after chemotherapy. Among those patients the rate of disease-free survival observed with tamoxifen plus ovarian suppression was 5.3% higher than tamoxifen alone and 9% higher with exemestane plus ovarian suppression. Our dataset presents similar distribution of high-risk features among women undergoing ovarian suppression. This may be related to the clinical conduct adopted by the specialists after the results of the SOFT and TEXT trial. Within the cohort undergoing ovarian ablation, the association of older age (OR 1.05) and bilateral salpingo-oophorectomy was significant. We hypothesize that women of older age are more inclined to consider surgical ovarian suppression.
In the combined analysis of TEXT and SOFT trials, the addition of ovarian suppression was associated with a substantial increase in grade 3 adverse events: 24.6% for tamoxifen versus 31.0% for tamoxifen plus ovarian suppression vs 32.3% for exemestane plus ovarian suppression. A similar increase was recorded for musculoskeletal symptoms (6.7% vs 5.7% vs 11.4%) and osteoporosis (3.9% vs 7.2 vs 14.8%), respectively. Vaginal dryness and dyspareunia were most frequent in the ovarian suppression plus exemestane group. Adverse events specifically for patients who opted for bilateral salpingo-oophorectomy or ovarian irradiation were not presented.
While optimal duration of ovarian suppression is not known, a postmenopausal state in young women comes with significant morbidity. In the Nurses’ Health Study, in the cohort undergoing hysterectomy between ages 35 and 50 without estrogen replacement therapy, the addition of bilateral salpingo-oophorectomy resulted in a significant increase in all-cause mortality.13 Long-term morbidity data are not available for medical ovarian suppression; however, it can be assumed that women treated with medical ovarian suppression and aromatase inhibitor would encounter long-term effects similar to those of premenopausal women undergoing bilateral salpingo-oophorectomy. Applying both the benefits of ovarian suppression for breast cancer prognosis and the resulting morbidity to a Markov Monte Carlo simulation model, Kwon and colleagues estimated 577 and 787 additional deaths in the medical ovarian suppression and bilateral salpingo-oophorectomy groups, respectively.14 When considering deaths from breast cancer and treatment-related adverse events, this model makes tamoxifen the optimal choice in endocrine therapy for premenopausal breast cancer; it is preferred for low-risk disease.
It is essential to identify candidates for ovarian suppression whose high risk of recurrence outweighs the risk of long-term morbidity. Regan and colleagues incorporated clinicopathological features in a continuous score termed ‘composite risk’.15 16 The absolute improvement of freedom from distant metastases for women with high composite risk was 10–15%. Although the composite risk score was not applied at our institution, women with high-risk features such as younger age, high tumor grade, stage III, or lymph node involvement were more likely to undergo medical ovarian suppression or bilateral salpingo-oophorectomy.
This retrospective study has limitations. As a single-institution study at a specialty center, the findings may reflect multidisciplinary care delivered by a relatively small number of clinicians; therefore, some findings may not be generalizable to other institutions. Menopausal status was extracted from physicians’ charts at initial consult, not by objective hormone level measurements; thus, we were unable to differentiate between premenopausal and perimenopausal status. It is unclear how many women were perimenopausal at the time of diagnosis, or how many transitioned into menopause after chemotherapy. For this reason, we analyzed the distribution of women older than 50 years between the four treatment groups. The distributions were even, ranging from 8.3% to 12.7% in each group (data not shown). Our observed rate of bilateral salpingo-oophorectomy versus medical ovarian suppression is higher than those cited in the SOFT and TEXT trials (16–18% of patients assigned to ovarian suppression opted to undergo bilateral oophorectomy or bilateral ovarian irradiation).7 In our cohort, the majority of women seeking bilateral salpingo-oophorectomy did so before initiating medical ovarian suppression. Many (n=193, 93%) began tamoxifen for a median duration of 18 months before crossing over to bilateral salpingo-oophorectomy. Women enrolled in the SOFT trial were offered a choice of medical ovarian suppression, bilateral salpingo-oophorectomy, or ovarian irradiation. Medical ovarian suppression was preferred (91%). In the TEXT trial, bilateral salpingo-oophorectomy or ovarian irradiation was allowed after 6 months of medical ovarian suppression. The rate of early cessation of medical ovarian suppression without substitution of ovarian ablation was 19% in the combined population of SOFT and TEXT. The prognostic impact of discontinuing medical ovarian suppression is unclear. In our study, only 53 women (22%) who had bilateral salpingo-oophorectomy started with medical ovarian suppression. The higher rate of bilateral salpingo-oophorectomy may be a result of the time period during which medical ovarian suppression for premenopausal women was not yet fully established. Another limitation is the lack of specific reasons cited for different forms of ovarian ablation; detailed information regarding the decision-making processes about bilateral salpingo-oophorectomy, or discussions about alternatives, were often not specified in physicians’ notes. Future research should examine whether adverse events associated with endocrine therapy, and/or quality of life concerns (ie, time commitment, mood disturbance) associated with medical ovarian suppression impact choice. There is a paucity of data regarding postoperative satisfaction or regret in women choosing bilateral salpingo-oophorectomy. This information would be crucial in guiding discussions between patients and providers regarding treatment options.
The only direct comparison of bilateral salpingo-oophorectomy versus treatment with luteinizing hormone-releasing hormone agonists was performed in women with metastatic disease. The authors show similar progression-free and overall survival in both groups.17 Bilateral salpingo-oophorectomy in the adjuvant setting was tested prior to that study and was shown to be equivalent to cyclophosphamide, methotrexate, and fluorouracil when combined with tamoxifen18; a second analysis 10 years later yielded similar results.19 The E-3193 study randomized 337 women to tamoxifen with and without ovarian suppression, with most choosing to undergo bilateral salpingo-oophorectomy (n=74; 42%). Neither quality of life nor complication rates differed between the groups.20 The adequacy of maintaining estrogen level suppression was examined in the SORT-EST substudy; at 3, 6, and 12 months, 34.2% of 79 treated with ovarian suppression and exemestane demonstrated at least one E2 level greater than 2.72 pg/mL.21 It is unclear whether these small transient increases of estradiol levels are also present, but less likely, in women undergoing bilateral salpingo-oophorectomy. In a recent study, Ferrandina and colleagues analyzed the cost-effectiveness of laparoscopic bilateral salpingo-oophorectomy and GnRHa administration in patients aged 40–49 years with hormone-sensitive breast cancer through a probabilistic decision tree model.22 The authors concluded that bilateral salpingo-oophorectomy is more cost-effective than GnRHa in the adjuvant setting.
Conclusion
Ovarian ablation is known to improve survival in premenopausal women with hormone receptor positive breast cancer with high-risk features. Therapeutic bilateral salpingo-oophorectomy is associated with low morbidity and is a reasonable alternative to medical ovarian suppression. However, many questions remain. Future prospective studies addressing the decision-making process, patients’ treatment preferences, and long-term effects of endocrine ablation are needed. Patient-reported outcomes, health-related quality of life, investigation of provider factors, treatment considerations and choice—including postoperative satisfaction or regret—will help guide future discussions between patients and providers, facilitating more informed decisions about treatment.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @VanceBroach, @leitaomd
Contributors AO: concept; design; data interpretation; drafting of manuscript; agrees to be responsible for all aspects of work. MLG: concept; data interpretation; supervision; drafting of manuscript; review of manuscript for important intellectual content; agrees to be responsible for all aspects of work. QCZ: data acquisition; drafting of manuscript; review of manuscript for important intellectual content; agrees to be responsible for all aspects of work. AI: data acquisition; data interpretation; review of manuscript for important intellectual content; agrees to be responsible for all aspects of work. RE: data acquisition; data interpretation; drafting of manuscript; agrees to be responsible for all aspects of work. ZA: data acquisition; data interpretation; drafting of manuscript; agrees to be responsible for all aspects of work. NF: data acquisition; data interpretation; drafting of manuscript; agrees to be responsible for all aspects of work. SBG: data interpretation; drafting of manuscript; review of manuscript for important intellectual content; agrees to be responsible for all aspects of work. KL: data interpretation; drafting of manuscript; review of manuscript for important intellectual content; agrees to be responsible for all aspects of work. YS: data interpretation; review of manuscript for important intellectual content; agrees to be responsible for all aspects of work. DJG: data interpretation; review of manuscript for important intellectual content; agrees to be responsible for all aspects of work. DSC: data interpretation; supervision; review of manuscript for important intellectual content; agrees to be responsible for all aspects of work. SSS: data acquisition; data interpretation; drafting of manuscript; agrees to be responsible for all aspects of work. VB: data interpretation; review of manuscript for important intellectual content; agrees to be responsible for all aspects of work. NRA-R: data interpretation; supervision; review of manuscript for important intellectual content; agrees to be responsible for all aspects of work. JC: data interpretation; review of manuscript for important intellectual content; agrees to be responsible for all aspects of work. ML: data interpretation; supervision; review of manuscript for important intellectual content; agrees to be responsible for all aspects of work. OZ: concept; design; data interpretation; supervision; drafting of manuscript; review of manuscript for important intellectual content; agrees to be responsible for all aspects of work.
Funding This study was funded in part through the NIH/NCI Support Grant P30 CA008748.
Disclaimer NAR reports grants from Stryker/Novadaq, grants from Olympus, grants from GRAIL, outside the submitted work. JC reports grants from Fidia grants from Sprout, outside the submitted work. DSC reports personal fees from Bovie Medical Co., personal fees from Verthermia Inc. (now Apyx Medical Corp.), personal fees from C Surgeries, personal fees from Biom 'Up, other from Intuitive Surgical Inc., other from TransEnterix Inc., outside the submitted work. AI reports personal fees from Mylan, outside the submitted work. MML is a consultant for Intuitive Surgical Inc., outside the submitted work. KLR reports other from Intuitive Surgical Inc., outside the submitted work.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.