Article Text

Abstract
Background The optimal treatment strategy for women with newly diagnosed ovarian cancer has yet to be determined. Poly(ADP-ribose) polymerase (PARP) inhibitors have demonstrated substantial improvement in progression-free survival as monotherapy maintenance treatment in the frontline setting versus active surveillance. Furthermore, preclinical and early clinical studies have shown that PARP inhibitors and immune checkpoint inhibitors have synergistic antitumor activity and may provide an additional therapeutic option for patients in this population.
Primary Objectives In women with newly diagnosed ovarian, fallopian tube, or peritoneal cancer, we wish to assess the efficacy of frontline maintenance treatment with the PARP inhibitor rucaparib versus placebo following response to platinum-based chemotherapy (ATHENA–MONO), and to assess the combination of rucaparib plus nivolumab (a programmed death receptor 1 (PD-1)–blocking monoclonal antibody) versus rucaparib alone (ATHENA–COMBO).
Study Hypothesis (1) Maintenance therapy with rucaparib monotherapy may extend progression-free survival following standard treatment for ovarian cancer in the frontline setting. (2) The combination of nivolumab plus rucaparib may extend progression-free survival following standard treatment for ovarian cancer in the frontline setting compared with rucaparib alone.
Trial Design ATHENA is an international, randomized, double-blind, phase III trial consisting of two independent comparisons (ATHENA–MONO and ATHENA–COMBO) in patients with newly diagnosed platinum-sensitive ovarian cancer. Patients are randomized 4:4:1:1 to the following: oral rucaparib+ intravenous nivolumab (arm A); oral rucaparib + intravenous placebo (arm B); oral placebo+ intravenous nivolumab (arm C); and oral placebo + intravenous placebo (arm D). The starting dose of rucaparib is 600 mg orally twice a day and nivolumab 480 mg intravenously every 4 weeks. ATHENA–MONO compares arm B with arm D to evaluate rucaparib monotherapy versus placebo, and ATHENA–COMBO evaluates arm A versus arm B to investigate the effects of rucaparib and nivolumab in combination versus rucaparib monotherapy. ATHENA–MONO and ATHENA–COMBO share a common treatment arm (arm B) but each comparison is independently powered.
Major Inclusion/Exclusion Criteria Patients ≥18 years of age with newly diagnosed advanced, high-grade epithelial ovarian, primary peritoneal, or fallopian tube cancer who have achieved a response after completion of cytoreductive surgery and initial platinum-based chemotherapy are enrolled. No other prior treatment for ovarian cancer, other than the frontline platinum regimen, is permitted.
Primary Endpoint The primary endpoint is investigator-assessed progression-free survival by Response Evaluation Criteria in Solid Tumors v1.1.
Sample Size Approximately 1000 patients have been enrolled and randomized.
Estimated Dates for Completing Accrual and Presenting Results The trial completed accrual in 2020. While dependent on event rates, primary results of ATHENA–MONO are anticipated in early 2022 and results of ATHENA–COMBO are anticipated to mature at a later date.
Trial Registration This trial is registered at clinicaltrials.gov (NCT03522246).
- ovarian neoplasms
- homologous recombination
- BRCA1 protein
- BRCA2 protein
Data availability statement
There are no data in this work.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, an indication of whether changes were made, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Ovarian cancer is the eighth leading cause of cancer-related death among women, responsible for approximately 184 000 deaths each year worldwide in 2018.1 For many decades, the standard of care for frontline therapy for women with newly diagnosed advanced ovarian cancer has consisted of a combination of cytoreductive surgery and platinum with or without taxane-based chemotherapy. Although most patients respond to this initial treatment, the majority will experience disease recurrence and require subsequent therapies.
The angiogenesis inhibitor, bevacizumab, has demonstrated significant improvement in progression-free survival in women with newly diagnosed ovarian cancer when added to frontline chemotherapy and continued as maintenance treatment.2 3 However, progression-free survival benefit with frontline bevacizumab use has not translated into an improvement in overall survival in this setting, and its use has been restricted to those with stage IV or high-risk disease in some countries.2 4 5 More recently, poly(ADP-ribose) polymerase (PARP) inhibitors, such as olaparib and niraparib, have provided promising therapeutic options as frontline maintenance treatment as monotherapy or, in the case of olaparib, in combination with bevacizumab, in patients with platinum-sensitive ovarian cancer; however, the greatest progression-free survival benefit has been seen, thus far, among patients with ovarian cancer associated with BRCA1 or BRCA2 (BRCA) gene mutations or homologous recombination deficiency.6 7 Despite these recent advances in frontline ovarian cancer therapies, the optimal treatment strategy for women with newly diagnosed ovarian cancer remains to be determined, given the varying level of efficacy achieved by PARP inhibitors in different molecular subgroups and the absence of a demonstrated overall survival benefit to date.
The PARP inhibitor, rucaparib, is approved in the United States and Europe as maintenance therapy for recurrent ovarian cancer that has responded to platinum-based chemotherapy, as well as for the treatment of BRCA-mutated ovarian cancer that has been treated with two or more prior chemotherapies.8 Given that rucaparib has demonstrated efficacy as maintenance therapy in the relapsed ovarian cancer setting regardless of BRCA mutation or homologous recombination deficiency status,9 we have hypothesized that the agent may also be effective as maintenance therapy across a broad patient population in the frontline setting.
Treatment with immune checkpoint inhibitors, such as nivolumab, a human programmed death receptor 1 (PD-1)–blocking monoclonal antibody, has led to markedly improved outcomes in multiple solid tumor types, such as non–small cell lung cancer and melanoma,10 but phase III studies evaluating immunotherapy in newly diagnosed ovarian cancer when added to conventional chemotherapy have not demonstrated any significant benefit to date.11 12 However, it is known that tumors with a deleterious BRCA mutation express novel, tumor-specific protein sequences (neoantigens), which can attract tumor-infiltrating lymphocytes that express programmed death-ligand 1 (PD-L1), and ovarian carcinomas associated with homologous recombination deficiency have more neoantigens relative to those that are homologous recombination proficient.13 Thus, ovarian tumors associated with BRCA mutations and/or homologous recombination deficiency may respond preferentially to immune checkpoint inhibitors, and the combination of a PARP inhibitor (ie, rucaparib) with an immune checkpoint inhibitor (ie, nivolumab) may have a synergistic effect.13 In addition, homologous recombination deficiency has recently been found to be associated with immune cell PD-L1 expression in newly diagnosed ovarian cancer.14
ATHENA–MONO and ATHENA–COMBO are two independent treatment comparisons to evaluate two separate hypotheses that were combined into one phase III trial to address patients’ unmet treatment needs. Both ATHENA–MONO and ATHENA–COMBO enrolled a broad, unselected patient population (eg, regardless of BRCA mutation or homologous recombination deficiency status) for the evaluation of these treatments as frontline maintenance. ATHENA–MONO aims to evaluate rucaparib monotherapy versus placebo to determine whether rucaparib monotherapy can extend progression-free survival in an unselected patient population. ATHENA–COMBO will evaluate whether adding nivolumab to rucaparib increases clinical benefit compared with rucaparib alone.
Methods
Trial Design
ATHENA (NCT03522246; GOG-3020/ENGOT-ov45) is an international, randomized, double-blind, phase III trial consisting of two separate and fully independently powered comparisons evaluating (1) rucaparib as monotherapy (ATHENA–MONO) and (2) rucaparib in combination with nivolumab (ATHENA–COMBO). The regimens are being assessed as maintenance treatment following response to frontline treatment (surgery and platinum-based chemotherapy) in patients with newly diagnosed ovarian cancer. Subjects are randomized 4:4:1:1 into the following arms: oral rucaparib + intravenous nivolumab (arm A); oral rucaparib + intravenous placebo (arm B); oral placebo + intravenous nivolumab (arm C); and oral placebo + intravenous placebo (arm D).
In ATHENA–MONO, rucaparib (arm B) is compared with placebo (arm D) to assess the effects of rucaparib monotherapy as frontline maintenance therapy. The treatment phase consists of 28-day treatment cycles. A starting dose of rucaparib 600 mg or placebo is administered orally twice a day. In ATHENA–COMBO, rucaparib and nivolumab (arm A) is compared with rucaparib (arm B), to evaluate the effects of adding nivolumab to rucaparib monotherapy. Oral rucaparib or placebo is administered prior to the initiation of the intravenous nivolumab or placebo. Rucaparib 600 mg is administered twice a day for the first 28-day cycle (cycle 1) and continued thereafter (arm B). Dosing with the intravenous study drug (nivolumab 480 mg) begins on cycle 2, day 1, and is administered every 4 weeks (arm A). Study drug treatment continues in 28-day cycles until 24 months after initiation of oral/intravenous combination study treatment, disease progression, death, or unacceptable toxicity.
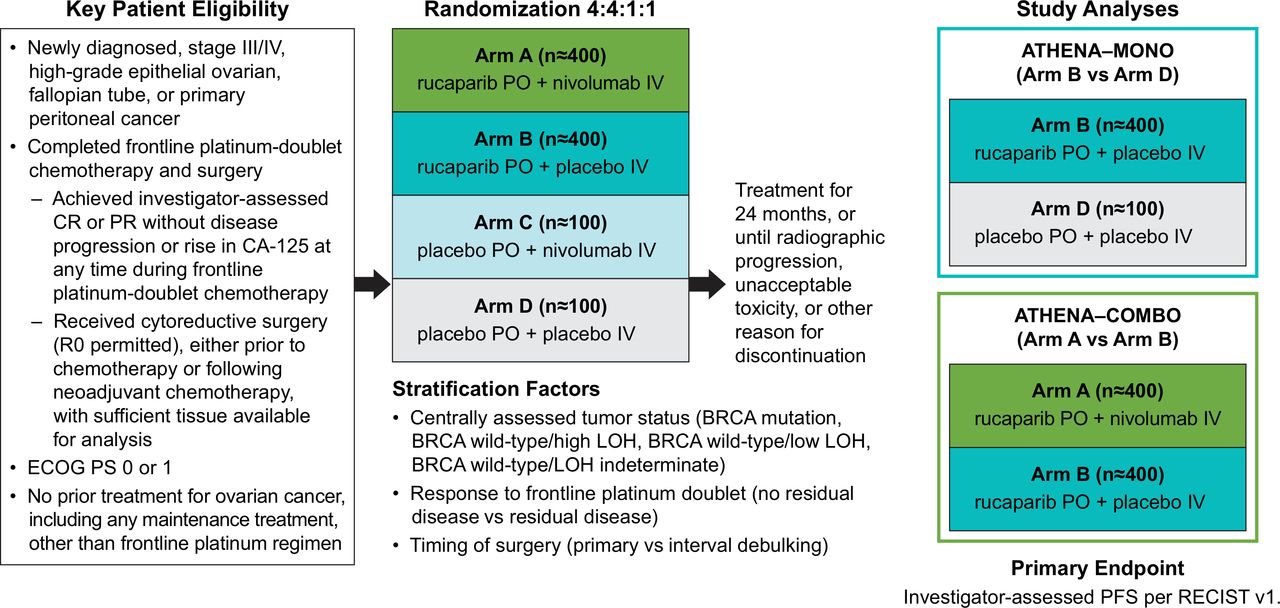
Figure 1 shows the trial schema and analysis plan for ATHENA–MONO and ATHENA–COMBO. In addition, as an exploratory endpoint, arm C (nivolumab) will be analyzed against arm D (placebo) to assess the relative contribution of nivolumab alone.

{kind=link}
Study schema and analysis plan. Starting dose of rucaparib is 600 mg orally twice a day and nivolumab 480 mg intravenously every 4 weeks. BRCA, BRCA1 or BRCA2; CA-125, cancer antigen 125; CR, complete response; ECOG PS, Eastern Cooperative Oncology Group performance status; IV, intravenous; LOH, loss of heterozygosity; PO, by mouth; PR, partial response; R0, total cytoreduction; RECIST, Response Evaluation Criteria in Solid Tumors.
Submission of tumor tissue from the cytoreductive surgery is required prior to enrollment to perform next-generation sequencing–based testing (FoundationOne CDx) by Foundation Medicine (Cambridge, Massachusetts, USA). The next-generation sequencing–based test determines the mutation status of homologous recombination pathway genes, including BRCA, and the percentage of the genome with loss of heterozygosity.9 In addition, biomarkers related to response or resistance to immunotherapies are being assessed.
The trial is being led by the GOG Foundation (GOG protocol 3020) and is conducted in association with NRG Oncology–Japan and the European Network of Gynecological Oncological Trial Groups (ENGOT protocol ov45). Target enrollment of approximately 1000 patients has been completed across 24 countries in North America, Europe, Asia, and Australia/New Zealand. The trial is approved by the institutional review board at each study site and done in accordance with the Declaration of Helsinki and Good Clinical Practice Guidelines of the International Council for Harmonisation. Patients provided written informed consent before participation.
Participants
Eligible patients are at least 18 years of age with newly diagnosed histologically confirmed, advanced (International Federation of Gynecology and Obstetrics stages III–IV), high-grade epithelial ovarian, primary peritoneal, or fallopian tube cancer. Patients must have completed frontline platinum-doublet chemotherapy and cytoreductive surgery, and achieved a response, as assessed by the investigator (defined as having no evidence of measurable disease by Response Evaluation Criteria in Solid Tumors (RECIST) v1.1 in patients with a complete resection (R0) following cytoreductive surgery or a complete response or partial response by RECIST v1.1, or a cancer antigen (CA-125) response by Gynecologic Cancer Intergroup criteria in patients with non-measurable disease), with no evidence of disease progression radiologically or through rising CA-125 at any time during frontline treatment. Cytoreductive surgery could have been completed prior to chemotherapy or following neoadjuvant chemotherapy. Patients must have received 4–8 cycles of frontline platinum-doublet treatment per standard clinical practice, including a minimum of 4 cycles of a platinum/taxane combination and at least 6 cycles of chemotherapy if best response was a partial response; no other prior treatment for ovarian cancer, including maintenance treatment, is permitted. Patients must have an Eastern Cooperative Oncology Group performance status of 0 or 1 and have adequate organ function.
Randomization and Blinding
Randomization is performed using a central randomization procedure with an interactive response technology. Patients are stratified at study entry to ensure treatment groups are balanced based on disease status after chemotherapy (residual disease vs no residual disease); timing of surgery (primary surgery vs interval debulking); and homologous recombination deficiency classification (BRCA mutation, BRCA wild-type/high loss of heterozygosity (loss of heterozygosity ≥16%), BRCA wild-type/low loss of heterozygosity (loss of heterozygosity <16%), BRCA wild-type/loss of heterozygosity indeterminate) by central laboratory next-generation sequencing–based test.
Rucaparib and nivolumab treatments are double blinded, so that the investigators, clinical site staff, patients, and sponsor personnel are blinded to all study treatment. Active and placebo oral and intravenous solutions are identical in appearance and supplied in identical containers. Clinical trial progress, safety, and efficacy event rates are being monitored by an independent data monitoring committee.
Outcomes
For both ATHENA–MONO and ATHENA–COMBO, the primary objectives are evaluation of investigator-assessed progression-free survival per RECIST v1.1. Secondary objectives include evaluation of progression-free survival, as assessed by blinded independent central review, overall survival, investigator-assessed objective response rate per RECIST v1.1, duration of response, and safety. Key exploratory objectives are to evaluate progression-free survival on the subsequent line of treatment, contribution of nivolumab monotherapy to efficacy of the combination, evaluation of potential molecular markers of response or resistance (eg, mutations in non-BRCA homologous recombination repair genes, PD-L1 expression, and tumor mutational burden, or genetic variants observed in circulating tumor DNA), and health-related quality of life and patient reported outcomes.
Sample Size and Statistical Methods
The ATHENA–MONO and ATHENA–COMBO comparisons will each separately evaluate primary and key secondary endpoints. The level of statistical significance will be split into two so that the ATHENA–MONO and ATHENA–COMBO comparisons will be made independently at a one-sided 0.0125 significance level. In order to yield ≥90% power at a one-sided 0.0125 significance level to show a statistically significant difference in progression-free survival, a sample size of at least 500 patients is required for ATHENA–MONO and at least 800 patients for ATHENA–COMBO.
Kaplan–Meier methodology will be used to summarize time-to-event variables. The 50th (median) percentile with 95% confidence interval will be summarized for each randomized treatment group. The stratified hazard ratio from the Cox proportional hazards model will be used to estimate the hazard ratio between the randomized treatment groups.
Discussion
Despite recent advances in the therapeutic landscape of newly diagnosed ovarian cancer, advanced ovarian cancer is still considered an incurable disease for the majority of patients. Thus, early and effective treatment options to further improve progression-free survival and overall survival are needed. Results from the SOLO1 and PRIMA phase III studies led to regulatory approvals of the PARP inhibitors, olaparib and niraparib, in the frontline maintenance setting following primary surgery and response to platinum-based chemotherapy.6 15 However, there are outstanding questions on appropriate patient selection based on clinical or molecular characteristics. In SOLO1, enrollment was restricted to women with newly diagnosed germline or somatic BRCA-mutated ovarian cancer. Although the PRIMA trial had no restriction on BRCA mutation or homologous recombination deficiency status, the greatest improvement in progression-free survival with niraparib treatment was observed in the BRCA-mutated and homologous recombination deficiency–positive subgroups. While a statistically significant progression-free survival improvement was reported in the homologous recombination deficiency–negative subgroup (hazard ratio 0.68, 95% confidence interval 0.49 to 0.94), the median progression-free survival was relatively short in the niraparib and placebo arms (8.1 vs 5.4 months, respectively). Additionally, PRIMA enrolled patients with clinically high-risk features for recurrence and excluded patients with complete resection/R0 after primary debulking surgery; thus, unanswered questions remain regarding the use of PARP inhibitors for maintenance treatment for a large proportion of newly diagnosed ovarian cancer patients in real-world clinical practice.
The primary aim of ATHENA–MONO is to determine whether rucaparib monotherapy as frontline maintenance treatment can extend progression-free survival in an unselected patient population. The study is enrolling patients regardless of BRCA mutation or homologous recombination deficiency status, and patients with complete resection/R0 after primary debulking surgery are allowed. In addition to evaluation in the overall, unselected population, analyses will also be conducted to evaluate efficacy in patients based on homologous recombination deficiency status. Positive results from ATHENA–MONO will demonstrate the effectiveness of rucaparib monotherapy in the frontline maintenance setting and broaden our understanding of the patient population that may benefit from a PARP inhibitor.
Although prior results from immunotherapy studies in newly diagnosed ovarian cancer have yielded disappointing efficacy benefits, the data suggest again that certain disease or molecular characteristics may be associated with improved efficacy in this setting.11 12 The ATHENA–COMBO comparison has been designed to evaluate the magnitude of benefit for adding nivolumab to rucaparib monotherapy in a frontline maintenance setting. Biomarkers that may be associated with higher immunogenicity (eg, PD-L1 expression, homologous recombination deficiency status) will also be assessed as exploratory analyses. The combination of rucaparib and nivolumab could provide additional therapeutic options to further extend progression-free survival. To our knowledge, ATHENA–COMBO is the first study to evaluate the combination of a PARP inhibitor and an immune checkpoint inhibitor as switch maintenance treatment (and not continuation maintenance) following completion and response to frontline chemotherapy. In addition, the dosing sequence of starting rucaparib one cycle prior to nivolumab in the study not only provides the opportunity to establish a baseline safety profile of the oral study drug for each patient prior to administering the intravenous study drug, but it also tests the hypothesis that priming the immune system with rucaparib monotherapy will enhance the activity in combination with nivolumab. The inclusion of a nivolumab monotherapy arm (arm C) will also allow us to better understand the relative contributions of each agent to the rucaparib + nivolumab combination.
Translational studies in the ATHENA trial will further our understanding of the changes in the tumor microenvironment following treatment with a PARP inhibitor, immunotherapy, or the combination. Patients are required to have sufficient tumor tissues from their cytoreductive surgery prior to enrollment, and blood samples will be collected during the study for circulating tumor DNA and immunogenicity analyses. The existing data from ovarian cancer trials do not provide a clear picture of an appropriate biomarker for patient selection for therapy. The study plans to assess biomarkers (eg, homologous recombination repair genes, PD-L1 expression, and tumor mutational burden) that may provide further insights into optimal patient selection for maintenance treatment, the factors that influence the activity of rucaparib alone and in combination with nivolumab, and potential resistance mechanisms.
The overall design of the ATHENA study is unique in that the treatment comparisons (ATHENA–MONO and ATHENA–COMBO) share arm B (rucaparib monotherapy). This innovative design optimizes use of our most valuable resource: our patients. Independent analyses for ATHENA–MONO and ATHENA–COMBO will be unblinded to treatment allocations and read out at different time points during the trial. Primary results for ATHENA–MONO are anticipated in early 2022, and results from ATHENA–COMBO are anticipated to mature at a later date.
Data availability statement
There are no data in this work.
Ethics statements
Patient consent for publication
Ethics approval
The trial is approved by the institutional review board at each study site and done in accordance with the Declaration of Helsinki and Good Clinical Practice Guidelines of the International Council for Harmonization.
Acknowledgments
The ATHENA study is being conducted as part of a clinical collaboration with Bristol-Myers Squibb. Medical writing support was provided by Vivian Chen (Clovis Oncology Inc, Boulder, Colorado, USA), and editorial support funded by Clovis Oncology was provided by Stephen Bublitz (Ashfield MedComms, an Ashfield Health Company).
Footnotes
Twitter @Shannon.Westin
Contributors All authors have read, reviewed, and approved the manuscript.
Funding The study was funded by Clovis Oncology Inc.
Competing interests BJM has served as a consultant and received honoraria from Clovis Oncology, Aravive, AstraZeneca, Easai, Elevar, Genetics, Genmab/Seattle, GOG Foundation, Gradalis, ImmunoGen, Karyopharm, McKesson, Merck, Mersana, Myriad, Novocure, Pfizer, Roche/Genentech, Sorrento, Tesaro/GSK, and VBL outside the submitted work. RLC reports grants from Clovis Oncology, AstraZeneca, Genmab, Janssen, Merck, and Roche/Genentech; and has served as a consultant for Clovis Oncology, Agenus, AstraZeneca, Genmab, GSK, Janssen, OncoQuest, Roche/Genentech, and Regeneron outside the submitted work. KF has received institutional funding from Clovis Oncology during the conduct of the study; and received traveling support from Clovis Oncology outside the submitted work. AMO has received an institutional grant from AstraZeneca; served on data safety monitoring boards or advisory boards (uncompensated) for AstraZeneca and GSK; served on steering committees (uncompensated) for Clovis Oncology and AstraZeneca; and served as a principal investigator on investigator-initiated trials for Clovis Oncology, AstraZeneca, and GSK. DMO has served as a consultant for Clovis Oncology, Abbvie, Agenus, Ambry, Amgen, Arquer Diagnostics, AstraZeneca, Eisai, Elevar, Genentech/Roche, GOG Foundation, Immunogen, InxMed, Iovance Biotherapeutics, Janssen/J&J, Merck, Mersana, Myriad Genetics, Novartis, Novocure, Regeneron, Roche Diagnostics MSA, Rubis, SDP Oncology (BBI), SeaGen, Sorrento, Takeda, Tarveda, Tesaro/GSK, and Toray; and has received research support from Clovis Oncology, Abbvie, Agenus, Ajinomoto, Amgen, Array Biopharma, AstraZeneca, Bristol-Myers Squibb, Cerulean Pharma, Eisai, EMD Serono, Ergomed, Genentech/Roche, GenMab, GOG Foundation, Immunogen, INC Research, inVentiv Health Clinical, Iovance Biotherapeutics, Janssen/J&J, Ludwig Cancer Research, Merck, Mersana, New Mexico Cancer Care Alliance, Novocure, PRA International, Regeneron, SDP Oncology (BBI), SeaGen, Serono, Stemcentrx, Tesaro/GSK, TRACON Pharmaceuticals, VentiRx, and Yale University outside the submitted work. DL has received institutional funding for trial development from Clovis Oncology during the conduct of the study; and has received research grants from Clovis Oncology; served on advisory boards for Clovis Oncology, AstraZeneca, GSK, Merck Sharp & Dohme, and PharmaMar outside the submitted work. SNW has received institutional funding and served as a consultant for Clovis Oncology during the conduct of the study; received institutional funding from Clovis Oncology, AstraZeneca, Bayer, Bio-Path, Cotinga Pharmaceuticals, GSK/Tesaro, Mereo, NIH, Novartis, and Roche/Genentech; served as a consultant for Clovis Oncology, Agenus, AstraZeneca, Eisai, GSK/Tesaro, Merck, Novartis, Pfizer, Roche/Genentech, and Zentalis; and is involved in an unpaid leadership or fiduciary role for GOG Foundation Board of Directors, Houston Gynecology and Obstetrical Society, NOCC – National Ovarian Cancer Coalition Advisory Board, OVARCOME Leadership Council, and Society of Gynecologic Oncology Board of Directors outside the submitted work. TJH has served on advisory boards for Clovis Oncology, Aravive, AstraZeneca, Caris, Elsai, GSK, Johnson & Johnson, Merck, and Roche Genentech; and has served as a consultant for Abbvie outside the submitted work. FM reports personal fees from Amgen, AstraZeneca, Celegene, CureVac, Eisai, GenomicHealth, Gilead/Immunomedics, GSK, Janssen-Cilag, MSD, Myriad, Novartis, Pfizer, Pierre-Fabre, PharmaMar, Roche, Tesaro, and Seagen outside the submitted work. RNE has served as a consultant for Clovis Oncology, AstraZeneca, Daiich Sankyo, Eisai, GSK, Merck, and Seagen; and received honoraria from AstraZeneca and Myriad outside the submitted work. IAM has served on advisory boards for Clovis Oncology, AstraZeneca, Roche, Takeda, and Tesaro; and received institutional funding from AstraZeneca outside the submitted work. RSK has served on data safety monitoring boards or advisory boards for Clovis Oncology, Basilea, Eisai, GSK, iTeos Therapeutics, Roche, Sotio, and Tesaro; and is involved in a leadership or fiduciary role for MHRA OHEAG. KKL, DS, SG, NG, SH, and LM are employees of Clovis Oncology and may own stock or have stock options in that company. All authors received writing support from Clovis Oncology during the conduct of the study.
Provenance and peer review Commissioned; internally peer reviewed.