Article Text

Abstract
Background Quality of surgical care as a crucial component of a comprehensive multi-disciplinary management improves outcomes in patients with endometrial carcinoma, notably helping to avoid suboptimal surgical treatment. Quality indicators (QIs) enable healthcare professionals to measure their clinical management with regard to ideal standards of care.
Objective In order to complete its set of QIs for the surgical management of gynecological cancers, the European Society of Gynaecological Oncology (ESGO) initiated the development of QIs for the surgical treatment of endometrial carcinoma.
Methods QIs were based on scientific evidence and/or expert consensus. The development process included a systematic literature search for the identification of potential QIs and documentation of the scientific evidence, two consensus meetings of a group of international experts, an internal validation process, and external review by a large international panel of clinicians and patient representatives. QIs were defined using a structured format comprising metrics specifications, and targets. A scoring system was then developed to ensure applicability and feasibility of a future ESGO accreditation process based on these QIs for endometrial carcinoma surgery and support any institutional or governmental quality assurance programs.
Results Twenty-nine structural, process and outcome indicators were defined. QIs 1–5 are general indicators related to center case load, training, experience of the surgeon, structured multi-disciplinarity of the team and active participation in clinical research. QIs 6 and 7 are related to the adequate pre-operative investigations. QIs 8-22 are related to peri-operative standards of care. QI 23 is related to molecular markers for endometrial carcinoma diagnosis and as determinants for treatment decisions. QI 24 addresses the compliance of management of patients after primary surgical treatment with the standards of care. QIs 25–29 highlight the need for a systematic assessment of surgical morbidity and oncologic outcome as well as standardized and comprehensive documentation of surgical and pathological elements. Each QI was associated with a score. An assessment form including a scoring system was built as basis for ESGO accreditation of centers for endometrial cancer surgery.
- endometrial neoplasms
- surgical oncology
Statistics from Altmetric.com
INTRODUCTION
Optimizing and ensuring the quality of surgical care is essential to improve the management and outcome of patients with endometrial carcinoma. The quality of surgical care as a component of comprehensive multi-disciplinary management has been shown to improve outcomes in patients with endometrial carcinoma, notably helping to avoid suboptimal surgical treatment.1 Adoption of guidelines is an effective tool for disease control and should be considered as a process measure of quality of gynecological cancer care.2 QIs enable healthcare professionals to compare their clinical management with the ideal standards according to the guidelines in order to detect aspects of suboptimal care.3 In order to complete its set of QIs for the surgical management of gynecological cancers, the European Society of Gynaecological Oncology (ESGO) initiated a project aiming to develop a list of QIs for surgical treatment of endometrial carcinoma.
The idea behind the project is to improve the standard of surgical care by providing a set of quality criteria that can be used on many levels: self-assessment, institutional quality assurance programs, governmental quality assessment, and eventually, to build a network of certified centers for endometrial carcinoma surgery. Certified centers can make the award known to doctors, patients, patient advocacy groups, and lay persons. The intention is incentive, not punitive. The targets defined by the international development group should not be used to penalize or litigate doctors or institutions. These QIs will be updated and modified based on new evidence.
METHODS
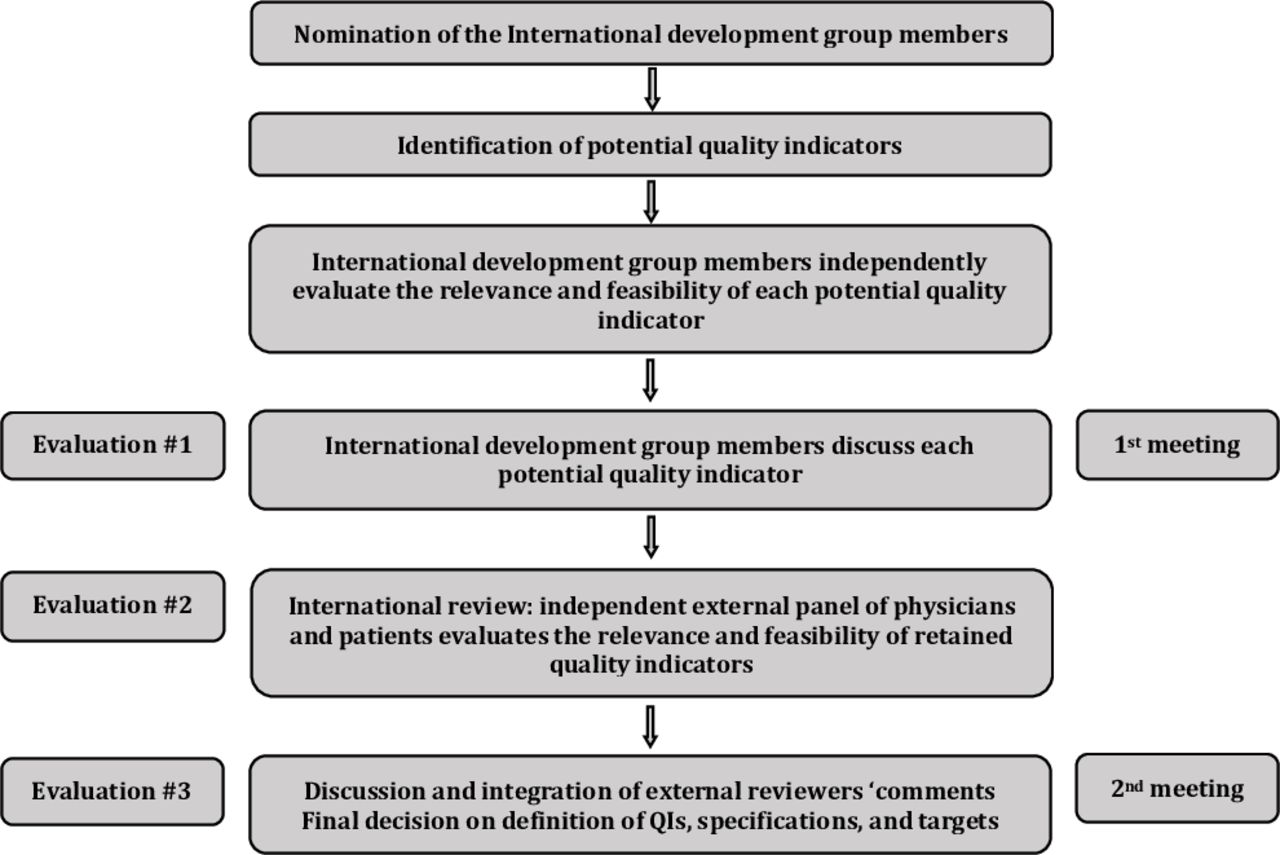
QIs for the surgical treatment of endometrial carcinoma were developed using a three-step evaluation process (Figure 1). This development process involved two meetings of an international development group, chaired by Professor Nicole Concin (Medical University of Innsbruck, Innsbruck, Austria/Evangelische Kliniken Essen-Mitte, Essen, Germany) and Professor Jan Persson (Skåne University Hospital, Lund University, Faculty of Medicine, Clinical Sciences, Lund, Sweden).
{kind=link}
Development process.
Nomination of an International Development Group
The ESGO Council nominated 17 gynecologic oncologists from its membership body, with well-recognized expertize, clinical and research activity, and leadership in the field as surrogate markers for their continuous effort in improving patients care.
Identification of Potential QIs
All potential QIs for endometrial carcinoma surgery were defined from the guidelines jointly developed by ESGO, the European SocieTy for Radiotherapy and Oncology (ESTRO), and the European Society of Pathology (ESP), and published indicators identified using a systematic literature search in Medline without any restriction of the search period (indexing terms: QI, quality assurance, endometrial carcinoma, endometrial cancer, uterine neoplasms, surgery, methodology, consensus statements, evidence-based medicine).4–11 Another systematic literature search was then conducted in Medline to identify available scientific evidence which supports the potential QIs (Online supplemental appendix 1). The reference list of each identified article was reviewed for other potentially relevant papers. The development group members were allowed to provide any additional references they deemed relevant (if any).
Supplemental material
Evaluation of Potential QIs
Potential QIs were formatted as a questionnaire and sent to the international development group. Experts were asked to evaluate each indicator according to relevance and feasibility in clinical practice. They were also free to propose any additional possible QIs they deemed relevant. Acceptance, rejection, or the need for further consideration of each indicator was discussed during the first meeting (February 3–4, 2021). QIs were retained if a large consensus among experts was reached.
External Evaluation of the Retained QIs: International Review
The ESGO Council established a large panel of practicing clinicians who provide care to patients with endometrial carcinoma. These international reviewers are independent of the international development group and are from different European and non-European countries to ensure global perspective. Patients with endometrial carcinoma were also included. The retained indicators were formatted as a questionnaire and sent to the reviewers for quantitative evaluation of each indicator according to relevance, feasibility in clinical practice, and quality of care improvement (physicians only). Open comments were encouraged (qualitative evaluation). Patients were asked to qualitatively evaluate each QI (according to their experience, preferences, feelings, etc). Evaluations of the indicators were returned by 140 independent physicians and by three patients with endometrial carcinoma (the list of international reviewers is available in Online supplemental appendix 2). Responses were pooled and sent to experts who convened during the second meeting (May 26–27, 2021). The comments were reviewed and discussed by the international development group members. Definitions of QIs, specifications, and targets were validated during the second meeting. Although the strengths of the process include an international development group, an international expert consensus to support the QIs, an international external review process (physicians and patients), a structured format to present the QIs, and management of potential conflicts of interests, the QIs result from a consensus of experts, with inherent bias in this type of method. They may have to be modified in the future based on publication of new data.
RESULTS
The key characteristics of an ideal indicator are clear definition, clinical relevance, measurability, and feasibility in clinical practice. Each retained QI is categorized as a structural indicator, process indicator, or outcome indicator and has a description which specifies what the indicator is measuring.12 The measurability specifications are then detailed. The latter highlight the way in which the indicator will be measured in practice to allow audits. The time frame for assessment of criteria is the last calendar year (unless otherwise indicated). Further to measurement of the indicator, a target is indicated. This specifies the level which each unit/center should be aiming to achieve. When appropriate, two targets were defined: an optimal target, expressing the best possible option for patients and a minimal target, expressing the minimal requirement when practical feasibility factors are taken into account. Targets are based on available scientific evidence, personal experience of the international development group members, on expert consensus, and on feedbacks from external reviewers. QIs 1–5 are general indicators related to center case load, training, experience of the surgeon, structured multi-disciplinarity of the team, and active participation in clinical research (Table 1). QIs 6 and 7 are related to the adequate pre-operative investigations (Table 2). QIs 8–22 are related to the compliance of the peri-operative management with the standards of care (Table 3). QI 23 is related to molecular markers for endometrial carcinoma diagnosis and as determinants for treatment decisions (Table 4). QI 24 addresses the compliance of management of patients after primary surgical treatment with the standards of care (Table 5). QIs 25–29 highlight the need for a systematic assessment of surgical morbidity and oncologic outcomes as well as standardized and comprehensive documentation of surgical and pathological elements (Table 6).
General indicators
Adequate pre-operative investigations
Compliance of the peri-operative management with the standards of care
QI related to molecular markers for endometrial carcinoma diagnosis and as determinants for treatment decisions
Compliance of management of patients after primary surgical treatment with the Standards of care
Recording pertinent information
General Indicators
Although the number of cases treated per center per surgeon per year is not a sufficient guarantee of surgical quality, it is major prerequisite. The volume effect on outcomes of cancer operation is related to a surgeon’s skill and experience defined notably by surgical volumes, as well as hospital infrastructure and the supporting team dedicated to surgical care. Available data support a positive relationship between number of cases operated on and outcomes (eg, survival, increased technical expertize, adherence to evidence-based treatment recommendations, and appropriate management of complications) for different types of cancer, indicating a benefit for centralization of care pathways.13–112 Volume appears to have more effects on outcomes for high-risk procedures that are associated with substantial morbidity. In a large National Cancer Database in the United States including 441 863 patients with uterine cancer patients, survival was significantly increased with increasing hospital volume for women with all stages of endometrioid, clear cell, serous, or carcinosarcoma endometrial cancer (25, 50, or 100 cases per year).88
Wright et al explored the association between changes over time (from 2000 to 2014) in volume and peri-operative outcomes for 44 558 women undergoing hysterectomy for endometrial cancer at 218 hospitals and showed that increased hospital volume was associated with lower rates of surgical and medical complications, mortality, transfusion, and prolonged length of stay.109 Diaz-Montes et al aimed to characterize the short-term outcomes for uterine cancer according to hospital case volume (6181 women undergoing primary surgery by 894 surgeons at 49 hospitals).34 Although there was a trend toward a lower in-hospital death rate for women managed at high-volume hospitals compared with low-volume hospitals, this trend did not reach statistical significance. Dividing volume hospitals depending on the average annual number of surgeries for endometrial carcinoma (using relatively low case number cut-off points: low <15 /year, medium 15–24/year, and high ≥25 /year), Becker et al observed no relation between surgical volumes and relative survival of patients with endometrial cancer.18
In Europe, the organization of gynecologic oncology training differs among countries, but there is a trend towards centralization and subspecialization. ESGO has developed a subspecialty training program in gynecologic oncology. Increasing evidence shows that the subspecialty backgrounds of treating physicians affect treatment outcomes of patients with malignant disease.113–120 Chan et al explored this hypothesis specifically for patients with endometrial carcinoma.121 Treatment by gynecologic oncologists was n independent prognostic factor for improved disease-specific survival after adjusting for age, stage, and grade of disease. According to the ESGO/ESTRO/ESP guidelines, treatment should be undertaken in a specialized center by a dedicated team of specialists in the diagnosis and management of gynecological cancers, especially in high-risk and/or advanced-stage disease.4–6
Multi-disciplinary care is recognized as best practice in treatment planning and care for patients internationally. In several cancer types, there is evidence that decisions made by a multi-disciplinary team are more likely to be in accord with evidence-based guidelines than those made by individual clinicians, and the role of a multi-disciplinary approach in the quality of care is recognized.119 122–129 According to the ESGO/ESTRO/ESP guidelines, planning of staging and treatment should be made on a multi-disciplinary basis (generally at a tumor board meeting, composed according to local guidelines) and based on the comprehensive and precise knowledge of prognostic and predictive factors for outcome, morbidity, and quality of life.4–6
Treatment requires centralization and involvement of a broad multi-disciplinary team including at least a certified gynecologic oncologist (or in countries where certification is not organized, a trained surgeon dedicated to the management of gynecological cancer (accounting for more than 80% of his or her practice or having completed an ESGO-accredited fellowship)), a radiologist, a radiation oncologist, a physician certified to deliver chemotherapy (a gynecologic oncologist and/or a physician with special interest to gynecologic oncology (medical or clinical oncologist)), and a pathologist. A structured program for multi-disciplinary diagnostic work-up, treatment, and follow-up must be present in centers responsible for the treatment. Institutions participating in clinical research can contribute to improvement of quality of care.130–159 Patients treated in study hospitals have a higher chance of receiving standard treatment according to guidelines than patients treated in hospitals not participating in cooperative clinical studies. Study hospitals might participate more often in quality assurance programs.
Adequate Pre-operative Investigations
Recording of histopathological tumor type and grade is required in endometrial biopsies. According to the ESGO/ESTRO/ESP guidelines, the mandatory pre-operative work-up includes: family history; general assessment and inventory of co-morbidities; geriatric assessment, if appropriate; clinical examination, including pelvic examination; expert vaginal or transrectal ultrasound or pelvic MRI.4–6 Depending on clinical and pathologic risk, additional imaging modalities (thoracic, abdominal and pelvic CT scan, MRI, positron emission tomography scan, or ultrasound) should be considered to assess ovarian nodal, peritoneal, and other sites of metastatic disease.
Multiple studies have reported high specificity of MRI techniques in the assessment of deep myometrial invasion, cervical stromal involvement, and lymph node metastasis.160–207 Similarly, high diagnostic performance of transvaginal ultrasound for the assessment of deep myometrial and cervical stromal invasions has also been described.164 169 181 208–213 In centers routinely performing a sentinel lymph node procedure in all patients with endometrial carcinoma, the need for pre-operative risk grouping based on myometrial invasion estimates is less pronounced.
Compliance of the Peri-operative Management with the Standards of Care
Many studies including two randomized prospective studies and pooled analyses support the use of minimally invasive surgery for patients with early-stage endometrial carcinoma, including those with high-risk carcinomas.214–281 Patients with high body mass index benefit from a minimally invasive approach most.282 According to the ESGO/ESTRO/ESP guidelines, minimally invasive surgery is the preferred surgical approach, including patients with high-risk endometrial carcinoma, in stage I and II disease.4–6 Any intra-peritoneal tumor spillage, including tumor rupture or morcellation (including in a bag), should be avoided. If vaginal extraction risks uterine rupture, other measures should be taken (eg, mini-laparotomy, use of endobag). Tumors with metastases outside the uterus and cervix (excluding lymph node metastases) are relative contraindications for minimally invasive surgery. Staging infracolic omentectomy should be performed in clinical stage I serous endometrial carcinoma, carcinosarcoma, and undifferentiated carcinoma, due to the high risk of microscopic omental metastases.283 The low rate of omental metastases in apparent clinical stage I endometrioid and clear cell carcinoma does not justify the procedure.284–298
A large amount of evidence supports the importance of sentinel lymph node biopsy in the surgical staging of patients with early-stage endometrial carcinoma and in the decision process on adjuvant therapies.299–361 Applying a sentinel lymph node algorithm in high-risk/high-grade endometrial carcinomas in the hands of experienced surgeons appears accurate to detect pelvic lymph node metastases.301 302 357 362 The use of indocyanine green increases sentinel lymph node detection rates per hemipelvis as compared with methylene blue dye in women with endometrial carcinoma undergoing minimally invasive surgery.363 364 High bilateral pelvic sentinel lymph node detection can be achieved when the tracer is injected into the cervix.300 365 Ultrastaging and pathologic review of negative pelvic lymph nodes of patients with presumed isolated para-aortic metastasis can identify occult pelvic dissemination.334 352 According to the ESGO/ESTRO/ESP guidelines, sentinel lymph node biopsy can be considered for staging purposes in patients with low-risk/intermediate-risk disease.4–6 Surgical lymph node staging should be performed in patients with high-intermediate-risk/high-risk disease. Sentinel lymph node biopsy is an acceptable alternative to systematic lymphadenectomy for lymph node staging in stage I–II. If sentinel lymph node biopsy is performed:
Indocyanine green with cervical injection is the preferred detection technique.
Tracer re-injection is an option if sentinel lymph node is not visualized upfront.
Side-specific systematic lymphadenectomy should be performed in high-intermediate-risk/high-risk patients if sentinel lymph node is not detected on either pelvic side.
Pathologic ultrastaging of sentinel lymph nodes is recommended.
A meta-analysis published in the beginning of the 2010s has quantified the association of complete cytoreduction with a statistically significant improvement in survival in patients with advanced/metastatic endometrial cancer.366 More recently, several retrospective studies have confirmed the prognostic importance of complete cytoreductive surgery.367–370 According to the ESGO/ESTRO/ESP guidelines, surgical tumor debulking including enlarged lymph nodes should be considered in stage III and IV endometrial carcinoma (including carcinosarcoma) when complete macroscopic resection is feasible with an acceptable morbidity and quality of life profile.4–6
Treatment of patients with recurrent endometrial carcinoma involves a multi-disciplinary approach with surgery, radiotherapy, and/or systemic therapy depending on the fitness and wishes of the patient, the tumor dissemination patterns, and prior treatment. In radiotherapy naïve patients, a decision about surgery needs to take account of patient morbidity and wishes, available non-surgical treatments, and resources. The interval between primary treatment and recurrences should also be taken into consideration. According to the ESGO/ESTRO/ESP guidelines, radiotherapy naïve patients with recurrent disease (including peritoneal and lymph node relapse) should be considered for surgery only if it is anticipated that complete removal of macroscopic disease can be achieved with acceptable morbidity.4–6 In radiotherapy pre-treated patients (external beam radiotherapy ± brachytherapy) with loco-regional recurrence, radical surgery, including exenteration, should be considered when the intention is complete resection with clear margins. Patients with oligometastatic disease should be considered for radical local therapy, including surgery, radiation therapy, and local ablating techniques.
Molecular Classification and Adjuvant Treatment
Four molecular subgroups of endometrial carcinoma and their determination by surrogate maker analyses have undergone extensive studies in recent years (POLE mutated, mismatch repair-deficient, p53 abnormal and endometrial carcinoma lacking any of these alterations, referred to as non-specific molecular profile). A diagnostic algorithm using immunohistochemical markers and one molecular test has been applied. The prognostic impact of the molecular classification has repeatedly been shown by independent groups and is of particular relevance in high-grade and high-risk tumours.371–376 All diagnostic tests should be performed in conjunction due to the occurrence of ‘double classifiers’.377 Other biomarkers such as L1 cell adhesion molecule expression or mutations in CTNNB1 may be potentially useful for low-grade endometrioid carcinomas with non-specific molecular profile, but further investigations are required.378–381 According to the ESGO/ESTRO/ESP guidelines, adjuvant treatment recommendations for endometrial carcinoma strongly depend on the prognostic risk group, as follows4–6:
Low risk: no adjuvant treatment is recommended. When molecular classification is known, omission of adjuvant treatment should be considered for patients with endometrial carcinoma stage I–II, low risk based on pathogenic POLE mutation. For the rare cases of patients with endometrial carcinoma stage III–IVA and pathogenic POLE mutation, there are no outcome data with the omission of the adjuvant treatment. Prospective registration is recommended.
Intermediate risk: adjuvant brachytherapy can be recommended to decrease vaginal recurrence. Omission of adjuvant brachytherapy can be considered, especially for patients aged <60 years. When molecular classification is known, POLE mutation and p53 abnormal with myometrial invasion have specific recommendations.
High-intermediate risk (pN0 after lymph node staging): adjuvant brachytherapy can be recommended to decrease vaginal recurrence. External beam radiation therapy can be considered for substantial lymphovascular space involvement and for stage II. Adjuvant chemotherapy can be considered, especially for high-grade and/or substantial lymphovascular space involvement. Omission of any adjuvant treatment is an option. When molecular classification is known, POLE mutation and p53 abnormal have specific recommendations.
High-intermediate risk cN0/pNx (lymph node staging not performed): adjuvant external beam radiation therapy is recommended, especially for substantial lymphovascular space involvement and/or for stage II. Additional adjuvant chemotherapy can be considered, especially for high-grade and/or substantial lymphovascular space involvement. Adjuvant brachytherapy alone can be considered for high-grade lymphovascular space involvement negative and for stage II grade 1 endometrioid carcinomas. When molecular classification is known, POLE mutation and p53 abnormal have specific recommendations.
High risk: external beam radiation therapy with concurrent and adjuvant chemotherapy, or alternatively, sequential chemotherapy and radiotherapy is recommended. Chemotherapy alone is an alternative option. Carcinosarcomas should be treated as high-risk carcinomas (not as sarcomas). When the molecular classification is known, p53 abnormal carcinomas without myometrial invasion and POLE mutation have specific recommendations.
The definition of prognostic risk groups is presented in Online supplemental appendix 3 for both situations when molecular classification is known or unknown.
Recording Pertinent Information to Improve Quality of Care
Proper documentation is crucial for the quality of surgical care. Several studies highlighted the association of the use of standardized operative reports and the acquisition of more complete and interpretable operative data compared with the use of non-standardized operative reports.382–385 Synoptic reporting methods were developed as a result of the lack of essential informations in the narrative operative reports in other surgical disciplines.386–402 The synoptic operative report generally improves completeness and consistency in surgical documentation compared with the traditional narrative operative report, suggesting its incorporation into surgical practice. ESGO has approved a template for ovarian cancer operative reports.403 In the absence of an international validated standardized surgical report for endometrial carcinoma, the international development group considers that the surgical report must be structured and should include at least the following minimum requirements: status of abdominal findings at the start and end of surgery, description of tumor spread (if any), lymph node evaluation, complications, total blood loss, tracer used for the sentinel lymph node procedure, number of sentinel lymph nodes removed (if any), location of sentinel lymph nodes (if any), residual post-operative disease, location of residual disease (if any), kind of procedure (sentinel lymph node procedure, debulking, etc), adhesiolysis (yes vs no), aim of surgery (palliative vs curative), stage of the disease, and rupture of uterus.
The pathology report is a major component of patient management and its accuracy depends on several factors. Pre-analytical steps must be carried out in an optimal way to allow for adequate pathological evaluation. The inclusions of informative clinical and surgical data on the pathology request form, and accurate sampling and processing of the specimens, are the basis for a correct histological diagnosis and the provision of information on tumor staging. The pathology report should comprehensively include all the features that enable a patient with endometrial carcinoma to be placed into a risk group, which ensures the appropriate management. It should include all the parameters affecting tumor staging and patient management.
Structured morbidity and mortality conferences are required for quality assurance of surgical care. Complications, reoperations, readmissions, secondary transfers to intermediate or intensive care units, and deaths should be discussed. The use of a validated surgical complications scoring system is encouraged. Several surgical complications reporting systems have been proposed in the 1990s.404–410 The therapy needed to manage a specific complication remains the cornerstone for ranking a complication. The most commonly used scoring system for post-operative complications is the Clavien-Dindo classification. It consists of five severity grades and focuses on the interventions needed, with a major emphasis on the risk and invasiveness of the therapy used, to correct a complication.404 405 A 5-year evaluation demonstrated its validation, reproducibility, and applicability worldwide, irrespective of the cultural background and in many fields of surgery.411 Several indexes based on the Clavien-Dindo classification and modifications of this classification have been proposed and used in large multi-centric studies.412–422 Proactive reporting of the recurrences/deaths in institutions/centers is also needed.
Scoring SYSTEM/ESGO accreditation
The ESGO accreditation of centers for endometrial carcinoma surgery is an award to institutions that offer patients the specific skills, experience, organization, and dedication that are required to achieve optimal levels of surgical care. The ESGO accreditation is based on the completion of these QIs and a scoring system that has been developedand internally, validated by the international development group. To do so, each QI was associated with a score, and an assessment form was built (Online supplemental appendix 4). The form can also be used to support the self-assessment, quality assurance programs, or the external assessment of an institution.
The sum of the individual scores being 143, it was decided that an institution that meets at least 80% of the score (score ≥115) provides satisfactory surgical management of patients with endometrial carcinoma. Centers interested to become accredited are also required to meet the minimum required targets of QIs 1 and 2. Centers receiving the ESGO accreditation will be entitled to use the subtitle ‘ESGO accredited center in endometrial carcinoma surgery’, to use the ESGO logo in its endometrial carcinoma related communication, and be listed on the ESGO website as accredited center for patients’ and physicians’ reference.
ESGO has also developed criteria that distinguish centers with accreditation for endometrial carcinoma surgery into two categories, either ‘Standard Accreditation’ or ‘Center of Excellence’. These criteria are outlined in Box 1. Centers accredited as a Center of Excellence may then build a network for education, training, and research. The system will have to be refined in the future with the feedback provided by the scoring of candidate centers, and by prospective research on the multivariate correlation between survival outcome, characteristics of the patient, and indicators.
Center criteria for ESGO accreditation for endometrial carcinoma surgery: (A) Standard Accreditation and (B) Center of Excellence
(A) Entry criteria for standard ESGO accreditation for endometrial carcinoma surgery
Sum of the individual scores ≥115 (>80% of the score)
All the following criteria must apply (minimum required targets should be met): 1, 2
(B) Requirements for ESGO accreditation for endometrial carcinoma surgery as a Center of Excellence
Sum of the individual scores ≥115 (>80% of the score)
All the following criteria must apply (optimal targets should be met (if any)): 1, 2, 3, 5, 10, 15, 17, 20, 21, 22, 29
Publication of three articles on endometrial carcinoma authored by a gynecological surgical oncology member of the team over the last 3 years, including at least one article as first or last author
Ethics statements
Patient consent for publication
Acknowledgments
The authors thank the 143 international reviewers (physicians and patient representatives, online supplemental appendix 2) for their valuable comments and suggestions.
References
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors The development group (including all authors) is collectively responsible for the decision to submit for publication. NC (chair), JP (chair), and FP (methodologist) wrote the first draft of the manuscript. All other contributors actively gave personal input, reviewed the manuscript, and gace final approval before submission.
Funding All costs relating to the development process were covered from ESGO funds.
Competing interests NC: advisory boards for Akesobio, Ensai, GSK, AstraZeneca, Mersana, Seattle Genetics, eTherRNA immunotherapies; NV grants for travelling from Roche, Genmab, Amgen and educational fees from MSD, Medscape Oncology, TouchIME. NRA-R: research grants (paid to his institution) from Stryker/Novadaq and GRAIL and funds from the NIH/NCI Cancer Center (support grant P30 CA008748). BA: advisory boards for Roche, Tesaro/GSK, Amgen, MSD; grants for traveling from Roche, Tesaro/GSK, Pharmamar; and educational fees from Roche, Tesaro/GSK, Celgene, Clovis, AstraZeneca, Novartis. DC: advisory boards for Akesobio, AstraZeneca, GSK, MSD, Novocure, Roche, Seagen, Sotio. AF: advisory boards for AstraZeneca, MSD and grants for traveling from Pharmamar. CF: advisory boards for Roche, Ethicon, Sequana, GSK, MSD/AZ, Clovis, Tesaro. CM: advisory boards for Roche, Novartis, Amgen, MSD, AstraZeneca, Pfizer, Pharmamar, Cerulean, Vertex, Tesaro, GSK and grants for traveling from Roche, Novartis, Amgen, MSD, Pharmamar, AstraZeneca, Tesaro, GSK. DQ: advisory boards for Arquer Diagnostics Ltd. JS: advisory boards for Novocure, Roche, Pfizer, AstraZeneca, GSK, Clovis, Eisei and grants for traveling from Roche, GSK, AstraZeneca. IV: consulting activities for Agenus, Aksebio, Amgen (Europe) GmbH, AstraZeneca, Bristol Myers Squibb, Clovis Oncology Inc, Carrick Therapeutics, Deciphera Pharmaceuticals, Eisai, Elevar Therapeutics, F. Hoffman-La Roche Ltd, Genmab, GSK, Immunogen Inc, Jazzpharma, Karyopharm, Mersana, Millenium Pharmaceuticals, MSD, Novocure, Novartis, Octimet Oncology, NV, Oncoinvent AS, Seagen, Sotio a.s., Verastem Oncology, Zentalis; contracted research (via KULeuven) for Oncoinvent AS, Genmab; corporate sponsored research for Amgen, Roche; and grants for traveling and accommodations from Amgen, MSD, Tesaro, AstraZeneca, Roche. PW: advisory boards for Amgen, AstraZeneca, MSD, Novartis, Pfizer, Roche, Clovis, GSK and grants for traveling from Roche, Novartis, AstraZeneca. JP: advisory boards for Intuitive surgical, Medtronics.
Provenance and peer review Not commissioned; internally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.