Article Text

Statistics from Altmetric.com
- gynecologic surgical procedures
- ovarian cancer
- surgical oncology
- cytoreduction surgical procedures
- peritoneal cavity
Summary
Complete cytoreductive surgery without residual tumor is one of the most important prognostic factors in advanced ovarian cancer patients.1 During cytoreductive procedures, it is not unusual to require multiple digestive and/or visceral resections,2 which undoubtedly increase surgical morbidity and can also decrease patients’ quality of life.3 Therefore, it is essential to be as conservative as possible during cytoreductive procedures and to avoid, whenever possible, multivisceral resections without compromising the main goal of the surgery which is to achieve the absence of residual tumor. In this video article (Video 1) we show the surgical approach of the left upper quadrant in a patient with peritoneal carcinomatosis from ovarian origin who underwent an en-bloc left diaphragmatic peritonectomy, splenectomy, and infragastric omentectomy, among other procedures which are not included in the video. The surgery was carried out in a French Comprehensive Cancer Center by a senior oncological surgeon, following Sugarbaker principles.4 To perform the surgery, we used different energy instruments, a multifunctional device which employs ultrasonic energy and advanced bipolar energy, a bipolar forceps, a monopolar tip, and a monopolar roller ball. We divided the surgical procedure in the 10 following steps:
Step 1: Surgical exposure
Step 2: Beginning of left diaphragmatic and paracolic gutter peritonectomy
Step 3: Mobilization of the splenic flexure of the colon
Step 4: Spleen mobilization
Step 5: Complete left diaphragmatic peritonectomy
Step 6: Hepatic mobilization
Step 7: Infragastric omental detachment
Step 8: Splenic vascular pedicle ligature
Step 9: Coloepiploic detachment
Step 10: Chest tube insertion
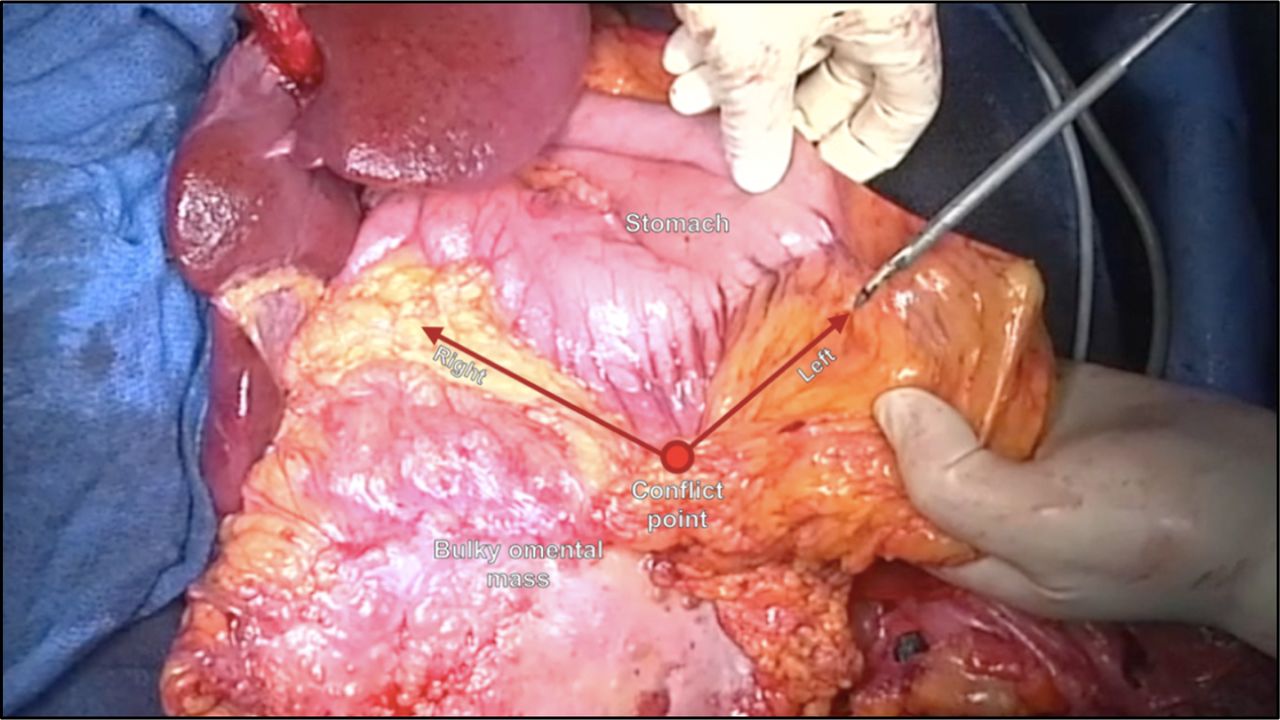
To summarize, we propose an alternative surgical approach to spare a transverse colectomy in a patient who presented with an omental cake highly adherent to the transverse colon. It is crucial to reduce the surgical radicality of cytoreductive surgery in patients with advanced ovarian cancer, without hindering the oncological outcome.

{kind=link}
Infragastric omental detachment with gastroepiploic arcade preservation.
Data availability statement
Data are available upon request.
Ethics statements
Patient consent for publication
Footnotes
Twitter @AngelesFite, @Alejandra
Contributors MAA: Conceptualization, video editing, writing-original draft. HL: Conceptualization, video editing, writing-original draft. FM: Conceptualization, video editing, writing-original draft. MD: Conceptualization, video editing, writing-original draft. AM: Conceptualization, project administration, supervision, writing-review. GF: Conceptualization, project administration, surgery and video recording, supervision, writing-review.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests GF reports personal fees from Olympus outside of the submitted work.
Provenance and peer review Not commissioned; externally peer reviewed.