Article Text

Statistics from Altmetric.com
Case presentation
A 27-year-old G1P1 patient diagnosed with a moderately differentiated squamous cell carcinoma of the cervix after cervical biopsy presented for counseling regarding fertility-sparing treatment immediately after diagnosis. The patient had no significant past medical history nor abdominal surgeries. She reported no history of smoking or drug abuse.
Pelvic examination revealed a 2 cm cervical tumor with no parametrial invasion, 2018 International Federation of Gynecology and Obstetrics (FIGO) stage IB1. Colposcopy exam showed a 2 cm extensive acetowhite lesion at the 6 o'clock position with no vaginal compromise. This was performed to confirm the size of the lesion. A pelvic magnetic resonance imaging (MRI) scan was obtained.
Dr Chacon
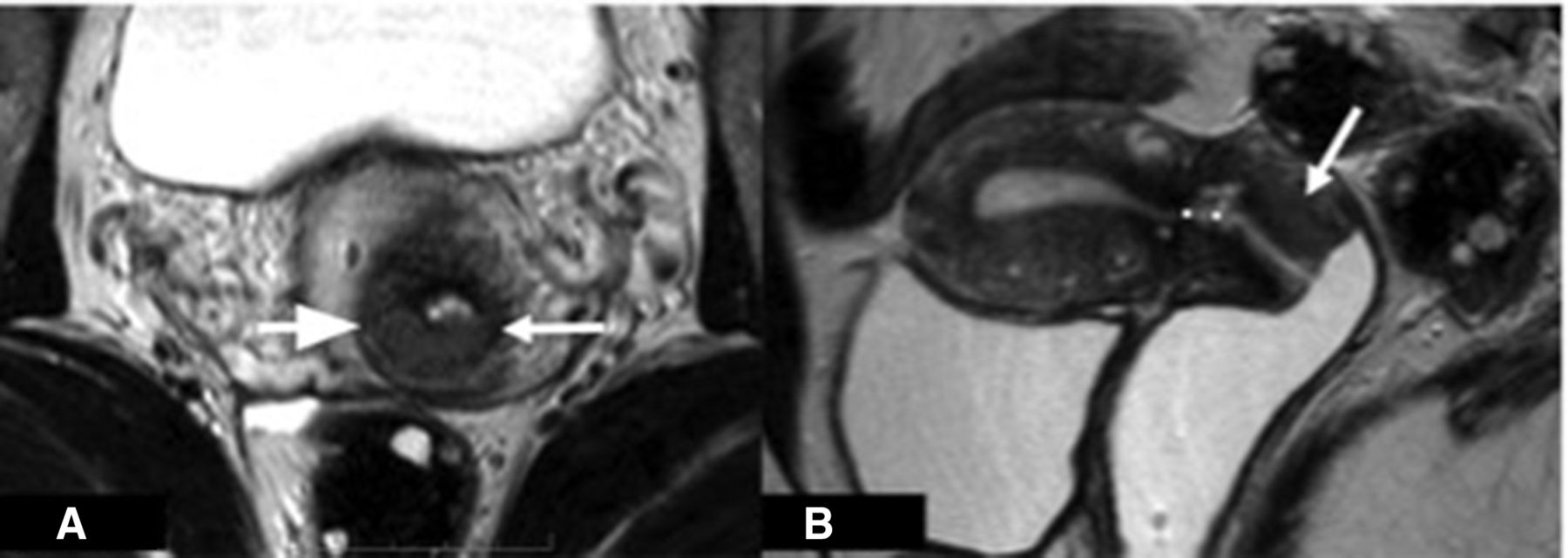
Abdominal and pelvic MRI showed a cervical mass with an intermediate signal on T2. Its measurements were 2 cm at its larger dimension and 1 cm distal to the internal cervical os. Neither parametrial involvement nor pelvic adenopathy were seen (Figure 1).

Pelvic magnetic resonance imaging (axial and sagittal) T2-weighted show a cervical mass with an intermediate signal on T2 (A, arrows). The mass measured 2 cm at its larger diameter, 1 cm distal to the internal cervical os (B, dotted line).
The patient was presented at the multidisciplinary conference composed of gynecologic oncologists, fertility specialists, and a psychologist. Based on physical examination and MRI images, as part of fertility-conserving treatment, the patient was recommended to undergo radical abdominal trachelectomy with sentinel node biopsy or three cycles of paclitaxel and carboplatin followed by radical trachelectomy. Oocyte cryopreservation was offered before starting treatment but the patient declined.
Dr Ribeiro
What options would you discuss with this patient at this time?
Retrospective studies have reported similar results for radical hysterectomy and radical trachelectomy for FIGO 2009 stage IB1 cervical cancer patients. 1 2 Selection is important because tumor size is not the only important factor. As an example, a patient with a 3 cm exophytic tumor may be a better candidate for radical trachelectomy than a patient with a 1 cm tumor located <1 cm from the internal cervical os.
Typically, neoadjuvant chemotherapy is used for patients with cervical tumors larger than 2 cm who were considered not ideal candidates for upfront radical trachelectomy. In this scenario, the neoadjuvant treatment seems to be an oncologically safe approach with adequate fertility outcomes. 3 4 However, patients with poor response to neoadjuvant chemotherapy or with adenocarcinoma histology and/or lymphovascular space invasion are potentially at higher risk for recurrence. 5 However, note that there are no studies evaluating neoadjuvant chemotherapy in improving distance to endocervical margin.
Traditionally, patients who wish to preserve fertility needed 10 mm of free endocervical margin 6 and 10 mm of residual cervix left for cerclage. This means that from the tumor to the internal cervical os approximately 2 cm of margin is needed. More recently, according to the National Comprehensive Cancer Network (NCCN) guidelines for cervical cancer, 7 a distance of 3 mm of free cranial margin and approximately 5 mm of the cranial aspect of the cervix should be left for cerclage, thus making radical trachelectomy an option for an increasing number of patients. MRI is the best method for predicting a distance between the tumor and the internal os with an accuracy of 89.8%. 8
As was done in this case, when considering fertility-sparing surgery, it is important to properly counsel patients regarding disease risk as well as prenatal and perinatal issues. In addition, a consultation with a reproductive fertility expert is very important.
An abdominal C1 radical trachelectomy9 was performed by a Pfannenstiel incision. Blue dye and technetium (Tc-99m) were used to identify sentinel nodes. Two external iliac and one obturator lymph nodes were detected on the right side of the pelvis and one external iliac lymph node was detected on the left pelvis. No evidence of macrometastasis was seen at frozen section. A cerclage with non-absorbable suture and a Smit sleeve with absorbable suture were placed before connecting the cervix to the vagina. Estimated blood loss was 400 mL, surgical time was 190 minutes with no intra-operative complications. The patient was discharged on post-operative day 2 without a ureteral catheter.
Dr Ribeiro
Please provide your comments regarding the surgical approach
Although the use of minimally invasive surgery is associated with worse disease-free and overall survival in patients undergoing radical hysterectomy as demonstrated by Ramirez et al in the LACC trial, 10 to date retrospective data show that the use of minimally invasive surgery appears safe in the radical trachelectomy setting. 11 An ongoing registry study (the IRTA Study) 12 is comparing open versus minimally invasive radical trachelectomy and the final results from this study are still awaited. One should note that extra care must be taken with the basic oncologic principles, such as avoiding manipulation of the tumor or its exposure to the pelvic cavity. Kong et al demonstrated that patients who underwent laparoscopic radical hysterectomy who have had intra-abdominal colpotomy had a three-fold higher risk of recurrence when compared with patients who underwent vaginal colpotomy.13
Prospective data 14–16 support the feasibility of sentinel lymph node detection in early-stage cervical cancer patients and suggest that extensive pelvic lymph node dissection may be safely avoided. However, not all guidelines consider exclusive use of sentinel lymph node dissection as standard. The European guidelines for the management of patients with cervical cancer 17 suggest that the standard lymph node staging procedure is systematic pelvic lymphadenectomy. The SENTICOL III trial 18 is evaluating survival and health-related quality of life after sentinel lymph node biopsy or sentinel lymph node biopsy + pelvic lymphadenectomy in early cervical cancer.
Dr Wernicke
Pathologic examination of the radical trachelectomy and the biopsy of bilateral sentinel lymph node specimens exhibited a moderately differentiated squamous cell carcinoma of the cervix ( Figure 2A ). A section of the endocervical margin was received for intra-operative consultation that was negative for infiltrating tumor and intraepithelial lesion. Depth of invasion was 10 mm of 25 mm, lymphovascular space invasion was present ( Figure 2B ), and the distance to the endocervical margin was 3 mm. Bilateral sentinel lymph nodes were studied with an ultrastaging protocol with no evidence of any metastases.
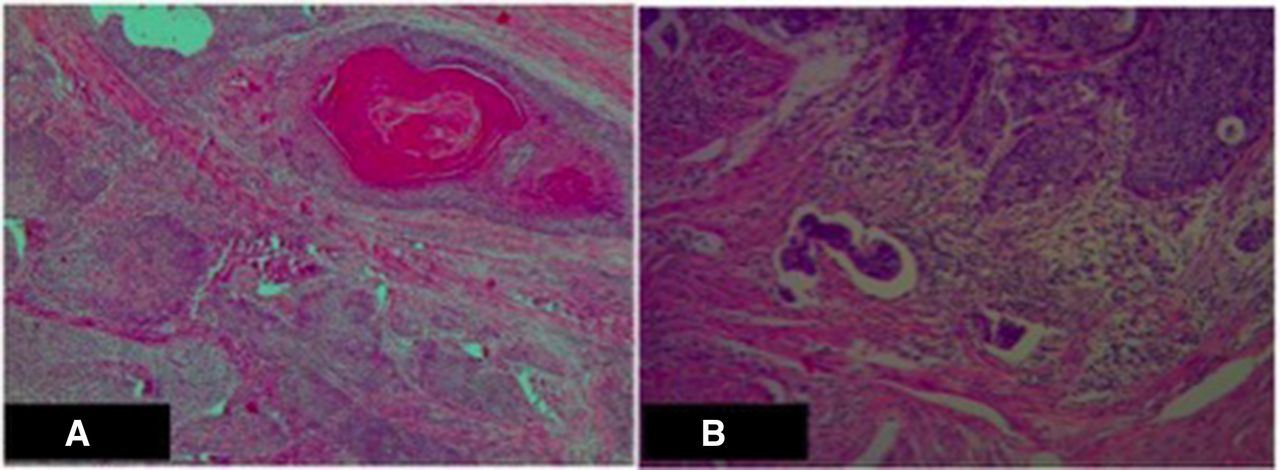
Radical trachelectomy specimen (hematoxylin & eosin). (A) Squamous cell carcinoma infiltrating the outer half of the myocervix. (B) Lymphovascular space invasion.
Following evaluation of the pathology report, and given the lymphovascular invasion, deep stromal infiltration, and tumor size of 21 mm, the patient was advised to complete treatment with pelvic radiation therapy, based on Sedlis criteria,19 or just observation.17 The patient decided to undergo the adjuvant treatment. At this time a new fertility multidisciplinary visit was offered in consideration of oocyte preservation and ovarian laparoscopic transposition. The patient accepted gamete cryopreservation, obtaining 12 oocytes, but she insisted on preserving the vitality of her uterus. She was informed about the existence of uterine transposition, and the risks and the lack of experience that exist regarding this technique. This novel procedure after radical trachelectomy had never been performed in Argentina, therefore the case was presented to our ethics committee. Once approved by the committee, it was decided together with the patient to perform a laparoscopic uterine transposition before initiation of radiation therapy. The patient and her husband were both infected with coronavirus (COVID-19) and consequently there was a lag time of 40 days between the radical trachelectomy and uterine transposition.
Dr Ribeiro
Please provide your thoughts regarding the role of uterine transposition in this patient
First, we recommend that all women who are being considered for uterine transposition are made aware of the novelty of this technique and the limitations in our present knowledge. These cases should all also be carefully and thoughtfully discussed with all oncologic providers to make sure that they are truly reasonable candidates for this procedure. It is critical that all providers are aware of the plans for the procedure and are also assured that oncologic outcomes will not be compromised.
Second, all patients must be offered the standard methods of fertility preservation, even if they accept the uterine transposition, as in the presented case. We strongly recommend embryo and/or oocyte cryopreservation because it can be a backup if uterine preservation does not work and help patients get pregnant if the uterine preservation works but the patient is unable to get pregnant spontaneously.
Third, the management of patients with early-stage cervical cancer following primary radical hysterectomy has been mostly based on Sedlis criteria, 19 and this has been extended to patients who undergo radical trachelectomy. However, some authors, 20 21 based on retrospective data, found that the administration of adjuvant external beam radiation therapy after radical hysterectomy was not associated with a survival benefit compared with observation alone, specially when type C1 radical hysterectomy was performed. 22 Cibula et al 21 reported that the recurrence rate in this group was 6.3% and the local recurrence rate 1.6%, without adjuvant treatment, with a median follow-up of 6.1 years. The death rate was 7% versus 14%, but was not statistically different. Based on these findings, the European Society of Gynecological Oncology guidelines consider that when an adequate type of radical hysterectomy has been performed observation is an alternative option. 17 It is important to understand that these studies have limitations such as retrospective data and small sample size, leading to insufficient number of patients to reach statistical power.
Regarding uterine transposition, one should note that it seems feasible after radical trachelectomy. In addition, menses and hormonal function are maintained, but this information is based on very limited data, published by our group. 23 Complications may occur and based on our experience (not published data) uterine necrosis and cervical stenosis are the major concerns. Due to limited experience, it is not possible to accurately predict all complications and patients must be aware of this when consenting to having a uterine transposition. Definitive oncologic safety and uterine viability to conceive are still unresolved issues. A major issue related to uterine transposition in patients who have had simple or radical trachelectomy is the risk of recurrence in the cervix. Mangler et al 24 reported seven (2.2%) cervical recurrences in 320 patients who underwent radical vaginal trachelectomies combined with laparoscopic removal of pelvic lymph nodes, with a median follow-up of 48 months. The authors did not clarify the recurrence rate in patients who met Sedlis criteria. 19 Patients must be properly informed about the recurrence risk, and should know that they may be incurring an extra risk of recurrence in favor of preserving their fertility. We recommend considering uterine transposition for cervical cancer only in highly selected cases. Also, it is imperative to follow up patients closely to further reduce morbidity in case of recurrence.
We performed the technique published by Ribeiro and colleagues 25 with some variations; principally we decided not to externalize the remaining cervix through the umbilicus and keep the entire uterus and adnexa inside the abdominal cavity. The reason was mainly to avoid the patient’s sensitivity to bleeding through her abdomen and to prevent possible infection. We used a gonadotropin-releasing hormone analog (GnRH) in order to induce amenorrhea. During the procedure the patient was placed in a dorsal modified lithotomy position. With a close technique (optic view) a 12 mm trocar was placed at the umbilical level, two accessory 5 mm trocars were placed in both iliac fossae, and finally a 12 mm trocar was placed at the hypogastrium.
Round ligaments were transected bilaterally, and the anterior peritoneum was transected to mobilize the bladder and identify the limits of the uterine–vaginal anastomosis. Most of these steps were performed with the use of ultrasonic energy. The infundibulopelvic ligaments were gently dissected to their origin. Special care was taken to avoid damaging the remaining vascular supply to the uterus. Once the uterus was completely disconnected from the vagina, we performed a frozen section biopsy of the remaining cervix that confirmed the absence of disease. The vaginal cuff was closed with absorbable sutures. The uterus was then transposed to the upper abdomen. At that time, the surgeon moved to the patient’s right side, with the first assistant between the patient’s legs, and the second assistant to the left side. The camera was placed in the hypogastrium trocar. The patient was placed in the reverse Trendelenburg position. We sutured the ovaries to each other and to the posterior wall of the uterus with absorbable suture to prevent them from being freely suspended in the abdomen. Finally, we fixed the uterus to the abdominal wall with non-absorbable suture. Estimated blood loss was 180 mL, and surgical time was 150 minutes with no intra-operative complications. The patient was discharged on post-operative day 2.
Dr Ribeiro
What are your thoughts on the variations performed to the previously described procedure?
In any new procedure, variations are expected and welcome. Uterine transposition is an evolving procedure, and we have reported 26 elsewhere some variations. Not attaching the cervix to the umbilicus has been the most controversial aspect of the procedure. There are both advantages and disadvantages. Direct inspection of the cervix, which is the end of the “flap”, is important to the procedure’s safety, specially if there is no Doppler ultrasound or MRI available to evaluate uterine perfusion in the post-operative period, as any necrosis can be seen immediately by clinical examination. For patients who have menstrual cycles during treatment, it can provide an excellent and simple way to evaluate uterine and ovarian function, and allow an outlet not just for menses but also mucoid secretion from the cervix. On the other hand, it is obviously awkward for patients and adds an additional surgical step and later dissection with a possible increased risk of dehiscence and infection. As a note, in 10 cases with the cervix attached to the umbilicus performed by our team to date, no umbilical infection occurred. It is important to note that post-trachelectomy patients do have a very short cervix that may hinder proper umbilical “anastomosis”. Because of this, we always place the cervix inside the abdominal cavity in cases like the one presented. A GnRH agonist should be given within 1–2 weeks of surgery to induce temporary ovarian suppression. Patients will need to receive appropriate redosing of the GnRH agonist until it is time to re-anastomose the cervix/uterus back to the vagina. The main disadvantage of this approach is that the induced menopausal symptoms may be difficult for some patients.
Suturing the ovaries to each other and to the posterior wall of the uterus seems a good option to prevent them from being freely suspended free in the abdomen. Suturing the ovaries to the subcostal margin is also an option. 26
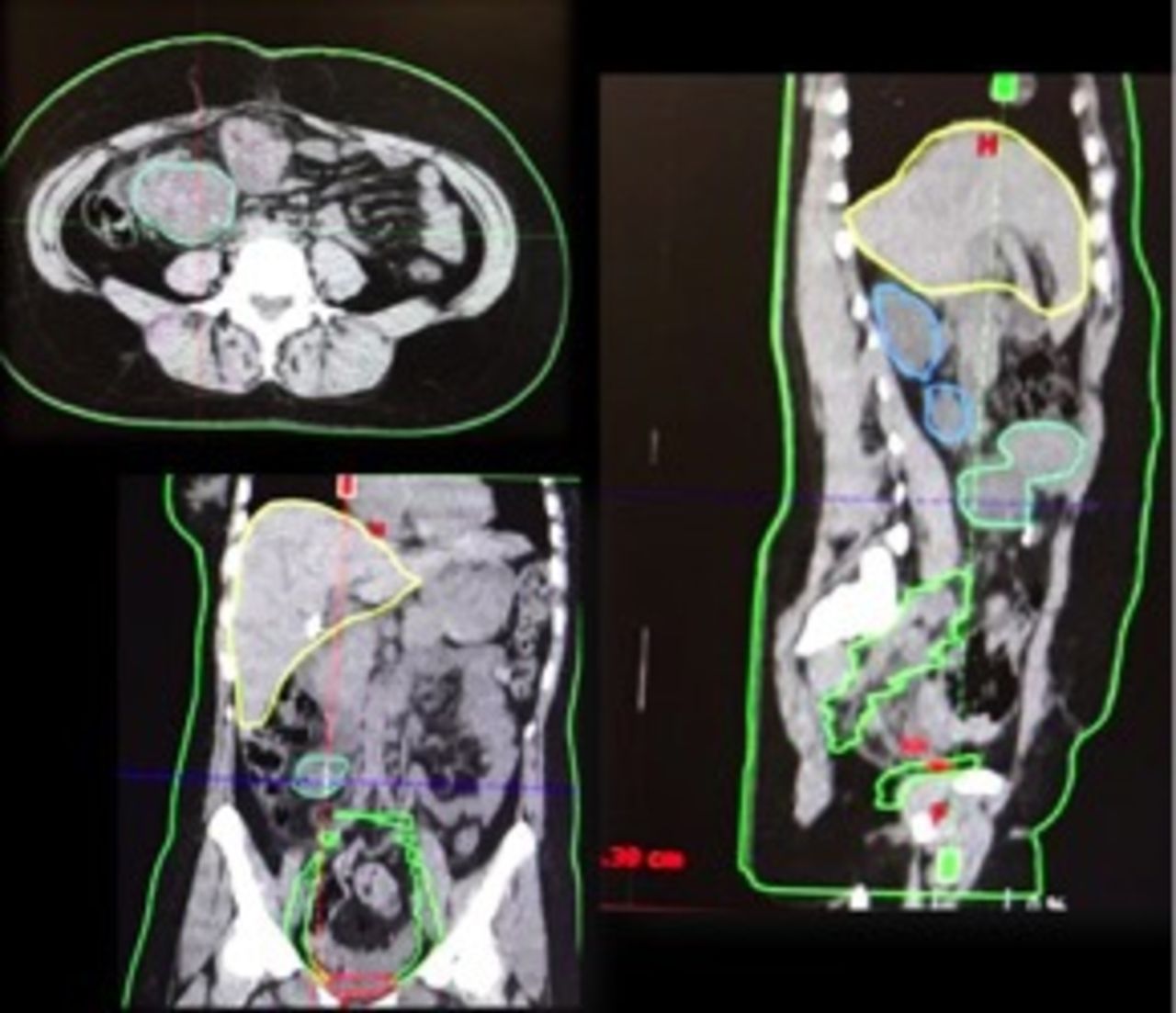
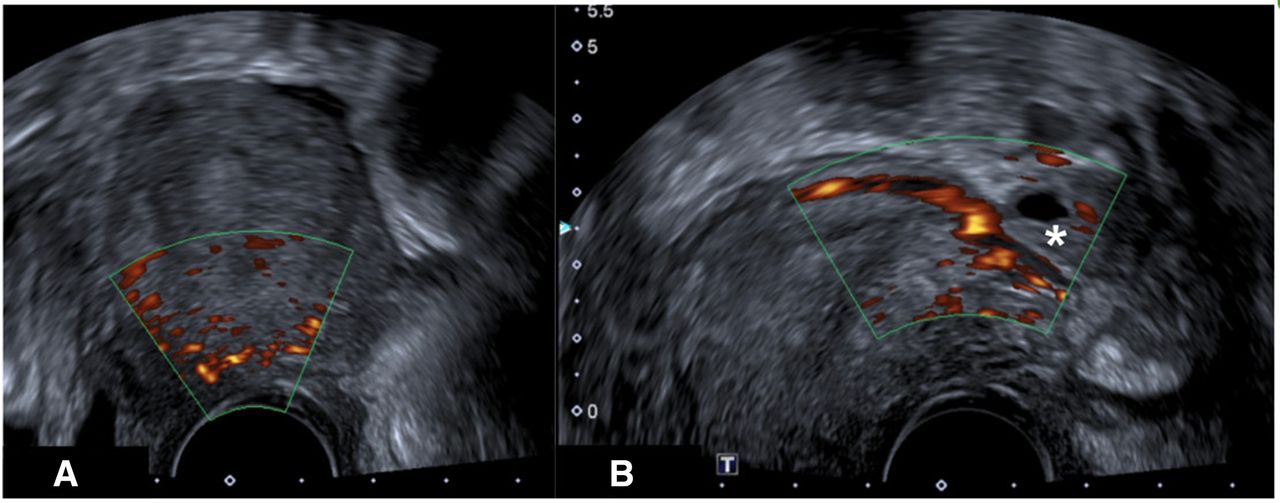
Uterine perfusion was assessed by Doppler ultrasound of the ovarian vessels on day 7 (Figure 3). A combination of triptorelin 3.75 mg subcutaneously (GnRh analogs) and oral dienogest 2 mg daily (progesterone) was used to prevent intra-abdominal menstruation. Three-dimensional pelvic radiotherapy was started 15 days after the surgery and was combined with cisplatin at a dose of 40 mg/m2 once a week (Figure 4). The patient received 5000 cGy over the course of 5 weeks without complications.
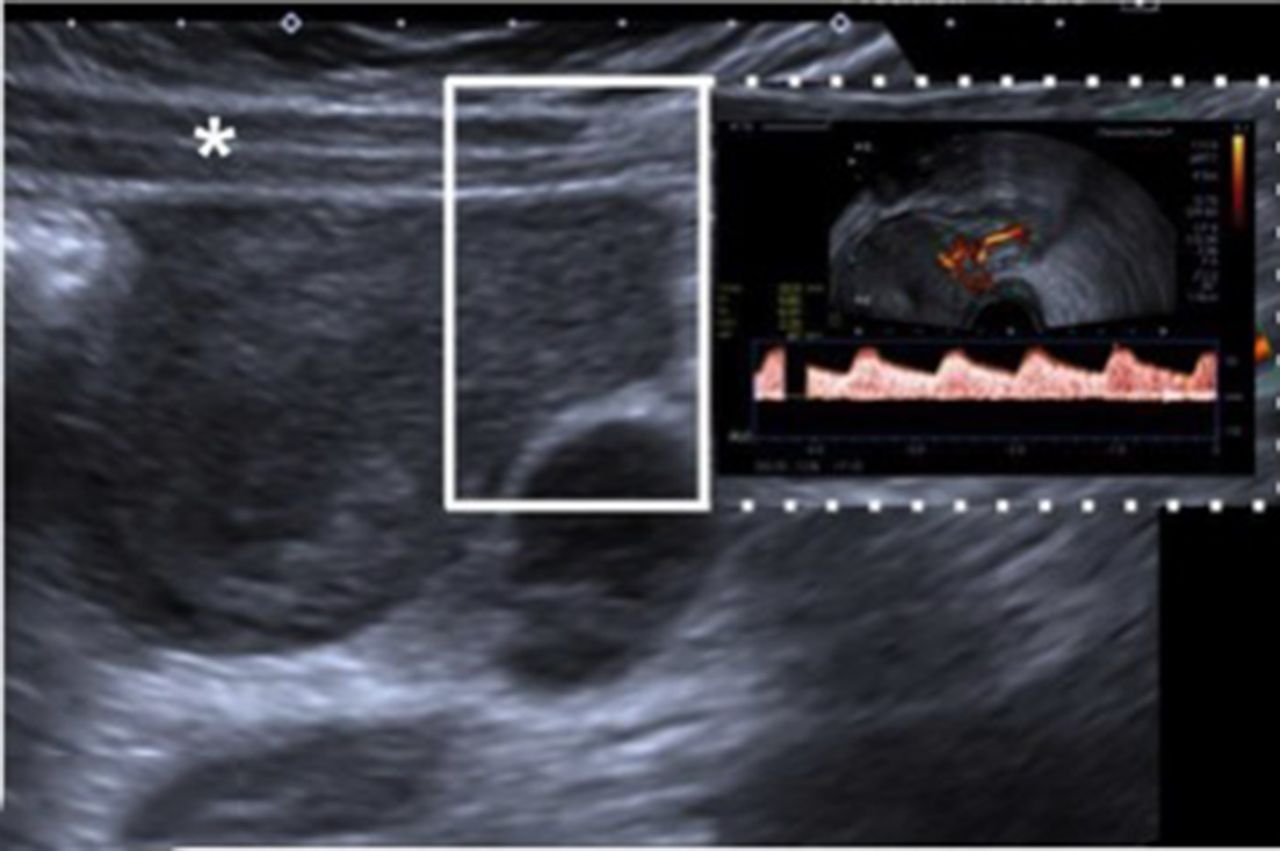
Abdominal ultrasound with Doppler at day 7 after uterine transposition. An abdominal ultrasound with Doppler (sagittal plane) was performed, demonstrating a normal remaining cervix with adequate vascularization on Doppler examination. Abdominal wall (*).

Computed tomography imaging for radiotherapy planning. Uterus and ovaries are outside the radiation field.
On the tenth day after completion of radiotherapy a laparoscopic uterine repositioning was performed. During the dissection of the right angle of the vagina, we identified an injury to the right ureter, just at the entrance to the bladder. Due to the radiation treatment received and the site of the injury, we decided to do a ureteral reimplantation with a psoas hitch. Subsequently, the cervix was introduced into the vagina and sutured to it with the use of polyglactin 2–0 separate sutures. Once the uterus was returned to its natural position, the round ligaments were sutured to the pelvic sidewall with the use of 3–0 non-absorbable sutures. The board ligaments were also reconstructed by suturing them to the pelvic sidewall along its natural course with the use of polypropylene 3–0 sutures.
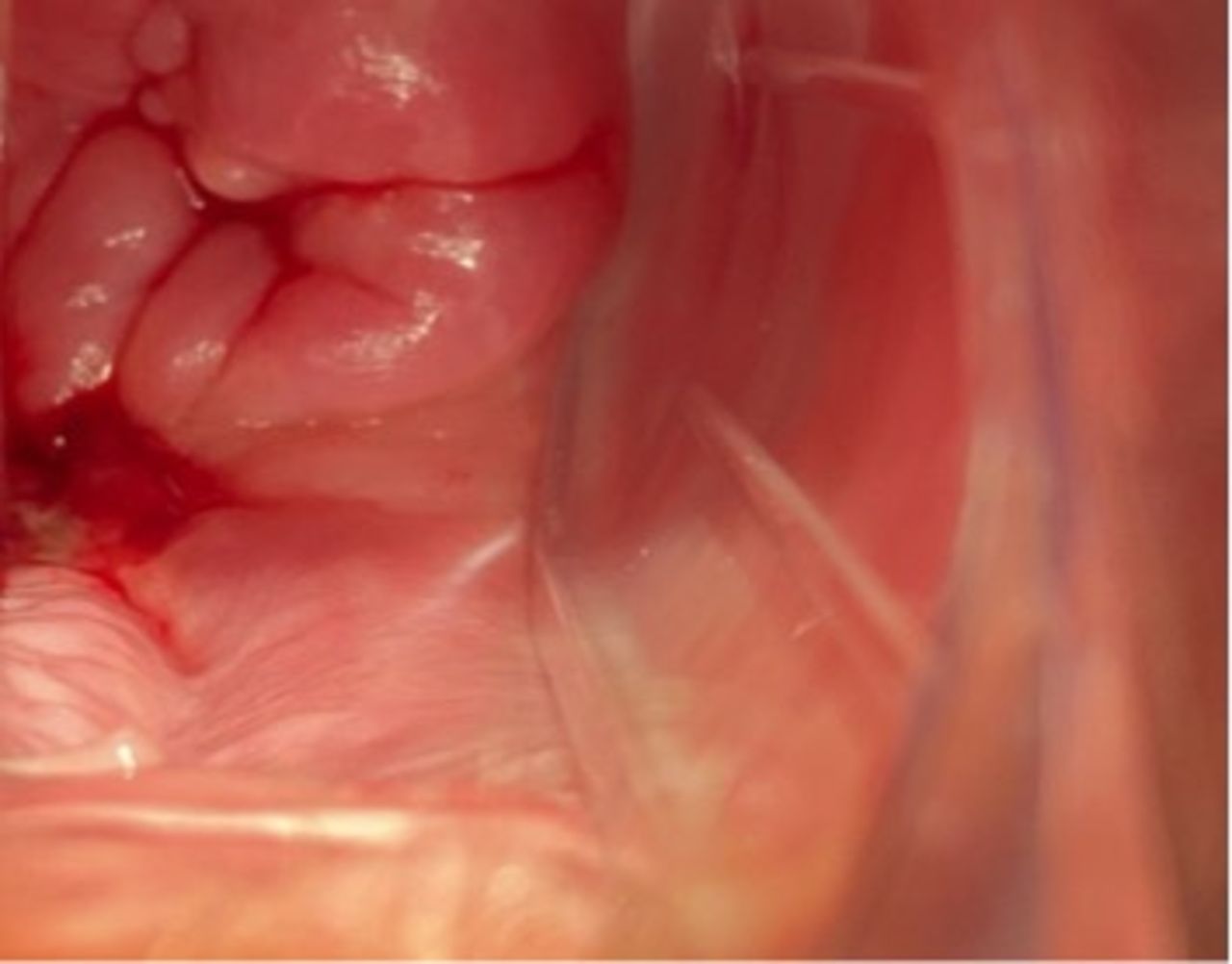
After checking the function of the ureteral reimplantation and leaving a double-J stent catheter, a drain was placed in the cul-de-sac. Estimated blood loss was 300 mL, and surgical time was 310 minutes. The patient was discharged on post-operative day 3. As a result of the ureteral injury, the patient remained for 7 days with a urinary catheter and the double-J stent was removed 30 days after the uterine repositioning. During this period of time the patient presented a low urinary infection treated with ciprofloxacin. Finally, she regained her menstrual cycle on day 40. Uterine and ovarian perfusion were re-evaluated by Doppler ultrasound (Figure 5). Following a normal physical examination (Figure 6), she resumed sexual activity using oral contraceptives 9 weeks after the last procedure. After 12 months of follow-up the patient has regular menses and no evidence of recurrence.

Transvaginal ultrasound with Doppler after uterine pelvic repositioning: (A) demonstrates the normal remaining cervix with adequate vascularization on Doppler examination and (B) shows the uterine arcuate vessels and left ovary (*) with satisfactory vascularization on Doppler.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cervix view 1 month after uterine pelvic repositioning.
Dr Ribeiro
What should be the routine surveillance for this patient?
Our recommended approach is with a clinical examination and cervical cytology (due the concern of not having irradiated the residual cervix) every 3 months for 2 years, then every 6 months until the patient completes 5 years of follow-up, then annually. Hormonal function (follicle-stimulating hormone, leutinizing hormon, estradiol) is measured once a year in order to diagnose early menopause. Chest x-ray once a year and pelvic MRI 6 months after surgery and then once a year is recommended.
Closing summary
Evolution of multimodal cancer therapy with subsequent improvement in survival rates, along with the incidence of cancer in young patients and the rise in the average age of first pregnancy, reinforces the importance of developing fertility-sparing approaches. Young women with cervical cancer who desire to preserve fertility may require radiotherapy as part of their treatment. For cervical cancer, it has been estimated that approximately 42% of patients planned for radical hysterectomy are younger than 40 years of age and ultimately 20% would be eligible for radical trachelectomy. Finally, approximately 5%–10% of patients undergoing radical trachelectomy would still have risk factors that require adjuvant radiotherapy. 20 21
For such patients, pelvic radiation hinders future fertility even after low doses. The oocytes are highly sensitive to radiation, and up to 50% may be destroyed after a dose of 2 Gy. 4 In addition, the uterus is also affected by pelvic radiotherapy, resulting in decreased uterine volume, reduced distensibility due to myometrial fibrosis, uterine vascular damage, and endometrial injury. 5 6 The only options for fertility preservation for these patients are oocyte or embryo cryopreservation and ovarian transposition. However, none of these techniques allow the patient to carry the pregnancy, thus requiring the use of a gestational carrier, which may not be an option due to religious, legal, and/or economic reasons.
Uterine transposition has emerged as a viable option for patients wishing to preserve their uterus and ovaries without impairing standard oncologic treatment. We reported 25 the first uterine transposition in 2017 for a patient with rectal cancer requiring neoadjuvant pelvic radiation. In 2018, Baiocchi et al 27 reported the first case after radical trachelectomy for a patient who fulfilled the Sedlis criteria for adjuvant radiotherapy.
Recently, we have published 23 the first series of cases of uterine transposition in women with gynecologic cancer. Four patients completed the uterine transposition and one patient decided on uterus removal before reimplantation. The median from uterine transposition to start of radiation was 14 (range 10–28) days. With a median follow-up of 25 months, there have been no recurrences. All four patients who completed the procedure have normal menstrual cycles, one failed to become pregnant, and the other three did not attempt it.
The small number of patients reported thus far in the literature is a strong limitation for any conclusion. However, the procedure is feasible and reproducible. Preliminary data suggest that uterine transposition may be safe for selected patients with cervical cancer that require pelvic radiotherapy after radical trachelectomy. Further studies are needed to determine the safety and efficacy of the procedure in terms of pregnancy preservation.
Ethics statements
Patient consent for publication
References
Footnotes
Twitter @-
Contributors DO: conception and design of the study, data collection, responsible surgeon, and manuscript preparation. RR: conception and design of the study, and manuscript preparation. JMS: conception and design of the study, and responsible surgeon.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.