Article Text

Abstract
Objective To evaluate the role of adjuvant chemotherapy in patients with surgical stage I-II endometrioid endometrial cancer (EC) with myometrial invasion (MI) >50%.
Methods We identified patients with stage I-II endometrioid grade 2 and 3 EC with MI >50% and negative nodes after pelvic ± para-aortic lymphadenectomy at four institutions (US and Italy). The association between adjuvant chemotherapy and cause-specific survival (CSS) or progression-free survival (PFS) was assessed with Cox proportional hazards models, adjusted for confounders using the inverse-probability of treatment weighting (IPTW).
Results From 1984 to 2012, 329 patients were identified. Median follow-up among those alive was 7.0 (interquartile range, 3.7–11.1) years. Five-year CSS was 86.1% (95%CI: 82.0–90.4%) and 5-year PFS was 82.2% (95%CI: 77.9–86.8%). Stage II (vs stage IB) was significantly associated with poorer CSS and PFS; older age with poorer PFS. With IPTW-adjusted analysis, adjuvant chemotherapy appeared to improve CSS (hazard ratio [HR]: 0.34; 95%CI: 0.11–1.03; P=.06) and nonvaginal PFS (HR: 0.36; 95%CI: 0.12–1.08; P=.07) (figures 1 and 2). Eleven (84.6%) of 13 para-aortic recurrences were observed in 194 patients who had neither para-aortic lymphadenectomy nor adjuvant chemotherapy. Conversely, no para-aortic recurrences were observed in 64 patients who received adjuvant chemotherapy.
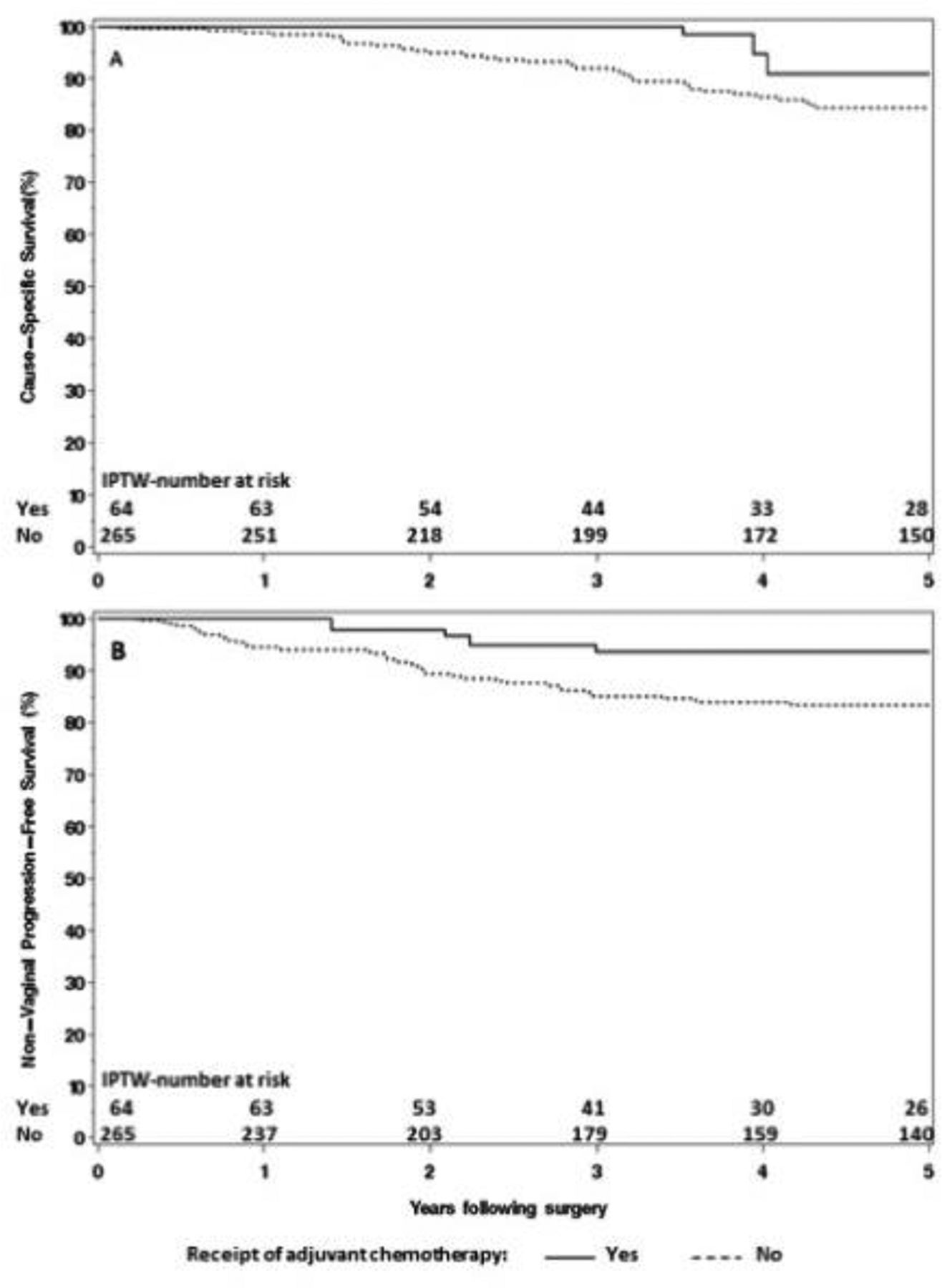
Inverse-probability of treatment-weighted cause-specific survival (A), and nonvaginal progression-free survival (B), according to receipt of adjuvant chemotherapy

{kind=link}
{kind=link}
Inverse-probability of treatment-weighted cause-specific survival among patients with FIGO stage IB (A) or stage II (B), according to receipt of adjuvant chemotherapy
Conclusions Adjuvant chemotherapy for surgical stage I-II endometrioid grade 2 and 3 EC with MI >50% appeared to improve CSS and nonvaginal PFS, although not meeting the conventional level of statistical significance. Stage II patients appear to benefit most from adjuvant chemotherapy. Chemotherapy ± para-aortic lymphadenectomy may help reduce para-aortic failures.