Article Text

Abstract
Introduction Frailty has been associated with poorer surgical outcomes and is a critical factor in procedural risk assessment. The objective of this study is to validate surgical outcomes in patients undergoing surgery for endometrial cancer (EC).
Methods Patients undergoing inpatient gynecologic surgery for EC were identified using the 2005–2017 National Inpatient Sample database. The Johns Hopkins Adjusted Clinical Groups (ACG) frailty-defining diagnosis indicator was used to designate frailty. Multivariate regression models were used to assess the association of frailty with post-operative outcomes and resource use.
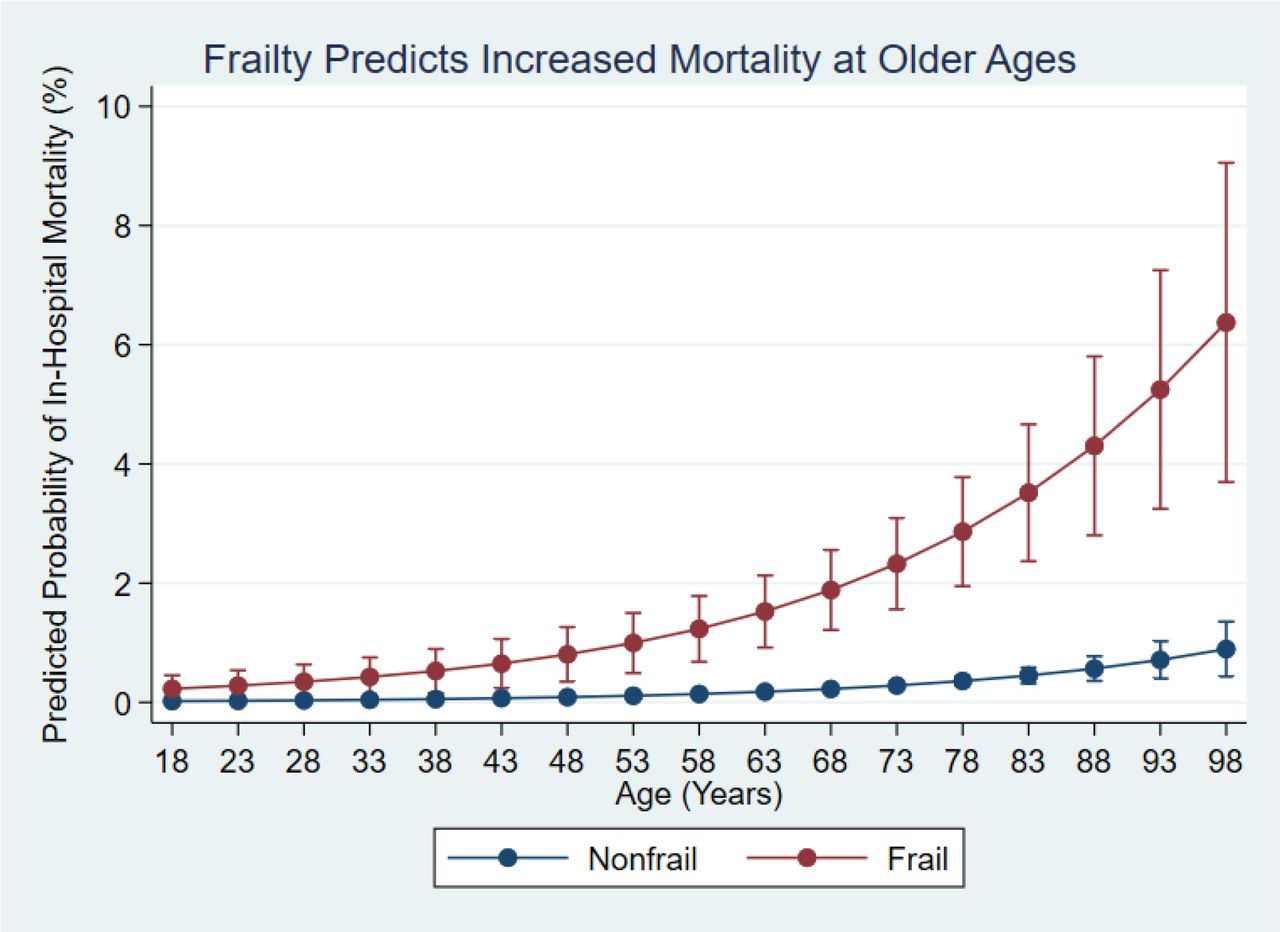
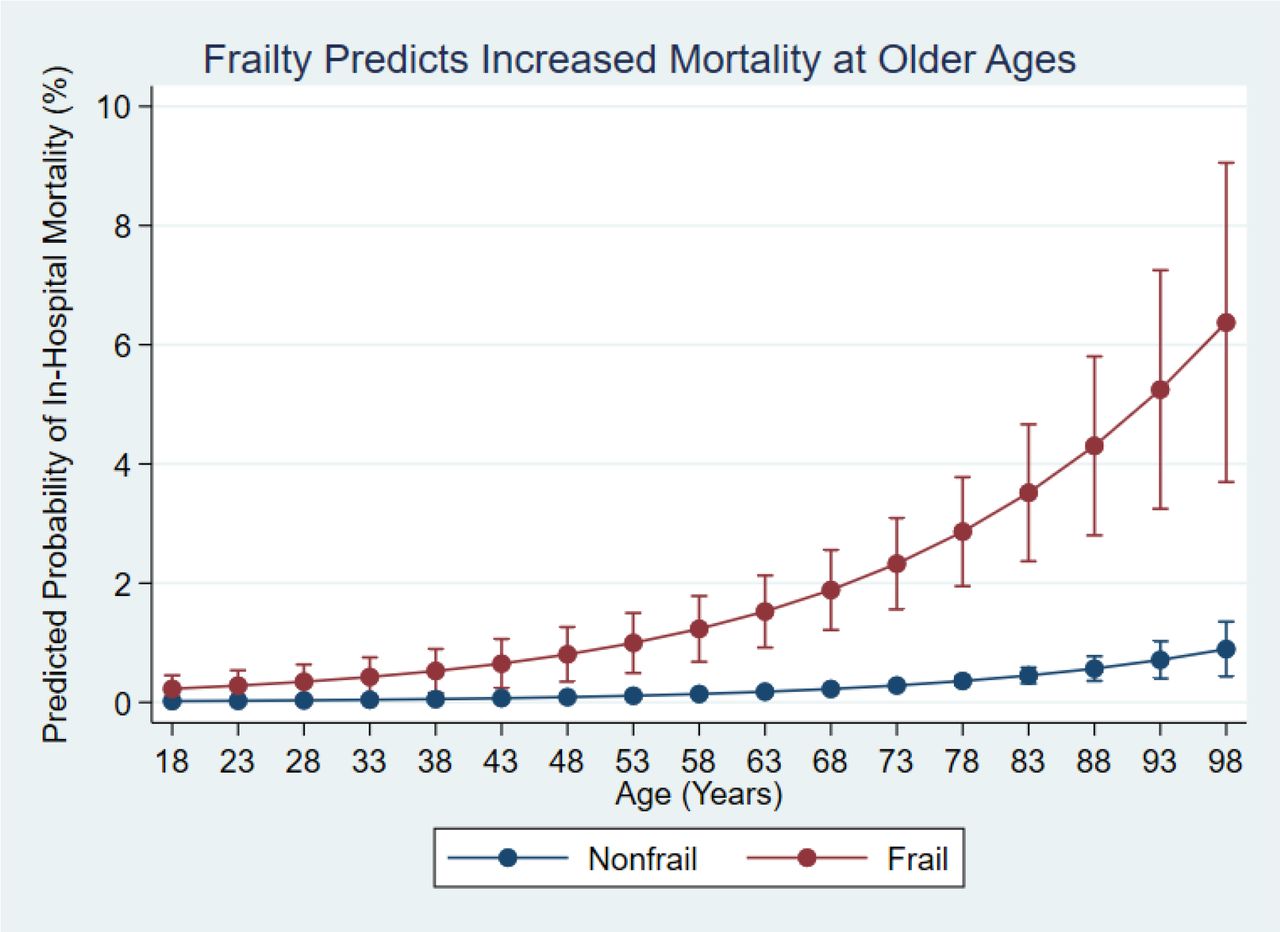
Results Of an estimated 339,846 patients, 2.9% (9,868) were considered frail. After adjusting for patient and hospital characteristics, frailty was associated with a four-fold increase in inpatient mortality (adjusted odds ratio [AOR]:4.1; p<0.001) and non-home discharge (AOR:5.2; p<0.001), as well as increased respiratory (AOR:2.6; p<0.001), neurologic (AOR:3.3; p<0.001), renal (AOR:2.0; p<0.001), and infectious (AOR:3.2; p<0.001) complications. While frail patients exhibit increased mortality with age (figure 1), the rate of mortality in this cohort decreased significantly over time (figure 2). Compared with non-frail counterparts, frail patients also had longer lengths of stay (7.6 days vs. 3.4 days; p<0.001) and increased hospitalization costs ($25,093 vs. $13,405; p<0.001).

{kind=link}
{kind=link}
Conclusion/Implications Frailty is independently associated with worse surgical outcomes, including mortality, and increased resource use in women undergoing surgery for EC. Though there have been improvements in mortality in more recent years, further efforts to mitigate the impact of frailty should be explored.