Article Text

Abstract
A 38 year old nulliparous woman with pemphigus vulgaris (PV) on oral prednisolone and azathioprine was referred to the Gynaecology service for an abnormal cervical cytological smear showing low-grade squamous intraepithelial lesion. She was asymptomatic, reported no abnormal vaginal bleeding, and had a 10 pack-year history of smoking.
Colposcopy was unsatisfactory with inadequate visualisation of the transformation zone due to severe cervico-vaginitis. A small focus of aceto-white epithelium was seen, surrounded by peeling, friable epithelium. HPV DNA test was negative. Punch biopsy demonstrated metaplastic squamous epithelium with intraepidermal suprabasal blister formation with acantholysis. Well-vascularised dermal papillae lined residual basal cells, giving rise to a tombstone appearance. There was no evidence of CIN/CGIN or invasive malignancy. An ulcer was also seen in the left buccal region.
Repeat colposcopy after 6 weeks showed a small ulcerated area at the biopsy site with rolled healing edges, and a separate small ulcer. Cervical smear and colposcopy 6 months later were unremarkable.
The incidence of cervical PV may be underestimated because women with PV are often managed by dermatologists without gynaecological input. In many published cases, cervical involvement was only detected after gynaecological examination due to symptoms such as dyspareunia, post-coital bleeding or vaginal discharge.
{kind=link}
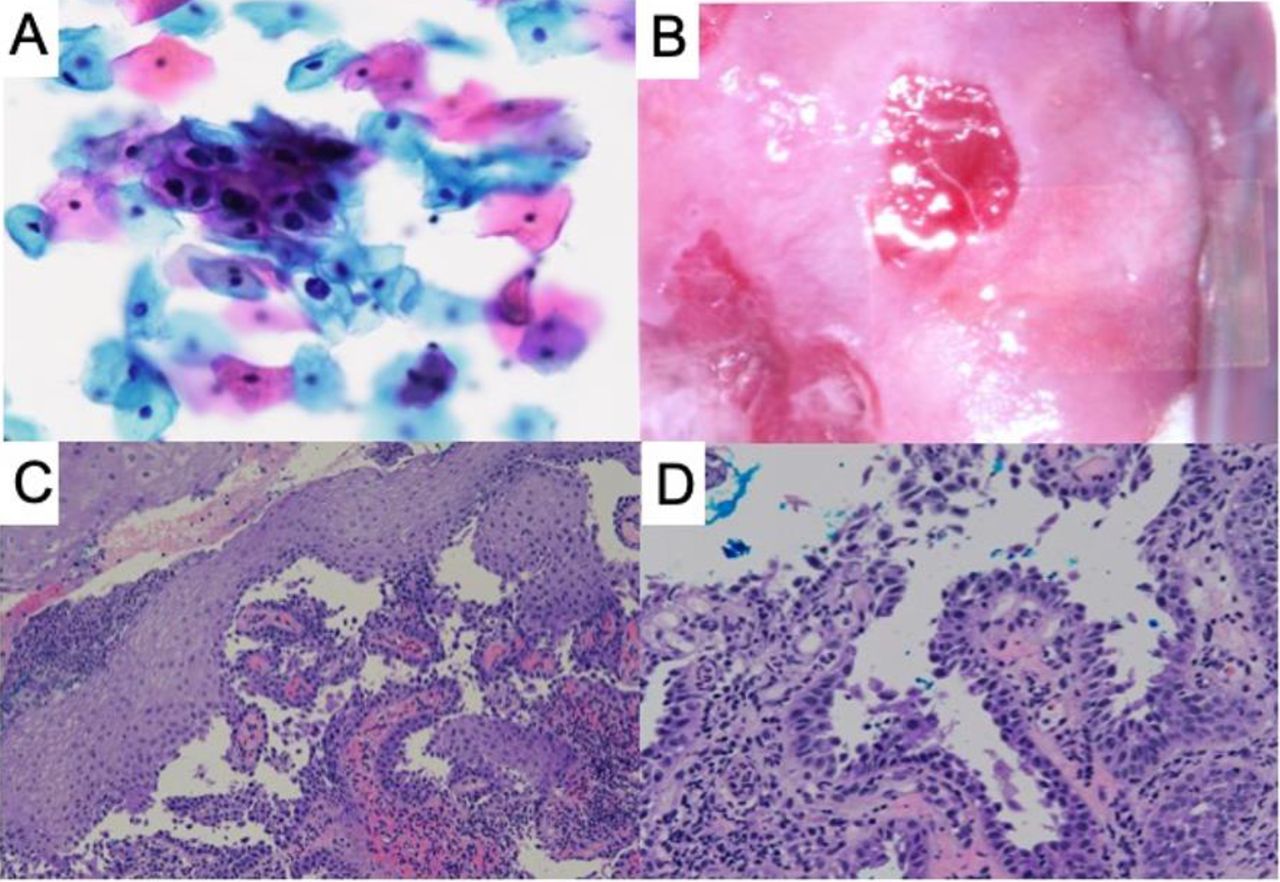
(A) Cervical smear containing scattered groups of abnormal keratinocytes with enlarged hyperchromatic nuclei, irregular nuclear membranes and bi-nucleation with perinuclear halo in keeping with koilocytosis; (B) Colposcopic appearance (high magnification); (C) Cervical tissue showing intraepidermal and suprabasal blister formation; (D) Well vascularised dermal papillae with residual basal layer giving rise to tombstone appearance
Cervical smears of patients with PV typically display acantholysis, which may be misinterpreted as reparative, inflammatory, or neoplastic change. There have been reports of unnecessary hysterectomy due to such misdiagnoses. Review by an experienced cyto-pathologist is required in the event of diagnostic uncertainty.