Article Text

Abstract
Objective In previous studies, neoadjuvant chemotherapy followed by interval debulking surgery was not inferior to primary cytoreductive surgery as initial treatment for advanced epithelial ovarian cancer. Our study aimed to compare surgical and survival outcomes between the two treatments in a large national database.
Methods Data were extracted from the National Cancer Database from January 2004 to December 2015. Patients with FIGO (International Federation of Gynecologists and Obstetricians) stage III-IV epithelial ovarian cancer and known sequence of treatment were included: primary cytoreductive (surgery=26 717 and neoadjuvant chemotherapy=9885). Tubal and primary peritoneal cancer diagnostic codes were not included. Residual disease after treatment was defined based on recorded data: R0 defined as microscopic or no residual disease; R1 defined as macroscopic residual disease. Multivariate Cox proportional HR was used for survival analysis. Multivariate logistic regression analysis was utilized to compare mortality between groups. Outcomes were adjusted for significant covariates. Validation was performed using propensity score matching of significant covariates.
Results A total of 36 602 patients were included in the analysis. Patients who underwent primary cytoreductive surgery had better survival than those treated with neoadjuvant chemotherapy followed by interval surgery, after adjusting for age, co-morbidities, stage, and residual disease (p<0.001). Primary cytoreductive surgery patients with R0 disease had best median survival (62.6 months, 95% CI 60.5–64.5). Neoadjuvant chemotherapy patients with R1 disease had worst median survival (29.5 months, 95% CI 28.4–31.9). There were small survival differences between primary cytoreductive surgery with R1 (38.9 months) and neoadjuvant chemotherapy with R0 (41.8 months) (HR 0.93, 95% CI 0.87 to 1.0), after adjusting for age, co-morbidities, grade, histology, and stage. Neoadjuvant chemotherapy had 3.5 times higher 30-day mortality after surgery than primary cytoreductive surgery (95% CI 2.46 to 5.64). The 90-day mortality was higher for neoadjuvant chemotherapy in multivariate analysis (HR 1.31, 95% CI 1.06 to 1.61) but similar to primary cytoreductive surgery after excluding high-risk patients.
Conclusions Most patients with advanced epithelial ovarian cancer may benefit from primary cytoreductive surgery. Patients treated with neoadjuvant chemotherapy should be those with co-morbidities unfit for surgery.
- ovarian cancer
- ovary
- ovarian diseases
- ovarian neoplasms
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, an indication of whether changes were made, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
HIGHLIGHTS
Patients who undergo primary cytoreductive surgery have improved survival compared to neoadjuvant chemotherapy.
Primary surgery with residual disease has equal survival to neoadjuvant chemotherapy without residual disease.
The 30-day and 90-day mortality is higher with neoadjuvant chemotherapy than with primary cytoreductive surgery.
Introduction
Upfront surgical debulking has been the treatment standard for primary ovarian cancer for many years. Over the past decade, however, prospective randomized controlled trials have shown neoadjuvant chemotherapy is not inferior to primary cytoreductive surgery, in regard to survival.1 2 More recently, the results of two new studies comparing neoadjuvant chemotherapy with primary cytoreductive surgery were presented, in attempts to address criticisms, such as reduced surgical aggressiveness, decreased survival compared with other studies, and extent of residual disease. Fagotti et al performed a superiority trial to assess progression-free survival and post-operative complications in patients receiving neoadjuvant chemotherapy versus primary cytoreductive surgery.3 There was no difference in progression-free survival between the two arms, but the authors found a significantly decreased number of post-operative complications with neoadjuvant chemotherapy. The surgical effort in this study was improved compared with the CHORUS and EORTC studies, with rates of optimal cytoreduction being 92.8% in the primary cytoreductive surgery group and 100% in the neoadjuvant chemotherapy group.3
Similarly, a phase III non-inferiority trial comparing overall survival between primary cytoreductive surgery and neoadjuvant chemotherapy did not show non-inferiority.4 The rates of optimal cytoreduction were lower than in the Fagotti study, with 37% in the primary cytoreductive surgery group and 82% in the neoadjuvant chemotherapy group.4 In addition to showing non-inferiority of neoadjuvant chemotherapy, the above studies demonstrated increased morbidity and mortality in patients undergoing primary cytoreductive surgery compared with interval debulking surgery. Quality of life has also been shown to be lower in this patient population.1 5 Both of the new studies, Fagotti et al3 and Onda et al,4 demonstrated a decrease in post-operative complications in the groups undergoing neoadjuvant chemotherapy.
In this study, we queried the National Cancer Database (NCDB) to better understand the outcomes of patient survival, morbidity, and mortality for patients with advanced epithelial ovarian cancer, and to use this information to facilitate patient selection for each respective primary treatment.
Methods
Patients that underwent initial primary cytoreductive surgery followed by chemotherapy were analysed as the primary cytoreductive surgery group. Patients selected for neoadjuvant chemotherapy initially received three or four cycles of chemotherapy followed by interval cytoreductive surgery. Neoadjuvant chemotherapy patients usually received three to four additional cycles of chemotherapy after surgery. Time of treatment initiation, either primary cytoreductive surgery or neoadjuvant chemotherapy, was also recorded. Residual disease after treatment was defined based on recorded data: R0 was defined as microscopic or no residual disease and R1 was defined as macroscopic residual disease. No continuous variable containing size of residual disease was available in the NCDB.
Patients
We extracted data from the Ovarian Cancer subset of the NCDB from 2004 to 2015: National Cancer Database Participant User File (PUF) Proposal ID: 2015.56. We excluded patients with non-epithelial tumors, those with early-stage (I-II) disease, and those with tubal or primary peritoneal cancers. We also excluded those with an unknown sequence of treatment or treatment other than primary cytoreductive surgery or neoadjuvant chemotherapy. Unfortunately, the NCDB contains de-identified patient-level data that do not identify hospitals, healthcare providers, or patients (see patients’ flowchart of inclusion/exclusion for more details of the selection process, Figure 1). There was a total of 26 717 patients that underwent primary cytoreductive surgery and 9885 patients that underwent neoadjuvant chemotherapy as first-line treatment for epithelial ovarian cancer that were included in the analysis of our study. Patients’ clinical characteristics are depicted in online supplementary Table 1.
Supplemental material

Inclusion and exclusion criteria from the National Cancer Database, Ovarian Cancer subset. Exclusion criteria were performed so that the final patient population included those with stage III-IV epithelial ovarian cancer whose primary treatment included either primary cytoreductive surgery or neoadjuvant chemotherapy. HIPEC, hyperthermic intraperitoneal chemotherapy; PCS, primary cytoreductive surgery.
Statistical Analysis
We performed bivariate analyses using Student’s t-test for continuous variables and Chi-square test for dichotomous variables to assess comparisons between treatment type (primary cytoreductive surgery or neoadjuvant chemotherapy) outcomes, and 30-day and 90-day mortality. Fisher’s exact test was used in the place of the chi-square test when cell sizes contained fewer than five patients. We used the same methods to assess the association of type of treatment with other covariates of interest: age, Charlson Comorbidity Index (CCI), age of diagnosis, stage, and histologic grade and type. Multivariable analyses using logistic regression modeling were used to account for potential effects of covariates found to be significant in univariate analyses. A final model adjusted for all significant covariates and treatment types was constructed.
Kaplan−Meier curves were used to estimate survival of both treatment types. The Cox proportional hazard ratio (HR) was used to compare survival of both therapeutic groups. The association with survival and other previously noted covariates of interest was also assessed with the Cox proportional HR. Then, a multivariate Cox proportional analysis was performed to account for all significant covariates in the univariate analyses. For this multivariate analysis we adjusted for the effect of all significant covariates and constructed a model with adjusted HRs and 95% confidence intervals (CIs).
A validation of the above analysis was performed by excluding patients at risk of not responding to chemotherapy, such as low-grade tumors or mucinous histology, and by excluding elderly or frail patients (based on the CCI), where the decision to do primary surgery may be biased. The multivariate survival and regression analyses were replicated in this modified database. Propensity score matching of the covariates was used to reduce any treatment assignment bias, and was performed with MatchIt, an R package.6 7
For all tests, p values <0.05 were considered statistically significant. Data analysis was performed using R environment for statistical computing and graphics (www.r-project.org).
Results
We included a total of 36 602 patients in the study: 26 717 underwent primary cytoreductive surgery and 9885 underwent neoadjuvant chemotherapy. The median age for those undergoing surgery was 61 (range 18–90) years, and 65 years (same range) for those that underwent neoadjuvant chemotherapy (p<0.001). The CCI was not 0 for 18.3% and 19.9%, respectively (p<0.001). Also, high-grade histology was 95.8% and 98.5%, respectively (p<0.001); mucinous histology was 2.9% and 1.0%, respectively, and serous histology was 71.1% and 74%, respectively (p<0.001). Analysis of the baseline characteristics of included individuals determined that patients who received neoadjuvant chemotherapy were overall older with more co-morbidities compared with the primary cytoreductive surgery group. Also, more patients in the neoadjuvant chemotherapy had higher-grade and advanced-stage tumors. The mucinous histologic type was more common in patients undergoing primary surgery. Those who received neoadjuvant chemotherapy had a higher rate of no gross residual disease (65.4%) compared with the primary cytoreductive surgery group (56.1%, p<0.001). Mortality (30 and 90 days) after surgery was higher in the neoadjuvant chemotherapy group (1% and 2.7% vs 0.3% and 2.2% in the surgery group, respectively, p<0.001 and p<0.005), although at 90 days there was no difference in mortality between groups, after excluding high-risk patients (online supplementary Table 1).
Survival Analysis
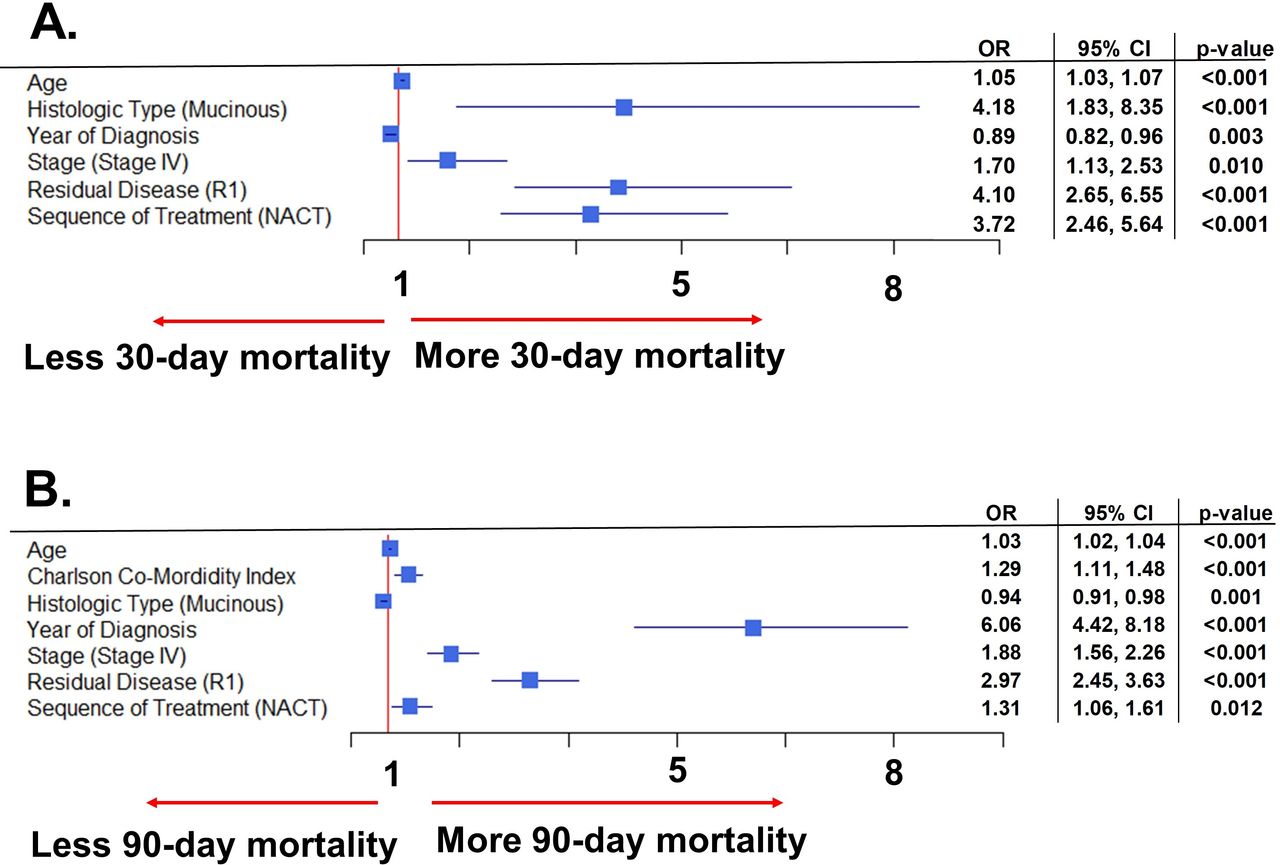
The univariate and multivariate survival analysis demonstrated mortality was increased with age, higher CCI, high histologic grade, mucinous histologic type, and more advanced FIGO stage. Presence of gross residual disease also contributed to increased mortality (Figure 2). In regard to sequence of primary treatment, those treated with neoadjuvant chemotherapy had a 37% higher mortality compared with the primary cytoreductive surgery group, median survival of 37.6 months (95% CI 36.7–38.5) and 50.4 months (95% CI 49.4–51.4), respectively, even after adjusting for the above contributing factors (Figure 2A). Conversely, mortality for epithelial ovarian cancer improved by year of diagnosis, the highest being in 2005 and the lowest in 2012. Therefore, after adjusting for age, stage, grade, histology, year of diagnosis, co-morbidities, and residual disease after surgery, patients that underwent primary cytoreductive surgery had better overall survival than neoadjuvant chemotherapy, with a 37% increased probability of dying for patients undergoing neoadjuvant chemotherapy (Figure 2B). These results hold true, even with replicate analysis excluding older patients (>75 years old), co-morbidities (CCI>0), low-grade cancers, mucinous subtypes, and adjusted for other covariates.

Mortality is increased with poor prognostic factors, but also with primary treatment of neoadjuvant chemotherapy. Prognostic factors including age, co-morbidities, grade, stage, mucinous histologic type, residual disease, and sequence of treatment are analysed in Figure 2A. The forest plot (Figure 2B) was attained after adjusting for the aforementioned prognostic factors. NACT, neoadjuvant chemotherapy.
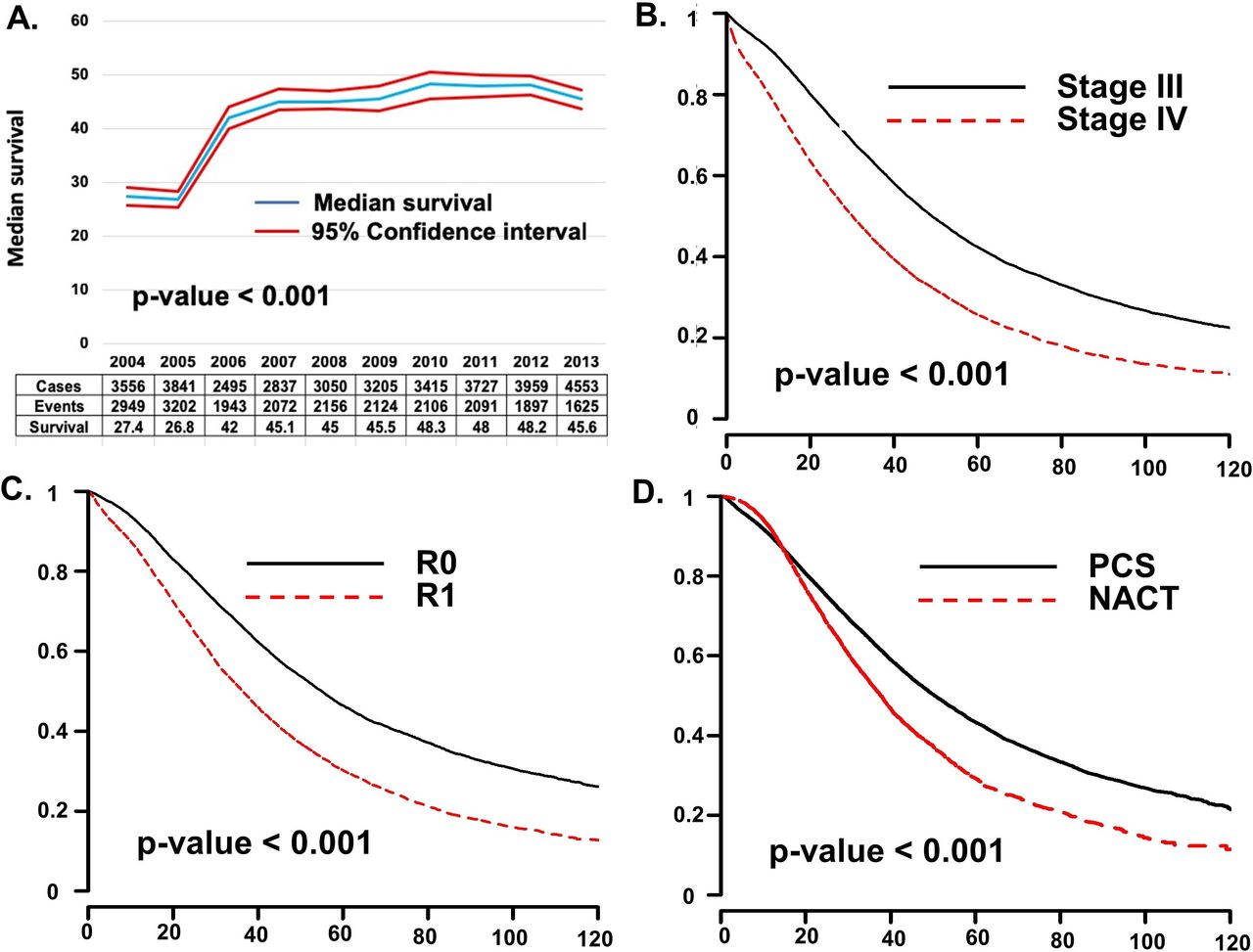
The multivariate survival results were unchanged after performing a propensity score. Only the effect of covariates and the significance level changed due to decreased sample size from the matching process, with a total of 2980 matched patients for each treatment (see online supplementary Figure 1 for specific comparisons). Figure 3 summarizes survival analyses of several of the covariates introduced in the analyses: year of treatment (Figure 3A), FIGO stage, (Figure 3B), residual disease (Figure 3C), and type of treatment (Figure 3D).

Survival has increased over time, and is increased based on lower stage of disease, the absence of gross residual disease, and with upfront primary cytoreductive surgery. Figure 3A stratifies survival based on year of treatment. The Kaplan–Meier curves in Figures 3B–3D look at survival based on stage (3B), presence or absence of residual disease (3C), and modality of upfront treatment (3D). NACT, neoadjuvant chemotherapy; PCS, primary cytoreductive surgery.
Stratified Survival Analysis
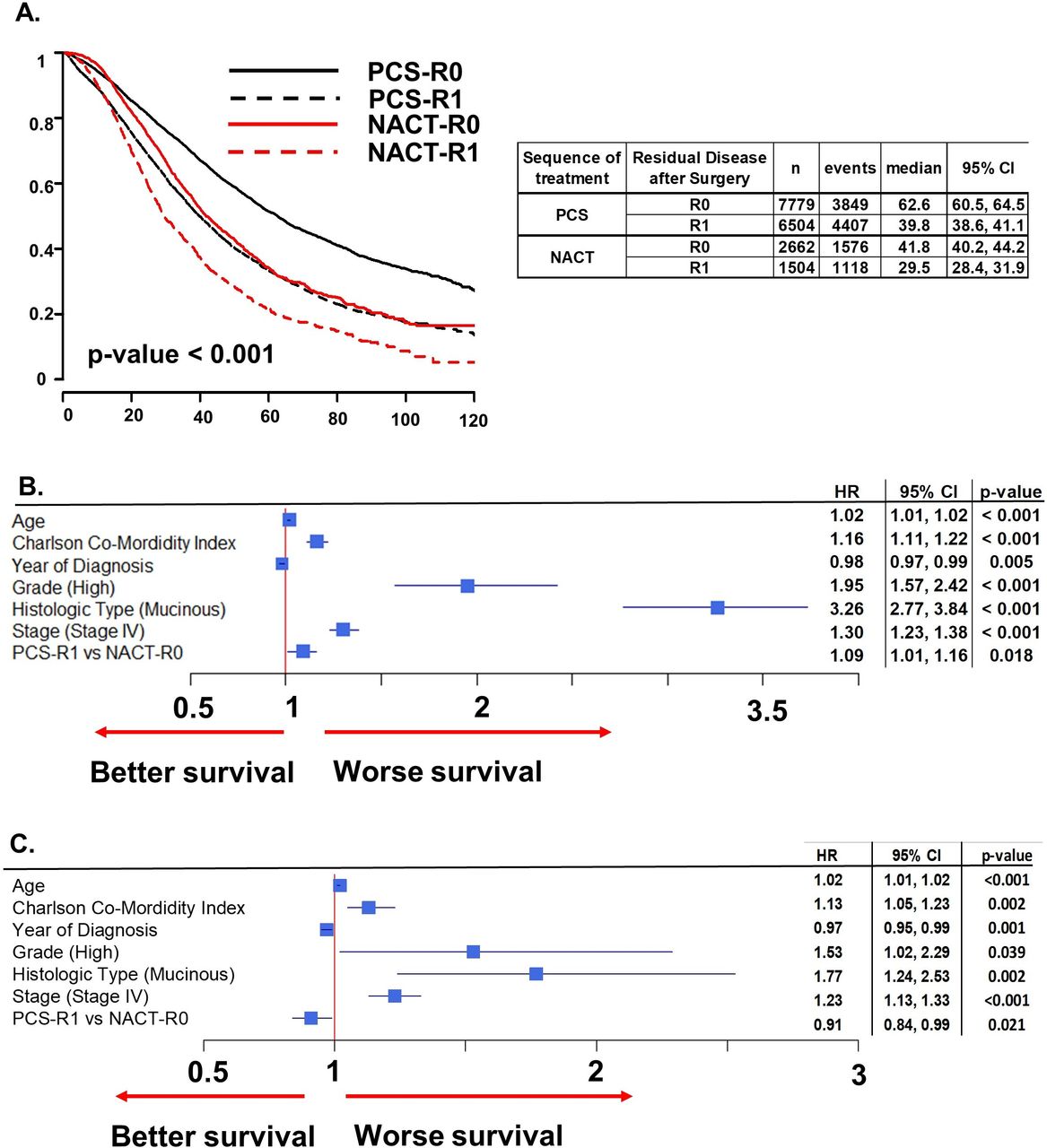
When stratifying survival of type of treatment by residual disease after surgery, patients that underwent primary cytoreductive surgery and were cytoreduced to R0 (primary cytoreductive surgery-R0) had the longest survival (62.6 months, 95% CI 60.5 to 64.5) (Figure 4A). Conversely, patients that underwent neoadjuvant chemotherapy and had macroscopic disease after surgery (neoadjuvant chemotherapy-R1) had the poorest survival. Neoadjuvant chemotherapy patients with R1 disease had worst median survival (29.5 months, 95% CI 28.4 to 31.9). Those patients that underwent primary cytoreductive surgery with macroscopic residual disease (surgery-R1) and those that underwent neoadjuvant chemotherapy without visible disease after surgery (chemotherapy-R0) had survival curves that overlap (Figure 4A).

Primary cytoreductive surgery-R0 patients have improved survival of all treatment groups and there are no clinically relevant differences in survival between primary cytoreductive surgery-R1 and neoadjuvant chemotherapy-R0. Patients are stratified by both presence of residual disease and modality of primary treatment in the Kaplan–Meier curves in Figure 4A. The forest plot (Figure 4B) demonstrates factors leading to decreased survival, including age, co-morbidities, stage, grade, mucinous type, presence of residual disease, and modality of primary treatment. Conversely, mortality for epithelial ovarian cancer improved by year of diagnosis, being the highest in 2005 and lowest in 2012. The forest plot (Figure 4C) of the multivariate analysis, after propensity score matching for all significant covariates affecting the outcome, demonstrates factors leading to worse survival including age, co-morbidities, stage, grade, mucinous type, and presence of residual disease. In this analysis, primary surgery with R1 residual disease and year of diagnosis have better survival. NACT, neoadjuvant chemotherapy; PCS, primary cytoreductive surgery.
In the Cox multivariate analysis, after adjusting for age, stage, grade, mucinous histology, year of diagnosis, and co-morbidities, survival for primary cytoreductive surgery-R1 patients had a small difference in median survival compared with neoadjuvant chemotherapy-R0 patients, with a HR of 1.09 (95% CI 1.01 to 1.01, p=0.02, Figure 4B). Median survival was 39.8 months for surgery-R1 patients compared with 41.8 months for chemotherapy-R0 patients. When this analysis was performed with propensity score matching for covariates affecting both treatments, surgery-R1 patients had better survival than chemotherapy-R0, with a HR of 0.91 (95% CI 0.84 to 0.99, p=0.02, Figure 4C).
Mortality Analysis
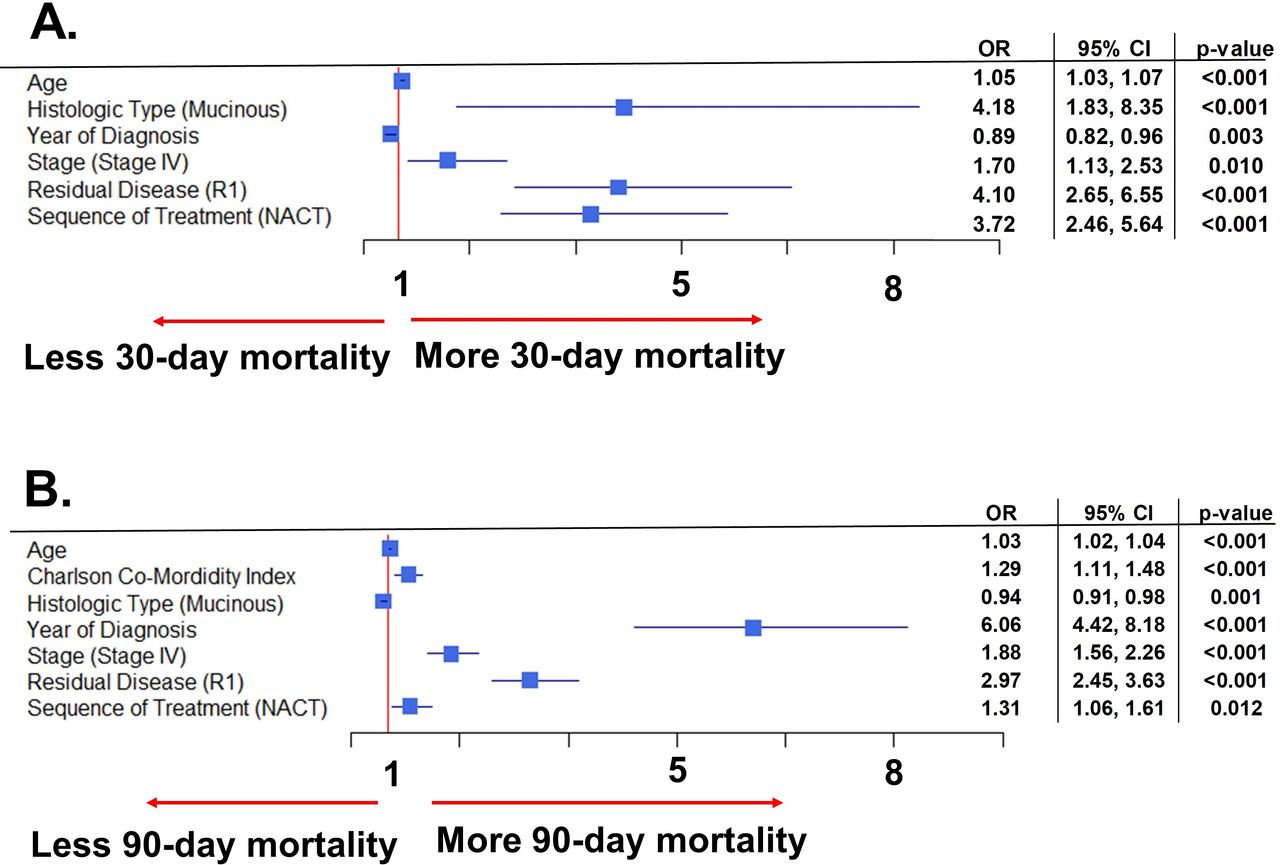
The 30-day mortality after surgery was increased significantly in those patients treated with neoadjuvant chemotherapy (1% vs 0.3% in the primary cytoreductive surgery group). The mortality rate was 3.7 times (95% CI 2.46 to 5.64) higher compared with primary cytoreductive surgery, regardless of age, stage, histologic type, year of diagnosis, and presence of residual disease (Figure 5A). This increased mortality was also seen 90 days after surgery, with a HR of 1.31 (95% CI 1.06 to 1.61), and after adjusting for all significant covariates in the multivariate analysis (Figure 5B).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The 30-day post-operative mortality is increased with neoadjuvant chemotherapy, while there is no difference in survival after 90 days, regardless of primary treatment. Figure 5A looks at stratifying 30-day post-operative mortality by factors including age, year of diagnosis, stage, presence of residual disease, and modality of primary treatment. Figure 5B uses the same factors, plus co-morbidities, to evaluate the effect on 90-day post-operative mortality. NACT, neoadjuvant chemotherapy; PCS, primary cytoreductive surgery.
When we replicated the analysis excluding older patients (>75 years old), any co-morbidities (CCI>0), low-grade cancers, mucinous subtypes, and adjusted for other covariates, mortality at 30 days was still different between patients undergoing primary surgery and those receiving neoadjuvant chemotherapy (0.2% vs 0.8%, respectively, p<0.001). For the 90-day mortality, we did not see any differences when excluding high-risk patients. There were few patients available for the propensity score matching and analysis of mortality (44 for each group at 30 days and 225 at 90 days), with not enough power to assess differences.
Discussion
In this retrospective, quasi-population-based study of the NCDB, patients with epithelial ovarian cancer that underwent primary cytoreductive surgery had better overall survival than patients that underwent neoadjuvant chemotherapy, even after adjusting for significant covariates. These results hold true after two validation studies: one excluding patients at risk of failing treatment, the other after propensity score matching of both treatment groups. Moreover, there were minimal survival differences in patients that underwent primary cytoreductive surgery and had residual disease (surgery-R1) compared with those receiving neoadjuvant chemotherapy with no residual disease after interval cytoreduction (chemotherapy-R0). Those differences depend on the analysis performed (with or without propensity score matching), with the 95% CIs very close to 1 in both scenarios. In addition, there were differences in 30-day and 90-day surgical mortality between treatment groups, showing benefit of primary cytoreductive surgery when compared with interval debulking post-neoadjuvant chemotherapy.
In a recent review by the authors of the first phase III neoadjuvant chemotherapy clinical trial, they recognize the poor overall survival of all patients in that trial, regardless of primary treatment.8 They hypothesized the study could be biased because centers potentially enrolled patients with poorer prognostic factors and because there were “remarkable” differences between participating centers.8 They argued that the latter may have been a result of lack of qualification process for participating centers.8 Now with new studies that increased surgical effort, there is still no difference in survival between primary cytoreductive surgery and neoadjuvant chemotherapy.3 More recently, the TRUST (Trial of Radical Upfront Surgical Therapy in advanced ovarian cancer (ENGOT ov33/AGO-OVAR OP7)) trial recruited patients for an international, multicenter, randomized trial which aims to determine optimal timing of surgery for treatment of advanced ovarian cancer.9 The trial is designed to assess overall survival and also control for surgical quality.9
Previous studies have suggested using neoadjuvant chemotherapy in cases where optimal or complete cytoreduction is not possible due to disease burden. It is often difficult to determine whether or not optimal cytoreduction is possible until abdominal exploration occurs. Other groups have designed selection methods to optimize surgical outcomes by focusing on pre-operative and peri-operative care.10 11 This model only assesses morbidity and mortality from primary cytoreductive surgery, without taking into consideration tumor biology, spread of disease, or oncologic outcomes.11 Others have studied how tumor biology may influence successful or optimal primary cytoreductive surgery.12 However, this model was never validated externally or prospectively. Pre-operative imaging has also been used to predict surgical outcomes, but these studies were not able to create internally validated prediction models. The predictive performance of any of these models was not validated externally.13 Exceptions to our proposal of primary cytoreductive surgery regardless of tumor burden would include patients with unresectable chest, brain, liver, or bone metastasis. It is also important to note that neoadjuvant chemotherapy is often utilized to compensate for inferior surgical quality. Although we recommend primary cytoreductive surgery for improved survival based on the results of this study, only those extensively trained in complex debulking surgery should perform these cases, in order to maximize patient benefit and minimize complications.
Finally, there have been efforts to predict optimal surgical outcomes by an initial laparoscopic examination of the abdominal cavity.14 15 A recent Cochrane systematic review could not firmly conclude whether laparoscopy before initial primary cytoreductive surgery could predict which patients would have optimal outcomes.14 Moreover, when laparoscopy is used to evaluate optimal primary cytoreductive surgery, approximately 40% of patients will not be offered this procedure as initial treatment.15 Therefore, to date, there are no validated methods to predict optimal primary cytoreductive surgery or surgical outcomes. Neoadjuvant chemotherapy is known to produce tissue changes, such as inflammation and fibrosis, which often makes interval cytoreduction more challenging than primary cytoreduction.16 A surgeon’s visual estimation of tumor burden has been shown to be more sensitive at determining histopathologically-confirmed malignancy in the abdomen at the time of primary cytoreductive surgery versus at interval cytoreduction.16 Our analysis shows no clinically-relevant differences in survival between those completely cytoreduced after neoadjuvant chemotherapy and those primarily cytoreduced but with residual disease left after surgery.
Both the CHORUS and EORTC studies demonstrated that post-operative mortality (within 28 days of surgery) was higher in the primary cytoreductive surgery group compared with neoadjuvant chemotherapy.1 2 Similarly, retrospective studies have also shown a decrease in post-operative mortality when primary treatment modality is neoadjuvant chemotherapy versus primary cytoreductive surgery.17 18 Our study reveals that post-operative mortality was at least three times higher in the neoadjuvant chemotherapy group at 30 days. Even after excluding elderly and frail patients, we still saw an increased mortality at 30 days with those undergoing neoadjuvant chemotherapy.
Strengths of our study are that the data are from a comprehensive, national cancer database. The sample size is robust, and we were able to stratify patients by baseline characteristics, including primary treatment modality and presence of residual disease. We were able to replicate the analysis after eliminating those patients at risk of failing chemotherapy and after propensity score matching to account for covariates biases, and the results were validated. Weaknesses include that this is a retrospective study, and disease burden cannot be quantified. There is lack of information on the reason for choice of primary treatment, the composition of the multi-agent chemotherapy, and the administration of maintenance treatment. Furthermore, we did not distinguish between patients treated at high- vs low-volume hospitals, which could affect the choice of primary treatment and surgical outcome. Finally, although we could not account for the increase of neoadjuvant chemotherapy utilization due to changes in clinical practices, we did account for the year of diagnosis and treatment as a proxy.
In conclusion, based on the findings of this study, we showed that primary cytoreductive surgery may be offered by expert surgeons to the majority of patients with advanced epithelial ovarian cancer, with the exceptions noted above. This is reinforced by the observation that patients with residual disease at the end of a primary cytoreduction, and those with no gross residual disease after an interval debulking, have minimal to no differences in overall survival. While neoadjuvant chemotherapy is within the standard of care, based on our results, patients that undergo neoadjuvant chemotherapy and interval debulking surgery, and are left with residual disease, have the poorest outcome. In order to minimize patients with poor prognosis, we recommend reducing neoadjuvant chemotherapy to a minimum, and indicate it primarily for those patients not medically fit for primary surgery or with unresectable metastasis to the bone, chest, liver, and brain, as well as those with diffuse bowel serosal and mesenteric disease.
Supplemental material
References
Footnotes
Contributors YAL and JGB made significant contributions to the conception, design, and/or acquisition of data, and/or analysis and interpretation of data. JGB, HDR, MEM, AN, ED, DPB, and MJG participated in drafting the article or revising it for important intellectual content and gave final approval of the version to be submitted.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. The data from our study were extracted from the National Cancer Database repository with permission. The data are available upon request to Jesus Gonzalez Bosquet at jesus-gonzalezbosquet@uiowa.edu.