Article Text

Abstract
Introduction As sentinel lymph node biopsy is evolving to an accepted standard of care, clinicians are being faced with more frequent cases of small volume nodal metastatic disease. The objective of this study is to describe the management and to measure the effect on recurrence rates of nodal micrometastasis and isolated tumor cells in patients with early stage cervical cancer at two high-volume centers.
Methods We conducted a review of prospectively collected patients with surgically treated cervical cancer who were found to have micrometastasis or isolated tumor cells on ultrastaging of the sentinel lymph node. Our practice is to follow patients for ≥5 years post-operatively either at our center or another cancer center closer to home.
Results Nineteen patients with small volume nodal disease were identified between 2006 and 2018. Median follow-up was 62 months. Ten (53%) had nodal micrometastatic disease, while nine (47%) had isolated tumor cells detected in the sentinel lymph node. Seven patients (37%) underwent completion pelvic lymphadenectomy and four of them also had para-aortic lymphadenectomy; there were no positive non-sentinel lymph nodes. The majority (74%) received adjuvant treatment, mostly driven by tumor factors. We observed two recurrences. Recurrence-free survival was comparable with historical cohorts of node negative patients, and adjuvant treatment did not seem to impact the recurrence rate (p=0.5).
Conclusion Given the uncertainties around the prognostic significance of small volume nodal disease in cervical cancer, a large proportion of patients receive adjuvant treatment. We found no positive non-sentinel lymph nodes, suggesting that pelvic lymphadenectomy or para-aortic lymphadenectomy may not be of benefit in patients diagnosed with small volume nodal metastases. Recurrence-free survival in this group did not seem to be affected. However, given the small numbers of patients and lack of level 1 evidence, decisions should be individualized in accordance with patient preferences and tumor factors.
- cervical cancer
- neoplasm micrometastasis
- sentinel lymph node
Statistics from Altmetric.com
HIGHLIGHTS
Recurrence-free survival in patients with early cervical cancer and small volume nodal metastases is comparable to that in node negative patients.
Pelvic and para-aortic lymphadenectomy may not be necessary due to the low incidence of positive non-sentinel nodes.
Most patients who receive adjuvant treatment have intermediate or high-risk features that primarily drive that decision.
Introduction
The presence of lymph node metastasis is an important negative prognostic factor in early cervical cancer.1 2 The significant survival benefit of adjuvant chemoradiation in patients with high-risk disease features, including lymph node metastasis, was shown in the GOG (Gynecologic Oncology Group) 109 study, where patients were randomized to receive either pelvic radiation alone or radiation plus concurrent chemotherapy.1 Since that study, the reliability of sentinel lymph node biopsy to accurately reflect a patient’s lymph node status has been confirmed in prospective multicenter studies,3 4 large retrospective studies,5 and a meta-analysis.6 A large retrospective study from our institution has shown that, compared with a complete pelvic lymphadenectomy, sentinel lymph node biopsy is associated with similar recurrence-free survival and a decreased rate of peri-operative complications.7 In addition, sentinel lymph node biopsy has been shown to increase the detection of lymph node metastasis by identifying sentinel lymph nodes outside the routine lymphadenectomy areas8 and by detecting the presence of small volume nodal disease (micrometastasis defined as 0.2–2 mm and isolated tumor cells defined as <0.2 mm) in an additional 15% of patients.5
As sentinel lymph node biopsy is becoming an accepted standard of care, we are faced with the conundrum of what the prognosis and appropriate management is for patients with early cervical cancer and small volume metastasis in the sentinel lymph node. A recent prospective study where patients underwent sentinel lymph node biopsy followed by confirmatory pelvic lymphadenectomy showed no impact on recurrence-free survival at 36 months; 12 of the 13 patients with small volume nodal disease did not receive any adjuvant treatment.9 Previous retrospective studies5 10–15 have included patients who had sentinel lymph node biopsy followed by pelvic lymphadenectomy, and have had conflicting results. Nodal micrometastases have been associated with decreased overall survival and increased recurrence in patients with cervical cancer in some studies5 10 13–15 but not in others.9 11 Patients with nodal sub-micrometastases in breast cancer (≤0.2 mm) and in melanoma (≤0.1 mm) have the same prognosis as node negative patients.16–19 However, in contrast to patients with cervical cancer, decisions regarding adjuvant treatment in breast cancer and melanoma are made primarily on characteristics of the primary tumor. Here we present a large case series from two institutions of patients with early cervical cancer and small volume nodal metastasis in the sentinel lymph node.
Methods
Patient selection
We conducted a retrospective observational study of data collected prospectively in patients with surgically treated early cervical cancer. Approval from the institutional ethics review boards and a data sharing agreement were obtained from our two high-volume centers. Patients treated by members of our division from 2006 to 2018 with a diagnosis of cervical cancer, International Federation of Gynecology and Obstetrics (FIGO) stages IA1–IB3, were identified. For the purposes of this publication, the updated FIGO 2018 staging system has been used. The size of the largest metastatic deposit was recorded from reviewing pathology reports, and only patients with the largest metastatic deposit <2 mm were included in this analysis. Patients who received adjuvant therapy or follow-up at a different center were contacted by telephone to ensure no recurrences were missed.
Surgical procedure and histopathology
In general, at our institutions, patients were primarily treated with a radical hysterectomy if the tumor was <4 cm in size, and primary chemoradiation for larger tumors unless fertility preservation was a consideration. Young patients with tumors >4 cm were considered for radical surgery only if the tumor was exophytic with minimal stromal involvement. Patients who desired fertility preservation were offered a cone biopsy and lymph node assessment if they met the criteria for microinvasive disease; otherwise, they were treated with a radical trachelectomy. Unless patients were treated on trial, a sentinel lymph node biopsy without confirmatory pelvic lymphadenectomy was offered to all. All patients underwent pre-operative staging computed tomography scans of the chest, abdomen, and pelvis, with or without pelvic magnetic resonance imaging, to aid in surgical planning.
The protocols for the sentinel lymph node procedure using technetium sulphur colloid or indocyanine green have been previously published independently by the two centers.20 21 On the morning of surgery, the cervix was infiltrated at 03.00 and 09.00 hours at one center, and at 12.00, 03.00, 06.00 and 09.00 hours at the other, with the technetium sulphur colloid. One center used isosulphan blue dye (Patent Blue; Bracco Diagnostics, Minneapolis, Minnesota, USA) in all patients, while the second only in cases when bilateral sentinel lymph nodes were not identified on a scintogram performed 20 min after injection. In both scenarios, 1 mL of Patent Blue was injected at the same locations on the cervix as the technetium. As of January 2015, indocyanine green replaced technetium. After dilution with sterile water to a concentration of 2.5 mg/mL, 1–2 mL indocyanine green solution was injected at 03.00 and 09.00 hours after induction of anesthesia.
Intra-operatively, sentinel lymph nodes were identified with a laparoscopic gamma probe or with a near infra-red endoscopic camera (Pinpoint, Novadaq) by scanning the pelvic and para-aortic regions. Nodes with a radioactive count at least five times the background count (technetium), blue nodes (Patent Blue), and fluorescent green nodes (indocyanine green) were labeled as sentinel lymph nodes and sent for intra-operative pathological review. This protocol has been previously published by our institutions.20 21 The sentinel lymph nodes were transected perpendicular to their long axis at 2–3 mm intervals. For intra-operative evaluation, one 5 µm section was obtained from the frozen block and stained with hematoxylin and eosin. Three additional sections were obtained from the paraffin block fixed in 10% formalin; two were stained with hematoxylin and eosin and a third with a pan cytokeratin cocktail immunohistochemistry (clone AE1/AE3, Dako).
Apart from the first 30 patients at one center and the first 39 patients at the other, during the validation period of the sentinel lymph node program, pelvic lymphadenectomy was not performed if the sentinel lymph node was reported as negative intra-operatively. When the sentinel lymph node was reported as positive intra-operatively, a pelvic lymphadenectomy and para-aortic lymph node dissection on the ipsilateral side of the positive node were completed. This was performed as per the usual practice at our institution, with the purpose of guiding adjuvant treatment decisions in this population. When the sentinel lymph node was not identified, an ipsilateral pelvic lymphadenectomy was completed.
Results
Patient characteristics
A total of 19 patients with early cervical cancer and small volume nodal metastatic disease were identified. Median follow-up was 62 months (range 13–94). Median age was 34 years (range 26–60). Most patients had squamous histology (10/19, 53%), with 26% (5/19) adenocarcinoma, and 21% (4/19) adenosquamous histology. The majority of patients had FIGO stage IB1 (37%, 7/19) and IB2 (42%, 8/19). Two patients (11%) had microinvasive disease on final pathology (FIGO stage IA1) and one patient had FIGO stage IA2 disease (5%). One patient (5%) had a large >4 cm tumor, FIGO stage IB3 (Table 1).
Patient and treatment characteristics
Surgical treatment
Patients with stage IB disease were primarily treated with radical surgery (58%, 11/19 laparoscopic hysterectomy and 20%, 4/19 laparoscopic-assisted vaginal trachelectomy), with the exception of two patients (11%) who were treated with a repeat cone biopsy and lymph node assessment. The two patients (11%) who had FIGO stage IA1 microinvasive disease were treated with a simple laparoscopic hysterectomy and assessment of lymph nodes. Sentinel lymph node assessment was performed in all cases and bilateral sentinel lymph nodes were identified in all.
Histology
Median tumor size was 18 mm (rage 1–44 mm) and the median depth of invasion was 8.8 mm (range 0.8–20 mm). Most patients had positive lymphovascular space invasion (15/19, 79%), and a significant proportion (8/19, 42%) met intermediate-risk criteria post-operatively.22
On final pathological ultrastaging, 10 patients (53%) had nodal micrometastatic disease while nine patients (47%) had isolated tumor cells detected in the sentinel lymph node. Intra-operatively, only four (40%) of the 10 patients with micrometastatic nodal disease were identified, and none of the patients with isolated tumor cells. The four patients who were identified during the surgery had completion ipsilateral pelvic and para-aortic lymphadenectomy. None of the non-sentinel lymph nodes were positive. The total mean number of lymph nodes removed per patient was 24. An additional three patients (18%, 3/19) were treated during the validation period and underwent completion bilateral pelvic lymphadenectomy, although the sentinel lymph nodes were reported as negative intra-operatively. In these seven patients who had pelvic lymphadenectomy with or without para-aortic lymphadenectomy, the total mean number of lymph nodes removed per patient was 17 and there were no positive non-sentinel lymph nodes. The remaining 12 patients (63%) had sentinel lymph node biopsy only without further lymphadenectomy. Although 3/9 patients with nodal micrometastasis had multiple positive nodes, these were all micrometastases and there were no positive non-sentinel nodes.
Adjuvant treatment
All eight patients (8/19, 42%) who met the intermediate-risk criteria received adjuvant radiation to the pelvis with concurrent cisplatin. In addition, two of these eight patients had a positive vaginal margin and received a brachytherapy boost. Eleven patients did not meet the intermediate-risk criteria; treatment of these patients was variable, with the majority (5/11, 46%) undergoing observation alone, while others were treated with chemotherapy (3/11, 27%), chemotherapy and radiation (2/11, 18%), or radiation alone (1/11, 9%). There was no statistically significant difference between recurrence-free survival in patients who were treated based on intermediate-risk criteria, those who were treated in the absence of intermediate-risk criteria, or those who did not receive any adjuvant therapy (Figure 1, p=0.5).
Recurrence-free survival (RFS) in patients who received adjuvant treatment versus patients who did not receive adjuvant treatment by risk stratification.
Recurrences
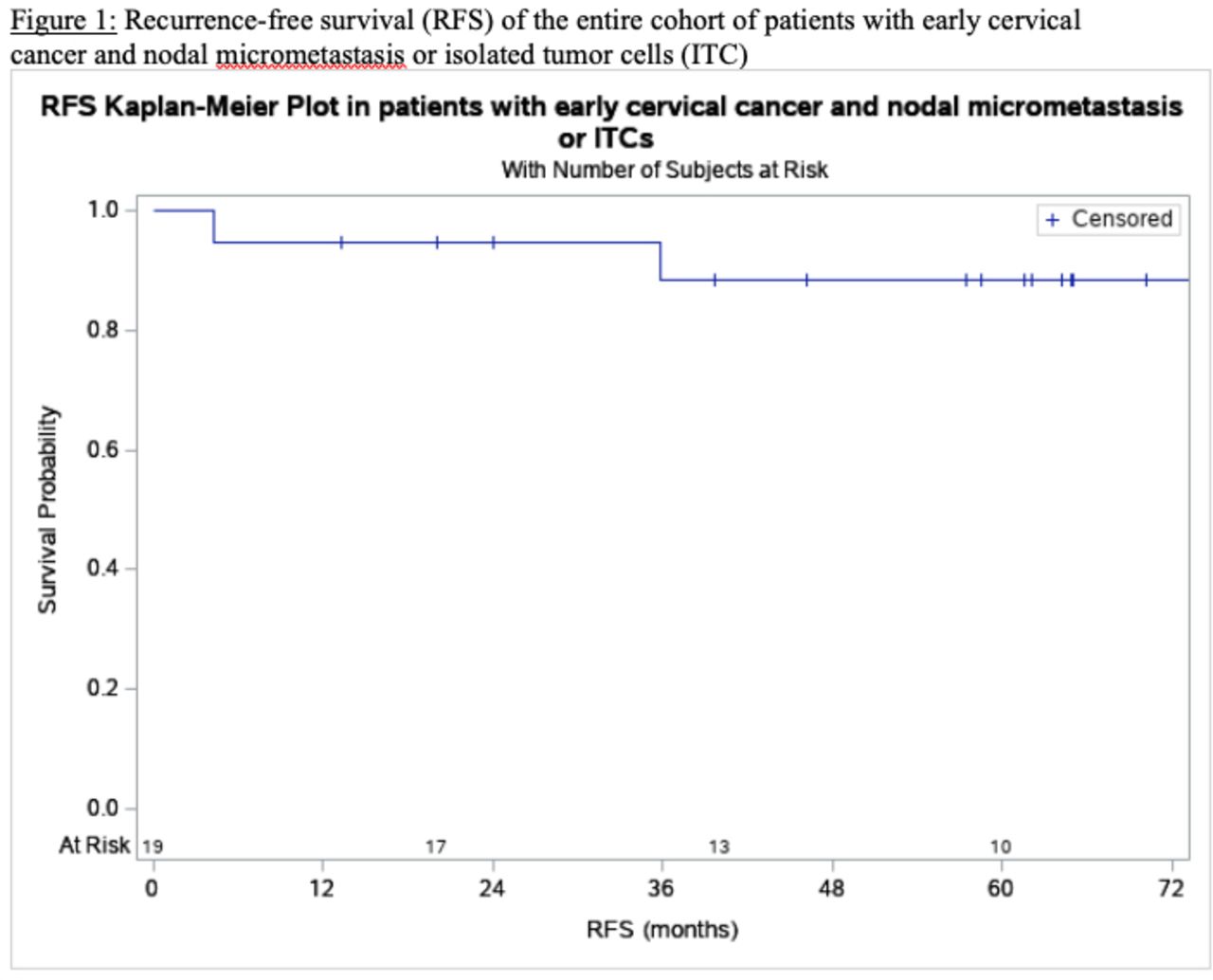
Two patients experienced a recurrence during the follow-up period, one early recurrence at 7 months and one late recurrence at 36 months. The 5-year recurrence-free survival was 89.5% (Figure 2). The patient who had the late recurrence of her FIGO stage IB2 poorly differentiated adenosquamous carcinoma had received adjuvant treatment with concurrent pelvic radiation and chemotherapy, followed by brachytherapy. This was done on the basis of high-risk criteria, including a positive vaginal margin, one positive parametrial lymph node, outer third cervical stromal invasion, and lymphovascular space invasion, in addition to having micrometastatic nodal disease in three of the five sentinel lymph nodes removed. The recurrence was invading into the pelvic sidewall and the patient was not a candidate for pelvic exenteration. She was treated with palliative intensity-modulated radiation therapy and systemic chemotherapy, ultimately succumbing to her disease.

{kind=link}
{kind=link}
Recurrence-free survival (RFS) of the entire cohort of patients with early cervical cancer and nodal micrometastasis or isolated tumor cells (ITCs).
The second recurrence was in a patient treated with a radical trachelectomy for a stage IB2 poorly differentiated squamous cell carcinoma. Her final pathology demonstrated superficial cervical stromal invasion, focal lymphovascular space invasion, and negative resection margins, with the closest margin distally at 5 mm. She had evidence of recurrence centrally, at the vaginal vault and lower uterine segment, and was treated with completion hysterectomy followed by adjuvant chemoradiation and vaginal vault brachytherapy.
Discussion
In this case series analysis of patients with early cervical cancer and small volume nodal metastasis we found that a large proportion of these patients (42%) had intermediate-risk features which required adjuvant treatment, irrespective of their nodal status; these included deep cervical stromal invasion, tumor size and lymphovascular space invasion.22 In the follow-up of the SENTICOL1 trial,9 four out of 13 patients with micometastasis or isolated tumor cells (31%) received adjuvant treatment for positive lymphovascular space invasion or parametrial involvement. The criteria for requiring adjuvant treatment differ between our study and SENTICOL1: patients in SENTICOL1 were eligible if parametrial or vaginal invasion was detected, they had positive lymph nodes, or tumors >4 cm. In our patient cohort, a significant proportion of patients with low-risk features and small volume nodal metastasis received adjuvant treatment. Interestingly, most of our patients had lymphovascular space invasion (15/19, 79%) compared with patients in the SENTICOL study, where only the minority (2/13, 15%) of patients with nodal micrometastasis or isolated tumor cells had lymphovascular space invasion.
In contrast to previous studies, our patients did not undergo confirmatory pelvic lymphadenectomy if the sentinel lymph node was negative on frozen section (with the exception of three patients who were treated during the sentinel lymph node validation period). The seven patients who underwent completion lymph node dissection (three bilateral pelvic lymphadenectomy and four ipsilateral pelvic and para-aortic lymphadenectomy) did not have any positive non-sentinel lymph nodes. This is similar to the results from the SENTICOL trial,3 where there were no positive non-sentinel lymph nodes in the patients with small volume nodal metastasis; of note, out of 139 patients, there was only one true false negative. The large retrospective study by Cibula and colleagues,5 which showed decreased survival at 5 years for patients with micrometastasis in the sentinel lymph node, did not comment on the rate of non-sentinel lymph node metastasis in this population. Given these observations, a complete ipsilateral pelvic and para-aortic lymphadenectomy may not be necessary in patients with micrometastasis or isolated tumor cells in the sentinel lymph node. However, given the uncertainty around the need for adjuvant treatment even in the absence of other intermediate- or high-risk features, having complete surgical staging may aid decision-making in favor of observation in order to reduce treatment-related morbidity.
We recorded two recurrences in our cohort, for a 5-year recurrence-free survival of 89.5%. It should be mentioned that one of the two recurrences had multiple high-risk features including a positive vaginal margin, positive parametria, positive lymphovascular space invasion, and deep stroma invasion in addition to three sentinel lymph nodes positive for micrometastasis, and recurred despite receiving adjuvant chemoradiation and brachytherapy boost. Moreover, the second recurrence occurred centrally in the pelvis and is unlikely to be due to unresected or untreated nodal disease. This survival rate is similar to the recurrence-free survival reported by the SENTICOL authors (91.6% and 90.4%, respectively, in patients with positive and negative lymph nodes) and to our own institution’s 5-year recurrence-free survival in node negative patients of 92%.7 Historically, the 5-year survival rate for women with stage IB cervical cancer and negative lymph nodes has been reported to be between 88% and 96%.23–25 As far as the impact of adjuvant treatment on outcomes, it is difficult to draw a conclusion from our cohort due to the small numbers as well as differences in prognostic risk factors between the two groups. There was no statistically significant difference in recurrence-free survival in patients who received or did not receive adjuvant treatment when stratified based on the presence or absence of intermediate-risk criteria (Figure 1, p=0.5).
Our study is the first to describe outcomes in patients with early cervical cancer and small volume nodal metastatic disease at an institution where sentinel lymph node biopsy without confirmatory lymphadenectomy has been the standard of care for many years. Our results suggest that pelvic and para-aortic lymphadenectomy may be omitted in these patients. Adjuvant treatment was given mostly based on tumor factors, but also due to uncertainty around the prognostic significance of small volume nodal metastasis. Recurrence-free survival was similar to historical cohorts of node negative patients. Limitations include the small number of patients and heterogenous population with respect to FIGO stage, surgical management, and criteria for adjuvant treatment. Due to the decreasing incidence of cervical cancer in our communities and the low incidence of small volume nodal metastatic disease, large prospective or randomized trials powered to answer this question are not likely to be feasible. Thus, future practice will be dictated by prospective cohort or retrospective studies like ours. Until then, individualized clinical decisions should be made, taking into account all relevant patient and tumor factors as well as patient preferences.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Editor's note This paper will feature in a special issue on sentinel lymph node mapping in 2020.
Contributors AN performed data collection, analysis and wrote the manuscript. LTG and SEF were involved in the surgical treatment of patients and manuscript editing. AC is the senior author, involved in the surgical treatment of patients and also responsible for the study idea, and for supervising data collection, analysis, and manuscript editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Sunnybrook Health Sciences Centre, Toronto, ON, Canada.
Provenance and peer review Commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. Deidentified participant data is securely stored by the first and the corresponding authors. Available upon reasonable request.