Article Text

Abstract
Objective Two randomized phase III trials demonstrated the efficacy and safety of combining bevacizumab with front-line carboplatin/paclitaxel for advanced ovarian cancer. The OSCAR (NCT01863693) study assessed the impact of front-line bevacizumab-containing therapy on safety and oncologic outcomes in patients with advanced ovarian cancer in the UK.
Methods Between May 2013 and April 2015, patients with high-risk stage IIIB–IV advanced ovarian cancer received bevacizumab (7.5 or 15 mg/kg every 3 weeks, typically for ≤12 months, per UK clinical practice) combined with front-line chemotherapy, with bevacizumab continued as maintenance therapy. Co-primary endpoints were progression-free survival and safety (NCI-CTCAE v4.0). Patients were evaluated per standard practice/physician’s discretion.
Results A total of 299 patients received bevacizumab-containing therapy. The median age was 64 years (range 31–83); 80 patients (27%) were aged ≥70 years. Surgical interventions were primary debulking in 21%, interval debulking in 36%, and none in 43%. Most patients (93%) received bevacizumab 7.5 mg/kg with carboplatin/paclitaxel. Median duration of bevacizumab was 10.5 months(range <0.1–41.4); bevacizumab and chemotherapy were given in combination for a median of three cycles (range 1–10). Median progression-free survival was 15.4 (95% CI 14.5 to 16.9) months. Subgroup analyses according to prior surgery showed median progression-free survival of 20.8, 16.1, and 13.6 months in patients with primary debulking, interval debulking, and no surgery, respectively. Median progression-free survival was 16.1 vs 14.8 months in patients aged <70 versus ≥70 years, respectively. The 1-year overall survival rate was 94%. Grade 3/4 adverse events occurred in 54% of patients, the most common being hypertension (16%) and neutropenia (5%). Thirty-five patients (12%) discontinued bevacizumab for toxicity (most often for proteinuria (2%)).
Conclusions Median progression-free survival in this study was similar to that in the high-risk subgroup of the ICON7 phase III trial. Median progression-free survival was shortest in patients who did not undergo surgery.
- ovarian cancer
- surgery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, an indication of whether changes were made, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
HIGHLIGHTS
The OSCAR study evaluated front-line bevacizumab for advanced ovarian cancer in the UK.
Median progression-free survival was 15.4 months and toxicity was predictable and manageable.
Median progression-free survival was shortest in patients who did not undergo surgery.
Background
Angiogenesis plays a key role in ovarian cancer progression and represents an important therapeutic target. Several anti-angiogenic agents have been evaluated in ovarian cancer; of these, bevacizumab is the most extensively studied.1 Bevacizumab is a humanized monoclonal antibody that targets vascular endothelial growth factor. It is approved in combination with chemotherapy in newly diagnosed and recurrent ovarian cancer by the US Food and Drug Administration, the European Medicines Agency, and in many other countries worldwide.
The efficacy and safety of front-line bevacizumab, carboplatin, and paclitaxel were demonstrated in two randomized phase III trials, the Gynecologic Oncology Group (GOG)-0218 and the International Collaboration on Ovarian Neoplasms (ICON) 7.2 3 Adding bevacizumab to carboplatin and paclitaxel chemotherapy significantly improved progression-free survival (primary endpoint) in both trials, although no significant impact on overall survival was detectable in the overall population of either trial. Nevertheless, in the subgroup of patients classified as ‘high risk’ in ICON7, overall survival was significantly improved with bevacizumab,4 leading to preferential use of bevacizumab in this population in some countries and regions.
Although such trials provide clear evidence of efficacy, typically randomized phase III trials have strict eligibility criteria and the populations are often not fully representative of patients presenting in routine oncology practice.5 It is important to assess whether outcomes observed in rigorously conducted randomized phase III trials can be replicated in the ‘real-world’ setting, where patients typically have more comorbidities and are less fit. In England, bevacizumab combined with chemotherapy is reimbursed in patients with stage IIIB–IV (high-risk) ovarian cancer, based on the significantly improved progression-free and overall survival in the ‘high-risk’ subgroup (stage III with ≥1 cm residual disease, any stage IV, or no surgery) of the ICON7 trial.3 4 The OSCAR study (An Observational Study of Avastin (Bevacizumab) in Combination With Chemotherapy as First-Line Treatment in Patients With Advanced Ovarian Cancer, NCT01863693; sponsored by Roche Products Ltd) aimed to determine the safety and efficacy of bevacizumab-containing therapy in this patient population in the UK.
Methods
This single-arm non-interventional study was conducted in accordance with the guidelines for Good Pharmacoepidemiology Practices and Good Clinical Practices, in full conformance with the principles of the Declaration of Helsinki and the current Guideline for Good Clinical Practice ICH Tripartite, and in compliance with the current European Union Clinical Trial Directive (2001/20/EC), as well as key recommendations of the UK Association of the British Pharmaceutical Industry guidance. The protocol and all study-related materials were approved by the South-East Coast, Brighton and Sussex Ethics Committee (12/LO/1680). All patients provided written informed consent. There was no patient or public involvement in the trial design.
Patients aged ≥18 years with high-risk stage IIIB–IV advanced ovarian cancer were eligible provided they had no contraindications to bevacizumab and that warnings and precautions for use as specified in the Summary of Product Characteristics6 were considered. Patients received bevacizumab (7.5 or 15 mg/kg every 3 weeks typically for up to 12 months, according to UK clinical practice and the ICON7 trial3) combined with standard front-line chemotherapy, and then continued as single-agent maintenance therapy. The choice of chemotherapy regimen was at the treating investigator’s discretion. Patients were evaluated according to standard practice or at the physician’s discretion during bevacizumab treatment (typically every 2–3 months according to UK practice), with an end-of-study assessment 12 months after the last bevacizumab dose. Patients were enrolled between May 2013 and April 2015.
The co-primary objectives were to characterize the safety profile of bevacizumab (assessed using National Cancer Institute Common Terminology Criteria for Adverse Events, version 4.0) in UK routine clinical practice, and to estimate progression-free survival. Secondary endpoints included overall survival, objective response rate, treatment regimen administered, and quality of life (EuroQol 5-Dimensions questionnaire, European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire core and ovarian cancer modules). Participation in quality of life assessment was optional.
There were no predefined hypotheses regarding the primary and secondary objectives of the study. The sample size was determined based on practical considerations rather than any formal hypothesis testing. Progression-free survival was defined as the interval between first dose of front-line therapy until documented disease progression. Overall survival was defined as the interval between first dose of front-line therapy until death from any cause. Objective response rate was assessed locally by investigators and defined as the proportion of patients with complete or partial response as best response. Subgroup analyses of safety and efficacy according to age (<70 vs ≥70 years) were performed.
Results
A total of 299 patients from 29 centers in England and Wales received bevacizumab-containing therapy. The median age was 64 years (range 31–83). Eighty patients (27%) were aged ≥70 years, including nine (3%) ≥80 years. Baseline characteristics and medical history are shown in Table 1. Only 57% of patients had undergone surgery (primary debulking in 21%, interval debulking in 36%). Older patients were less likely than younger patients to undergo surgery. Consistent with the high proportion of unoperated patients, the vast majority of patients (90%) matched the Medical Research Council definition of ‘high risk’ in ICON7.
Baseline characteristics and medical history
Most patients (93%) received bevacizumab 7.5 mg/kg every 3 weeks with carboplatin and paclitaxel. Among the 11 patients who received single-agent carboplatin with bevacizumab, five were aged ≥80 years, four were 70–80 years, and two were <70 years. The median duration of bevacizumab therapy was 10.5 months(range <0.1–41.4), and was similar in subgroups of patients aged <70 versus ≥70 years. Bevacizumab was given in combination with chemotherapy for a median of three cycles (range 1–10). In 85 patients (28%), bevacizumab was administered for >12 months. Table 2 provides further details of treatment exposure. At the data cut-off date (14 May 2018), 155 patients (52%) had received further chemotherapy, most commonly carboplatin (43%), doxorubicin (31%), and paclitaxel (18%).
Treatment exposure
Almost all patients (99%) experienced at least one adverse event. The most common adverse events (any grade) were fatigue (48%), constipation (40%), nausea (38%), and hypertension (32%) (Figure 1A). Grade 3/4 adverse events occurred in 54% of patients (55% of patients aged <70 years vs 54% of those ≥70 years). The most common grade ≥3 adverse events were hypertension (16%) and neutropenia (5%). Grade 3/4 hypertension was more common in older than younger patients (20% vs 15%, respectively) but there were no other notable safety differences according to age (Figure 1B). There were seven grade 5 adverse events (deaths), including one gastrointestinal perforation (see online supplementary table S1). Two of the patients with a fatal adverse event were aged ≥70 years (one case each of bowel obstruction secondary to disease progression and aspiration pneumonia).
Supplemental material
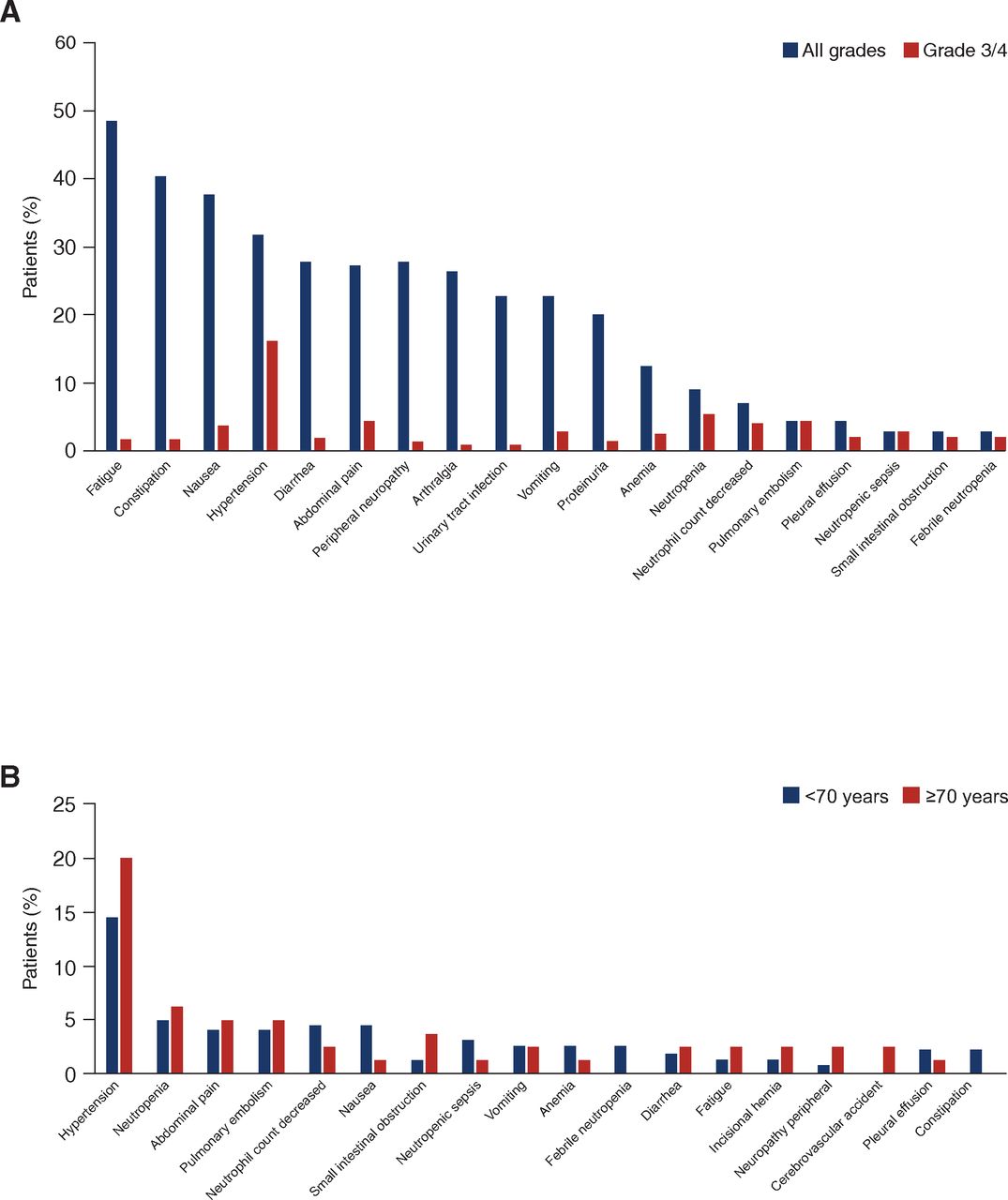
Most common adverse events: (A) overall population (any grade in ≥20% of patients and/or grade 3/4 in ≥2% of patients); (B) according to age (grade 3/4, occurring in ≥2% of patients in either subgroup).
Table 3 shows adverse events of special interest for bevacizumab overall and according to age. The most common type of bleeding event was grade 1/2 epistaxis, which occurred in 41 patients (14%). Within the category defined as thromboembolic events, the most common was pulmonary embolism, which occurred in 13 patients (4%). Thromboembolic events were more common in older than younger patients. Three grade ≥3 adverse events classified as gastrointestinal perforation comprised one case each of perforated appendicitis, enterocutaneous fistula, and gastrointestinal perforation. Of note, there were no grade ≥3 cases of congestive heart failure, cardiac disorders, posterior reversible encephalopathy syndrome, or pulmonary hypertension.
Adverse events of special interest for bevacizumab
Overall, 35 patients (12%) discontinued bevacizumab because of adverse events, most often proteinuria (2%) or pulmonary embolism (1%). Only one patient (0.3%) discontinued bevacizumab because of hypertension. Sixty-seven patients (22%) began new antihypertensive therapy after initiation of bevacizumab-containing therapy. Patients with a medical history of hypertension (n=92) were more likely than those without a medical history of hypertension (n=207) to start new antihypertensive therapy after beginning bevacizumab (33% vs 18%, respectively). This effect was particularly pronounced in patients aged ≥70 years (46% of patients with a medical history of hypertension vs 16% of patients with no history of hypertension).
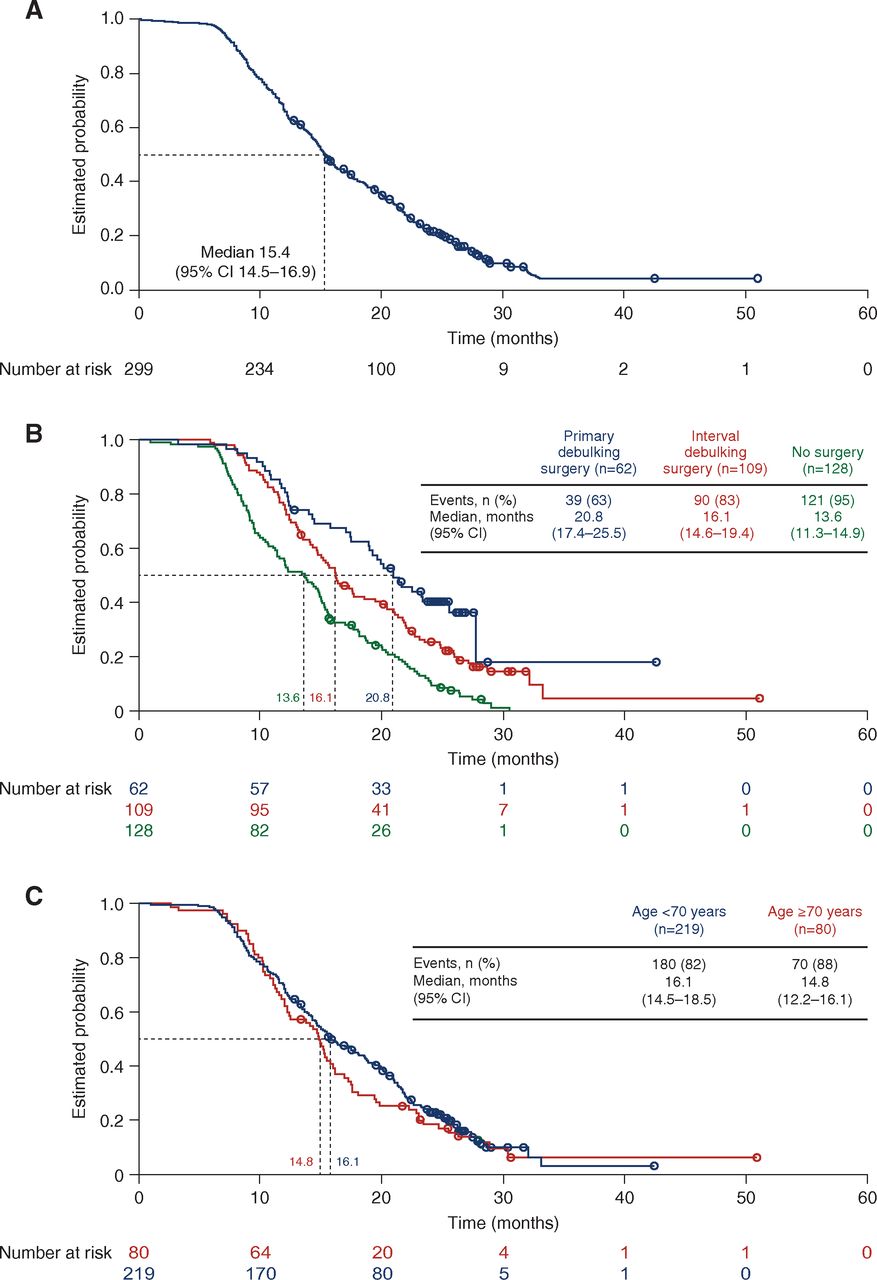
At the data cut-off date (14 May 2018), progression-free survival events had been recorded in 250 patients (84%). The majority of these represented progression detected by computed tomography (CT) or magnetic resonance imaging (189 patients, 76% of events); progression was detected by CA125 elevation alone in 35 patients (14%), CA125 elevation subsequently confirmed by CT scan in eight patients (3%), physical examination with or without CA125 elevation in nine patients (4%), and by histology of cells in the pleural effusion in one patient (<1%). Eight patients (3%) died without documented progression. Median progression-free survival was 15.4 (95% CI 14.5 to 16.9) months (Figure 2A). The 1-year progression-free survival rate was 68% (95% CI 62% to 73%). Sensitivity analyses defining progression-free survival from the date of first intervention (primary surgery or systemic therapy) instead of the protocol definition (aligned with ROSiA and ICON7, defining progression-free survival from the start of systemic therapy) showed consistent results: median progression-free survival was 15.4 (95% CI 14.6 to 17.2) months.

{kind=link}
{kind=link}
Progression-free survival: (A) overall population; (B) according to surgery; (C) according to age.
Subgroup analyses according to prior surgery (Figure 2B) showed median progression-free survival of 20.8 months(95% CI 17.4 to 25.5) in 62 patients who underwent primary debulking surgery, 16.1 months (95% CI 14.6 to 19.4) in 109 patients who underwent interval debulking surgery, and 13.6 months (95% CI 11.3 to 14.9) in 128 patients who had no surgery. In subgroup analyses according to age, median progression-free survival was 16.1 months (95% CI 14.5 to 18.5) in patients aged <70 years and 14.8 months (95% CI 12.2 to 16.1) in those ≥70 years (Figure 2C). Age showed no clear prognostic effect for progression-free survival.
The best overall response was complete response in 63 patients (21%) and partial response in 143 patients (48%), giving an objective response rate of 69% (95% CI 63% to 74%). An additional 70 patients (23%) achieved stable disease as their best response, resulting in a disease control rate of 92% (95% CI 89% to 95%). Objective response rate showed no difference according to age (69% (95% CI 63% to 75%) in patients aged <70 vs 68% (95% CI 56% to 78%) in patients aged ≥70 years). Likewise, disease control rates were almost identical (93% (95% CI 88% to 96%) vs 91% (95% CI 83% to 96%) in younger vs older patients, respectively).
At the data cut-off, 105 patients (35%) had died (9 (15%) of the 62 patients with primary debulking surgery, 41 (38%) of the 109 with interval debulking surgery, and 55 (43%) of the 128 with no surgery) (see online supplementary figure S1). The 1-year overall survival rate in the overall population was 94% (95% CI 90% to 96%). In subgroup analyses by age, 1-year overall survival rates were 94% (95% CI 90% to 97%) in patients aged <70 years versus 91% (95% CI 83% to 96%) in patients aged ≥70 years.
Supplemental material
Overall, 106 patients (35%) consented to the optional quality of life component of the study. At baseline, 87 patients (29%) completed questionnaires but there was rapid attrition, with only 66 patients (22%) completing post-baseline questionnaires before 5.5 months, and 59 (20%) between 5.5 and 9.5 months after baseline. The available data showed no relevant changes from baseline in global health status, functioning, or symptom scales, except for improvements in role and social functioning (core module) and a transient increase in peripheral neuropathy symptoms (ovarian cancer module). However, the relatively low baseline participation rate and reduced participation over time limit the conclusions that can be drawn from this dataset.
Discussion
The safety profile of front-line bevacizumab-containing therapy in this UK-based observational study is consistent with findings from the two randomized phase III trials (GOG-0218 and ICON72 3) and the single-arm ROSiA study in the front-line setting.7 Most adverse events were typical of the chemotherapy regimen. Bevacizumab therapy was associated with hypertension, thromboembolic events, and low-grade bleeding and proteinuria, as expected according to previous studies in this setting.2 3 7–9 The incidence of gastrointestinal perforation was low (1% grade ≥3). Adverse events were as expected and no new safety signals emerged, despite administration of neoadjuvant bevacizumab in 36% of patients. This finding is consistent with published safety results from the GEICO 1205 and ANTHALYA randomized phase II trials evaluating neoadjuvant bevacizumab; neither identified any particular safety concerns with neoadjuvant administration of bevacizumab.10 11 Hypertension and thromboembolic events were slightly more common in older than younger patients; this finding is consistent with the known increased risk of these events in older patients and those with pre-existing hypertension, irrespective of treatment, and is also consistent with findings from the ROSiA study.12
Median progression-free survival of 15.4 months (95% CI 14.5 to 16.9) in this predominantly high-risk patient population receiving bevacizumab for 1 year replicates median progression-free survival of 16.0 months (95% CI 14.2 to 17.8) in the high-risk subgroup of the randomized phase III ICON7 trial.3 Our results are also very similar to recently published data from a prospective observational study in Japan (n=346), in which patients with stage III/IV newly diagnosed ovarian cancer received bevacizumab with carboplatin and paclitaxel, with bevacizumab continued for 22 cycles in total.13 Median progression-free survival in the Japanese study was 16.3 months (95% CI 14.5 to 18.9) . The response rate was 78% (95% CI 67% to 86%). In addition, a single-center retrospective analysis of 60 patients treated with front-line bevacizumab after primary debulking surgery or interval debulking surgery in South West Wales, UK, demonstrated median progression-free survival of 16 months.14 Similar to OSCAR, some of these patients received bevacizumab in combination with single-agent carboplatin as they were not considered fit enough to receive combination chemotherapy.
On the other hand, median progression-free survival of 15.4 months in the OSCAR study is shorter than the median progression-free survival of 21.3 months (95% CI 20.3 to 22.5) in the German OTILIA non-interventional study9 and 25.5 months (95% CI 23.7 to 27.6) in the international single-arm ROSiA study.7 Differences in dose, treatment duration, patient prognosis, and surgery may all contribute to differences in median progression-free survival between the OSCAR, OTILIA, and ROSiA studies. For example, in OTILIA, all patients received bevacizumab at 15 mg/kg for 15 months, and in ROSiA treatment was continued for up to 24 months. Furthermore, in the ROSiA study, 23% of patients had stage I–IIIA disease, in contrast to OSCAR and OTILIA, which included only patients with stage IIIB–IV disease. Surgical differences were also apparent between countries: in the German OTILIA and global ROSiA studies, 94% (A Wegenaer, 2019, personal communication) and 95% of patients, respectively, underwent debulking surgery, and there was no visible residual disease after primary debulking surgery in 27% and 28% of patients, respectively,7 9 15 compared with 57% undergoing surgery and only 4% with no visible residual disease in the OSCAR study.
In our study population, only 21% of patients underwent primary debulking surgery, and a remarkable 43% received no surgery. Median progression-free survival was shortest in patients who received no surgery and longest in patients who underwent primary debulking surgery. One possible explanation for the low proportion of patients with surgery is that only patients ineligible for other clinical trials were enrolled in the OSCAR study, and therefore the population represents a particularly poor-prognosis subgroup. To test this hypothesis, one would need to collect data on all patients treated during the enrollment period. As highlighted by Phillips et al,16 outcomes in patients who do not receive standard therapy are rarely reported, but are typically considerably worse than in populations treated in prospective studies. In a cohort of 593 patients diagnosed with advanced ovarian cancer in a regional cancer center in Birmingham, UK, median overall survival was significantly shorter in the overall population than in patients who underwent surgery (30.2 vs 38.7 months; p<0.001); in patients undergoing primary debulking surgery, median overall survival was 54.5 months.16
The high proportion of patients with no surgery in the OSCAR study contrasts with the ICON7 population, in which all eligible stage III patients had to have primary surgery and only 2% (stage IV) had no surgery,17 perhaps making the replication of median progression-free survival in the OSCAR study more striking. It highlights an urgent need for quality control and improved surgical management of patients with ovarian cancer in the UK. British Gynecological Cancer Society clinical practice guidelines clearly state that the goal in managing advanced epithelial ovarian cancer is complete cytoreduction,18 and the need for specialist surgical training has been emphasized.19 Nevertheless, a recent audit of two gynecologic cancer centers in the UK illustrates the continued variation in surgical practice and its impact on outcomes.20
The main limitations of the OSCAR study are the lack of a control arm, the relatively short duration of follow-up, and the low participation in quality of life assessments, which limits conclusions on the impact of treatment on patients. Major strengths are the relatively large sample size and the inclusion of a patient population representing ‘real-life’ clinical practice, including patients deemed too unfit to receive combination chemotherapy (or surgery) and a substantial proportion of elderly patients. Finally, the consistency with progression-free survival observed with front-line bevacizumab in the high-risk population of the randomized phase III ICON7 trial is noteworthy, confirming the applicability of these results to everyday practice.
Looking ahead, further data on front-line bevacizumab-containing therapy will be generated in the ongoing randomized phase III Medical Research Council ICON8B trial, as well as the control arms of the PAOLA-1 (NCT02477644), ENGOT-ov39/GOG-3015/IMagyn050 (NCT03038100), ENGOT-ov43/BGOG (NCT03740165), and ENGOT-ov46/AGO/DUO-O (NCT03737643) trials.
Acknowledgments
The authors thank the patients who participated in this study and their families, the investigators, the study team from Roche, the clinical operations team, and the biostatisticians. The OSCAR study was sponsored by Roche Products Ltd (Welwyn Garden City, UK). Medical writing assistance was provided by Jennifer Kelly, MA (Medi-Kelsey Ltd), funded by Roche Products Ltd (Welwyn Garden City, UK).
References
Footnotes
Contributors The OSCAR study was designed by the sponsor in collaboration with the first author. All authors except AO treated patients and collected data, which were analyzed by statisticians at SQN, a Contract Research Organisation contracted by Roche Products Ltd. This manuscript was prepared by the first author with support from a medical writer funded by Roche Products Ltd. All authors reviewed subsequent drafts and approved the final version for submission.
Funding This study was funded by Roche Products Ltd.
Competing interests MH has participated in advisory boards for Roche, Tesaro, Clovis Oncology, and AstraZeneca. GB has participated in advisory boards for Roche, Novartis, and Genomic Health. JH has participated in advisory boards for Roche, AstraZeneca, and Tesaro. AO is an employee of Roche. TJP has participated in advisory boards for Roche, Novartis, and Merck Sharp & Dohme Limited and has received travel/accommodation expenses from IGEA Medical. All remaining authors have declared no conflict of interest.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.