Article Text

Abstract
Objective Advances in minimally invasive surgery, particularly with robotic surgery, have resulted in improved peri-operative outcomes in patients with endometrial cancer. In addition, randomized trials have shown that addition of adjuvant radiotherapy following surgery improves loco-regional disease control among stage I intermediate-risk endometrial cancer patients. We aimed to investigate the efficacy and safety of combined treatment of robotic surgery and adjuvant radiotherapy in this patient population.
Methods A single-center retrospective study was conducted on stage I endometrioid-type endometrial cancer patients with intermediate-risk features (<50% myometrial involvement and grade 2–3 histopathology, or >50% myometrial involvement and grade 1–2 histopathology) treated with hysterectomy and adjuvant radiotherapy between January 2010 and December 2015. Data on surgery and radiotherapy were collected and correlated with clinical and surgical outcomes using log-rank. Oncologic outcomes were then compared between robotic surgery and laparotomy.
Results A total of 179 intermediate-risk endometrial cancer patients were identified, of whom 135 (75.4%) received adjuvant radiotherapy and were included in the final analysis. Median age at diagnosis was 63 years (range 40–89) and median follow-up was 4.7 years (range 1.1–8.8). Seventy-seven patients (57%) underwent robotic surgery and 58 patients (43%) underwent laparotomy. Surgical staging with lymph node dissection was performed on 79.3% of the patients. The majority of patients (79.3%) received vaginal brachytherapy as part of adjuvant radiotherapy, while 20.7% received external-beam radiotherapy. Among the entire cohort, eight (5.9%) patients recurred and all eight recurrences occurred in the robotic surgery group; no recurrence was found in the laparotomy group. This translated into 5 year disease-free survival of 100% in the laparotomy group, compared with 91.8% in the robotic surgery group (p=0.005). No difference in overall survival was found between the two groups (p=0.51).
Conclusion Oncologic outcomes for stage I intermediate-risk endometrial cancer treated with hysterectomy and adjuvant radiotherapy at our institution are comparable to the previously published literature. The higher recurrence rate observed with robotic surgery at our institution has not been observed previously and requires further investigation.
- endometrial cancer
- radiotherapy
- robotic surgery
Statistics from Altmetric.com
HIGHLIGHTS
Robotic surgery was associated with a higher recurrence rate than laparotomy in patients with stage I intermediate-risk endometrial cancer.
No difference in 5 year overall survival was seen between robotic surgery and laparotomy.
Adjuvant radiotherapy resulted in loco-regional disease control comparable to historical control.
Introduction
Endometrial cancer is the second most common gynecologic malignancy worldwide1 and the most common in North America.2 3 According to the National Comprehensive Cancer Network (NCCN) guidelines,4 the standard treatment for medically operable patients with endometrial cancer limited to the uterus is total hysterectomy and bilateral salpingo-oophorectomy with consideration for surgical staging, followed by observation, adjuvant radiotherapy, and/or systemic therapy. Multiple studies have demonstrated that, compared with laparotomy, laparoscopic surgery is associated with improvement on peri-operative outcomes, including fewer wound complications, lower blood loss, and shorter hospital stay.5–7 In addition, randomized clinical trials have shown laparoscopy resulted in oncologic survival outcomes similar to laparotomy in endometrial cancers.8 9 Thus, in recent years, the laparoscopic approach has largely replaced laparotomy as the choice of surgical treatment.10 11
Similar to laparoscopy, robotic surgery is increasingly being used to treat patients in both gynecologic and non-gynecologic cancer. Since its introduction and approval by the Food and Drug Administration (FDA) in 2005, studies have shown robotic surgery is associated with improved peri-operative outcomes in surgical treatment of endometrial cancer compared with laparotomy12 and similar oncologic outcomes compared with laparotomy.13 However, a recent Safety Communications from the FDA has raised the issue of safety and effectiveness of robotic surgery in cancer treatment,14 while only a limited number of studies have directly compared long-term oncologic outcomes between robotic surgery and laparotomy to date. In addition, the majority of patients included in the past studies on robotic surgery, including the Gynecologic Oncology Group (GOG) LAP25 and LACE9 trials, had low-risk, as opposed to intermediate-risk, features, where the question of robotic surgery versus laparotomy may not have been truly tested due to the very low recurrence rate in the low-risk group. Furthermore, a recently published study on surgical treatment of early-stage cervical cancer has shown minimally invasive surgery, including robotic surgery, was associated with poorer survival outcomes.15
Multiple randomized trials, including GOG 99 and PORTEC-1, have demonstrated improvement in locoregional disease control with addition of adjuvant radiotherapy following surgical staging in intermediate-risk endometrial cancer.16–19 In addition, the PORTEC-2 study has demonstrated the benefit of using vaginal brachytherapy compared with external beam radiotherapy, in terms of quality of life and toxicity, while achieving similar survival outcomes.20 Since the introduction of robotic surgery in 2005 and publication of the long-term result of PORTEC-2, many patients with intermediate-risk features are now treated with robotic surgery and adjuvant radiotherapy, especially vaginal brachytherapy alone. In this study, we present surgical and clinical outcomes of intermediate-risk endometrial cancer patients treated at our institution with either robotic surgery or laparotomy and adjuvant radiotherapy.
Methods
Institutional Review Board approval was obtained before commencement of the study. A retrospective single-institution chart review was conducted on women 18 years or older with endometrioid-type endometrial cancer with intermediate risk features according to PORTEC-1 criteria17 (<50% myometrial involvement and grade 2–3 histopathology, or >50% myometrial involvement and grade 1–2 histopathology), who had undergone hysterectomy between January 1, 2010 and December 31, 2015 at our institution. The choice of surgery between laparotomy and robotic surgery was left to the discretion of surgeon, while body habitus, inability to assume deep Trendelenburg position, and patient’s preference also contributed to the final decision. Only patients who had received adjuvant radiotherapy were selected for final analysis, as most of the patients who did not receive adjuvant radiotherapy due to various reasons (eg, patient preference, contra-indications to radiotherapy) were discharged from follow-up shortly after surgery, and data on long-term clinical outcomes were not readily available. Patients with high-risk features on surgical pathology, including serous or clear-cell histology, >50% myometrial involvement with grade 3 histopathology, uterine sarcoma, lymph node involvement, and/or International Federation of Gynecology and Obstetrics (FIGO) stage II and higher, were excluded, as they did not meet the inclusion criteria of PORTEC-1. Those with a previous history of pelvic radiotherapy and/or chemotherapy, metastatic disease at presentation, gross positive surgical margin, and history of malignancy within 5 years before diagnosis of endometrial cancer were also excluded.
Patients with limited surgical staging or high risk of lymph node involvement, including grade 3, deep myometrial invasion, and/or positive lymphovascular invasion were treated with external beam radiotherapy, and others were treated with vaginal vault brachytherapy. External beam radiotherapy was delivered to a dose of 45 Gy in 25 fractions over a course of 5 weeks, with a conformal four-field box or intensity-modulated radiotherapy technique. Vaginal vault brachytherapy was delivered with a single line source vaginal cylinder, where the upper 5.0 cm of the vagina was treated to a total dose of 30 Gy delivered in 3 weekly fractions (10 Gy per fraction) prescribed to the surface of the applicator.
All patients included in the study were selected and compared in a concurrent time frame. Data on demographics, histopathology, surgical and radiation treatments, and clinical outcomes on local, regional, and distant recurrences were collected. Intra- and post-operative complications were classified into major and minor categories according to the ACS National Surgical Quality Improvement Project Classification.7
Statistical analysis was performed using International Business Machines Corporation (IBM) Statistical Package for the Social Sciences (SPSS) Statistics 25.0 (Aramonk, NY, USA). Fisher’s exact test was used to compare the rate of peri-operative complications between types of surgery. Survival curves were generated with the Kaplan-Meier method, and the log-rank test was used to calculate 5 year overall survival and disease-free survival and to compare survival rates between robotic surgery and laparotomy. Overall survival was defined as the time interval between pathologic diagnosis with endometrial biopsy and death from any cause, and disease-free survival was defined as time interval between pathologic diagnosis with endometrial biopsy and either radiological, pathologic, or clinical diagnosis of recurrence, whichever occurred first. Both cancer-related and non-cancer-related deaths were censored at time of death for disease-free survival.
Results
A total of 135 patients who received adjuvant radiotherapy were identified (Figure 1) and 14 (10.4%) patients were lost to follow-up. Patient demographics are summarized in Table 1. Median age at diagnosis was 63 years (range 40–89) and median follow-up was 4.7 years (range 1.1–8.8). On surgical pathology, 45.9% of patients had superficial myometrial invasion and 54.1% had deep myometrial invasion. The majority (65.2%) of patients had grade 2, followed by 27.4% with grade 1, and 7.4% with grade 3. Lymphovascular invasion was identified in 23% of patients. In accordance with the PORTEC-1 study,16 61 patients (45.2%) were categorized as high-intermediate risk.
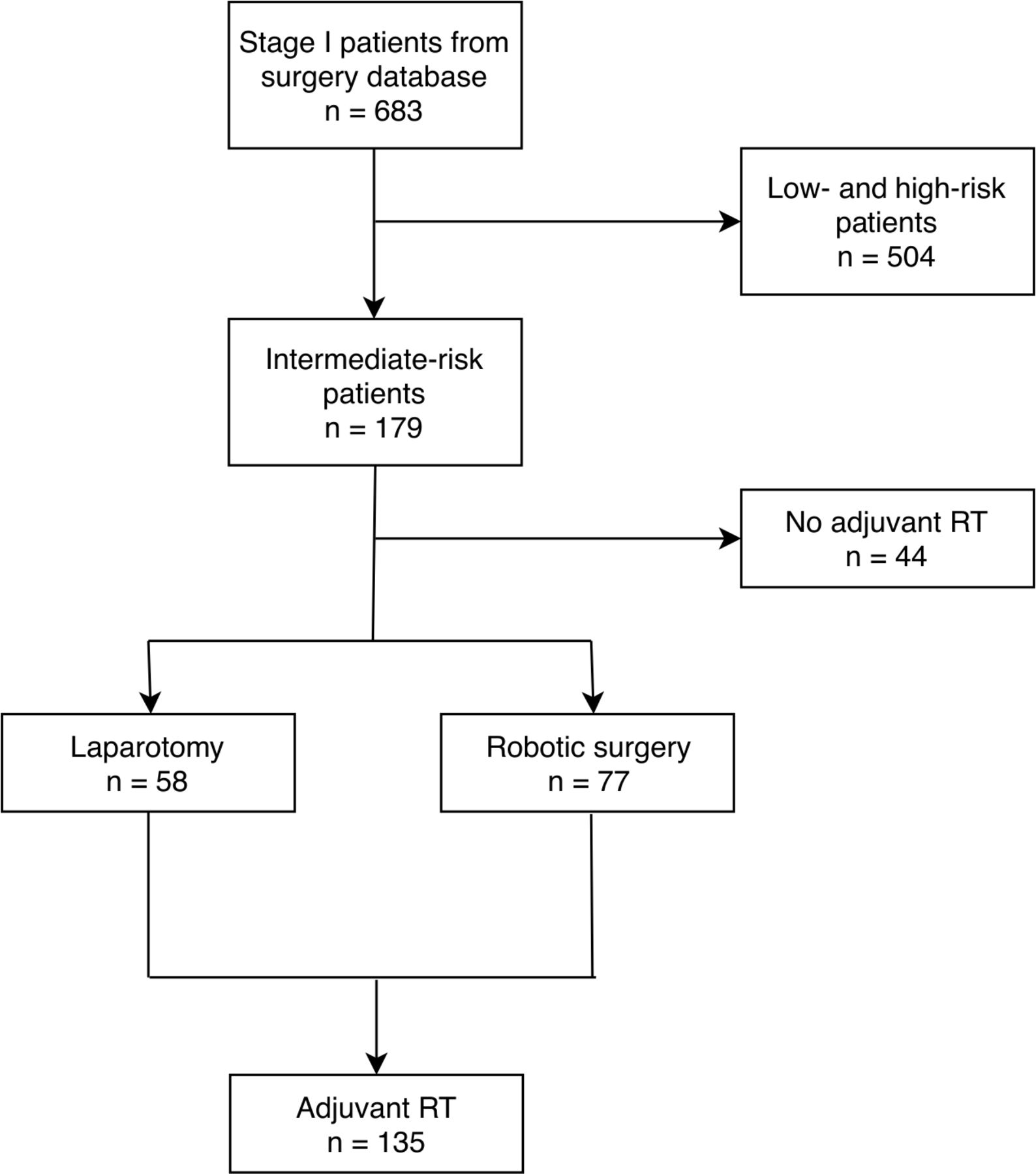
Consort diagram for patient selection. RT, radiotherapy.
Patient baseline characteristics: well balanced between the robotic and laparotomy groups
Among the entire cohort, 77 (57%) patients underwent robotic surgery and 58 (43%) patients underwent laparotomy. Robotic surgery was introduced at our institution in late 2011 and has largely replaced laparotomy since its introduction (Figure 2). Patient demographics, tumor characteristics, and type of adjuvant treatment were similar between the robotic and laparotomy groups: no significant differences were observed between the groups with respect to age, grade, depth of myometrial invasion, lymphovascular invasion, type of adjuvant radiotherapy, number of lymph node sampled, or proportion of high-intermediate risk patients.

Number of surgeries (total and robotic) and recurrences by year of surgery.
Surgical staging with pelvic lymph node dissection was performed on 79.3% of patients and the median number of pelvic lymph nodes sampled was eight (range 1–25). The median interval between surgery and adjuvant radiotherapy was 77 days (range 22–187). The interval between surgery and adjuvant radiotherapy was longer in the robotic group (85 days, range 46–187) compared with the laparotomy group (66 days, range 22–125). The majority (79.3%) of patients received vaginal brachytherapy as adjuvant radiotherapy, while 20.7% of patients received external beam radiotherapy, and no patient received both vaginal brachytherapy and external beam radiotherapy. Two (1.5%) patients with grade 3 and positive lymphovascular invasion received adjuvant systemic therapy in addition to adjuvant radiotherapy.
Eight (5.9%) recurrences were observed among the entire cohort of 135 patients (Table 2). Of the eight recurrences, three (2.2%) were loco-regional (one vaginal and two pelvic) and five (3.7%) were distant recurrences (online supplementary table 1). Median time to recurrence was 2.1 years (range 0.6–5.4). Five year disease-free survival was 95.3% and 5 year overall survival was 95.2% (Figure 3). Of the five (3.7%) deaths observed, two (1.5%) were caused by endometrial cancer.
Supplemental material

{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier survival curve for disease-free survival (a) and overall survival (b). DFS disease-free survival; OS overall survival.
Data showing a higher recurrence rate was observed in the robotic surgery group than the laparotomy group
All of the eight recurrences were in the robotic surgery group (8/77, 11.3%); no recurrences were seen in the laparotomy group (0/58). No difference in 5 year overall survival was found between the two groups (p=0.51), but 5 year disease-free survival was significantly higher in the laparotomy group (100%) than in the robotic group (91.8%) (p=0.005). Similarly, patients with negative lymphovascular invasion had better disease-free survival than those with positive lymphovascular invasion (p=0.039). Other variables, including age, depth of myometrial invasion, grade, lymph node dissection, and type of adjuvant radiotherapy were not associated with a survival difference.
As it pertains to peri-operative complications we identified one (0.7%) intra-operative and six (4.4%) post-operative complications. Among the six cases of post-operative complications, four cases were major (one myocardial infarction, one pulmonary embolism, and two deep wound infections) and two cases were minor (one superficial wound infection and one urinary tract infection). No significant differences in post-operative complications were found between the robotic (2.6%) and laparotomy (6.9%) groups (p=0.46). One patient had a bowel injury intra-operatively during robotic surgery. No death from post-operative complications was identified.
Discussion
Our study demonstrates that surgical and oncologic outcomes in intermediate-risk endometrial cancer patients at our institution treated with either laparotomy or robotic surgery, followed by adjuvant radiotherapy, are comparable to historical controls from the past studies, including GOG9916 and PORTEC-1.17 However, the robotic approach was associated with a higher rate of recurrence than the laparotomy approach. This finding has not been previously reported in this particular intermediate-risk group and, to our knowledge, this is the first series comparing oncologic outcomes of robotic surgery to laparotomy in the same cohort patient population of endometrial cancer.
Peri-operative outcomes from robotic surgery have been extensively studied. A prospective analysis compared 67 robotic surgery cases with previously operated vaginal/laparoscopy (47 cases), laparoscopy (37 cases), and laparotomy (99 cases) approaches; no significant difference in regards to recurrence rates or peri-operative complications was found between the four groups, thus advocating robotic surgery for its association with shorter hospital stay and lower conversion rate to laparotomy, compared with laparoscopy.21 Similar findings have been reported in many other studies.8 22–24 However, only a small number of studies on long-term oncologic outcomes from robotic surgery (excluding laparoscopy) are available. A single-arm study by Brudie et al25 found an acceptable rate of recurrence across all stages of endometrial cancer, with a recurrence rate of 8.0% in the intermediate-risk group during their median follow-up of 31 months. Similar outcomes were demonstrated in another single-arm retrospective study by Kilgore et al.26 A recent systematic review on nine studies by Galaal et al,27 including six randomized clinical trials, found no significant differences in the risk of death or disease recurrence between women who underwent laparotomy and laparoscopy for endometrial cancer.
Interestingly, a recently published phase III LACC trial by Ramirez et al on 631 patients with early stage cervical cancer has shown that minimally invasive surgery (including robotic surgery and laparoscopy) was associated with a significantly lower disease-free survival than laparotomy, and the association persisted even after accounting for multiple variables.15 The patient accrual was terminated early due to the strong association of minimally invasive surgery with higher rates of relapse and death. In their study, patients in the minimally invasive surgery group were not randomized to robotic surgery versus laparoscopy, with the majority (244/289, 84.4%) of patients in the minimally invasive surgery group undergoing laparoscopy. In the post hoc analysis, no difference in disease-free survival was observed between laparoscopy and robotic surgery groups, both showing inferior outcomes compared with laparotomy, but noting that the study was not powered to detect a difference between the laparoscopic versus the robotic approach. Several explanations have been proposed for lower disease-free survival in minimally invasive surgery in their study; the authors have suggested that the routine use of a uterine manipulator in minimally invasive surgery may have potentially increased the risk of tumor spillage. In addition, increased risk of tumor displacement into the peritoneal cavity from carbon dioxide insufflation during robotic surgery has also been suggested as a possible explanation for the observed inferior outcomes.
In our study, the median time interval between surgery and adjuvant radiotherapy was 77 days, longer than those seen in the published literature.28–30 This is largely due to the recent change in practice at our institution to purposely delay adjuvant radiotherapy to 12 weeks following robotic surgery, compared with the 6–8 week interval for laparotomy patients, to prevent vaginal cuff dehiscence, a phenomenon more commonly reported in robotic surgery. The rate of vaginal cuff dehiscence can reach up to 4.1% in robotic surgery, as evidenced by a retrospective study involving 510 patients,31 where thermal effect and vaginal closure technique were cited as potential contributing factors to the higher rate of vaginal dehiscence. Since the introduction of robotic surgery at our institution in 2011, three patients developed vaginal dehiscence within a relatively short period of time, and all had received adjuvant radiotherapy 6–8 weeks after surgery. A decision has been made among gynecologic oncologists and radiation oncologists at our institution to delay adjuvant radiotherapy to provide more time for healing. However, it is not yet known if the delay in adjuvant radiotherapy will actually result in a lower rate of vaginal dehiscence and this requires further investigation.
In our study, a trend towards higher recurrence rate was observed for those whose interval to start adjuvant radiotherapy following hysterectomy was longer than 11 weeks (p=0.083), and a greater proportion (52/77, 67.5%) of patients in the robotic surgery group had intervals longer than 11 weeks, compared with the laparotomy group (14/58, 24.1%) (p<0.001). Previous studies have shown that treatment prolongation and frequent interruptions during treatment have been associated with decreased local control and survival in patients with cervical cancer.32–34 More recently, studies have investigated the association of longer interval between hysterectomy and adjuvant radiotherapy with higher recurrence and worse survival outcomes in endometrial cancer.29–31 Cattaneo et al,28 in their retrospective study involving 309 patients with endometrial cancer, found a strong correlation of higher recurrence rate with treatment delay of greater than 9 weeks, where 5 year recurrence-free survival in the shorter interval (<9 weeks) group was 90%, compared with only 39% in the longer interval (≥9 weeks) group (p<0.001).
Among the 71 patients in our robotic surgery group, eight (11.3%) patients recurred. Historical data from previous studies16 26 27 35 on robotic surgery have shown results of large variation, with recurrence rates ranging from 1.2% in one study, with a short (18 month) median follow-up, to as high as 14.8% in another study (recurrence rates from two other studies were 8.3% and 8.4%). Despite the recurrence rate of 11.3% in our study being similar to that seen in previous studies, this raises concerns for the following reasons. All of the previously cited studies included endometrial cancer patients of all stages, whereas our study population had narrower inclusion criteria with potentially more favorable outcome expectations. Furthermore, only those patients who had received adjuvant radiotherapy were included in our study, further reducing loco-regional relapse. In addition, a large number (66/71, 85.7%) of patients in the robotic surgery group from our study underwent pelvic lymph node dissection, a higher proportion than that seen in similar groups with intermediate-risk features included in other studies17 20 where surgical staging with pelvic lymph node dissection was not required, potentially eliminating patients with stage III disease from our patient population. Taking into consideration all these factors, a recurrence rate of 11.3% observed exclusively in the robotic surgery group in our study raises clinical concerns. In contrast, patients who had undergone laparotomy in our study (n=58) have done very well without any documented recurrence at the time of analysis. It is very possible that the patients in our robotic surgery group have done similarly well compared with those from historical series at other institutions, while improvement in surgical techniques with more modern equipment and specialized practice, as well as better peri-operative care for laparotomy patients, may have led to the difference in oncologic outcomes seen between robotic surgery and laparotomy groups in our study.
Robotic surgery was introduced at our institution in 2011, representing a major transition from laparotomy to robotic surgery. No patient who underwent surgery between 2010 and 2011 recurred, and only after a significant proportion of patients underwent robotic surgery in 2012 did we start to see recurrences (Figure 2). The majority (128/135, 94.8%) of patients were operated on by four of the five gynecologic oncologic surgeons at our institution, and all of the eight recurrent cases were evenly distributed among the four robotic surgeons. In addition, most recurrences were seen within 5 years and our median follow-up period of 4.7 years would be adequate to capture most of the recurrences. Data from other institutions will help determine whether our findings are unique to our center, or more common than previously recognized.
As a result of the findings described above, gynecologic surgeons at our institution are reviewing their surgical techniques, where they are attempting to reduce uterine manipulation during robotic surgery. In addition, patients who have undergone robotic surgery now start adjuvant radiotherapy within 10 weeks, as opposed to 12 weeks, from the date of surgery. More importantly, patients who are deemed to require adjuvant radiotherapy on pre-operative histological and radiological evaluations are no longer treated with robotic surgery. In addition, gynecologic surgeons at our institution have altered their technique of not placing an intrauterine tip with the manipulator, coagulating both fallopian tubes before hysterectomy, and performing a mini-laparotomy for extraction of large uteri. These are designed to minimize tumor spills under the pneumo-peritoneum. However, more mature data are required to evaluate the impact of these changes on recurrence outcomes.
The strengths of the study include the homogeneous population; of all the patients who underwent surgical staging in 2010–2015, only those who received adjuvant radiotherapy following surgery were included in our study, with defined risk criteria that have been validated by the PORTEC-1 study.17 In addition, only a small proportion of patients were lost to follow-up, as most of the patients who have received adjuvant radiotherapy are followed for many years at our institution. On the other hand, the retrospective nature of our study introduces potential bias and confounders. In addition, the relatively small study population (n=135) and number of events (n=8) limit the comprehensive multivariate statistical adjustments for potential confounders.
In conclusion, recurrence rates in stage I, intermediate-risk endometrial cancer patients treated with hysterectomy and adjuvant radiotherapy are comparable to that of the published literature. However, a higher recurrence rate was found in patients treated with robotic surgery compared with laparotomy. Further prospective studies evaluating the significance of our results in this population are necessary.
Supplemental material
References
Footnotes
Correction notice Since this article was first published online, figure 3 and the supplementary table 1 have been updated.
Contributors All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by JS, TL, LH, MF-K-F, KL, MG, CE and RS. The first draft of the manuscript was written by JS and study conceptualization and design were performed by TL and RS. Manuscript review and editing were performed by TL, LH, MF-K-F, KL and MG. Supervision of the study was conducted by RS.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.