Article Text

Abstract
Introduction/Background This is the first study up to date aiming to evaluate different ultrasound features of low and high grade serous epithelial ovarian cancer (LGSC, HGSC). In the histopathology, LGSC contains psammoma bodies more often than HGSC. The formation of psammoma bodies is due to collagen production by neoplastic cells with subsequent calcification.
Methodology This was a retrospective study comprising two cohorts (LGSC and HGSC) of 53 cases each (17 early and 36 advanced stage). Clinical information, ultrasound assessment of primary lesion using IOTA terms and additional ultrasound features of primary tumor and carcinomatosis (hyperechogenic spots, sheet/nodal type and echogenicity of carcinomatosis etc.) were compared.
Results Women with LGSC were younger (mean age 49.0 vs 60.4 years), less often postmenopausal (60 vs 90%), presenting with lower level of CA125 (mean 380 vs 1059 U/mL) and rarer ascites (15 vs 36%). LGSC in comparison to HGSC were often presenting as unilocular-solid lesions (31 vs 2%) with more papillary projections (52 vs 31%), with hyperechogenic appearance of solid tumor components (55 vs 17%) and hyperechogenic peritoneal spread (100 vs 13%) with multiple hyperechogenic spots (74 vs 7%) and shadowing (46 vs 4%) corresponding to the presence of calcified psammoma bodies. In contrast, HGSC were frequently solid (62.5 vs 29%), richly perfused tumors (87 vs 67%) presenting with hypoechogenic peritoneal spread (77 vs 0.0%). All differences were statistically significant.
Conclusion LGSC and its peritoneal spread usually manifest as hyperechogenic (almost white) while HGSC are typically hypoechogenic. The significant difference in tumor and its carcinomatosis appearance contributes to the ultrasound-based tumor-specific preoperative diagnosis and individualized planning of care.
Disclosure This work was supported by Charles University in Prague (UNCE 204065 and PROGRES Q28/LF1) and by a grant from the Czech Research Council (AZV NV19-03-00552).

{kind=link}
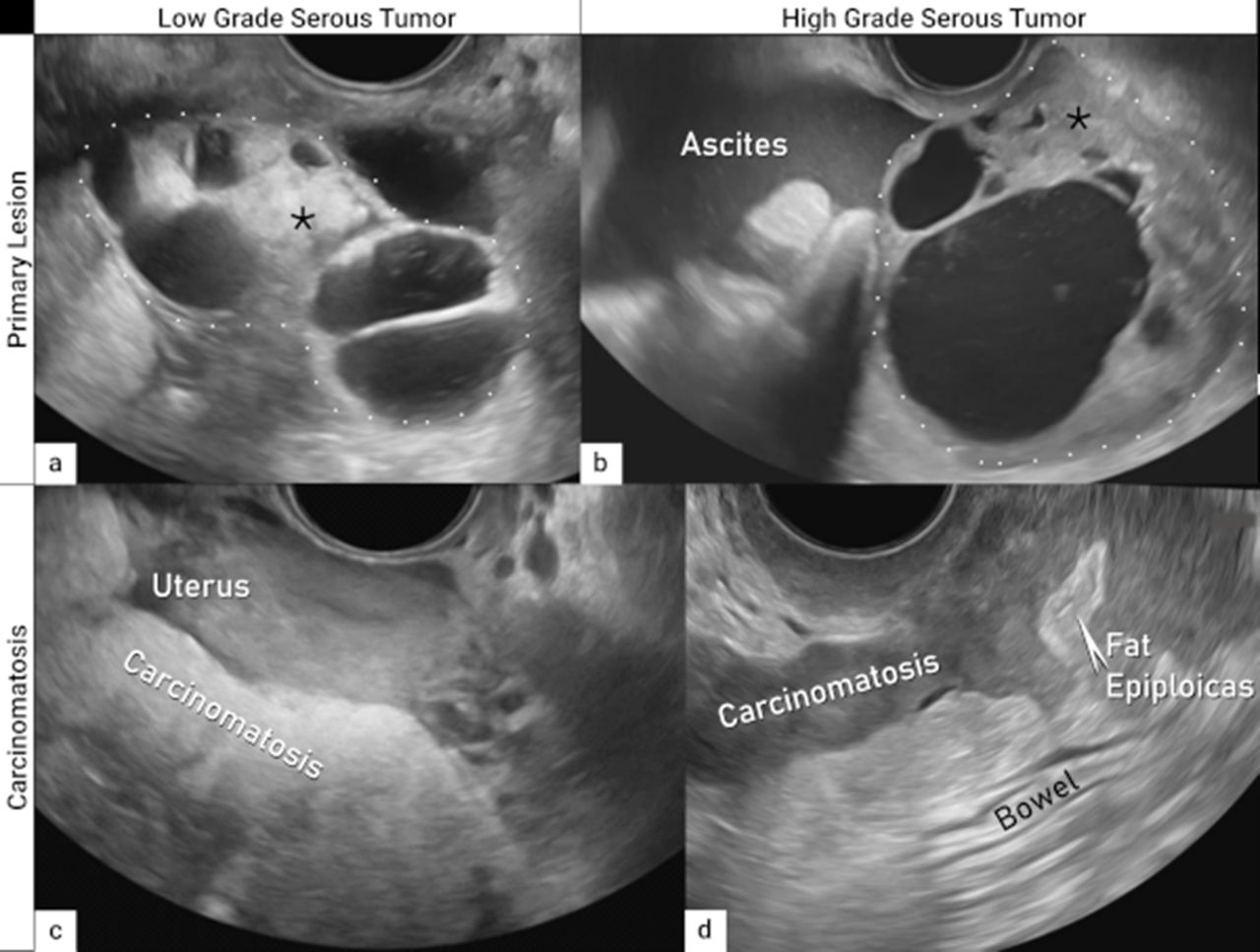
Ultrasound characteristics of LGSC and HGSC (* Solid component of ovarian tumor)